Guidewire passage through metal stent mesh using a novel sphincterotome during the stent-in-stent technique
Shinsuke Akiyama, Takuya Kobayashi, Gensho Tanke, Masaya Wada, Tetsuro Inokuma

Abstract
Click any figure to enlarge with its caption.
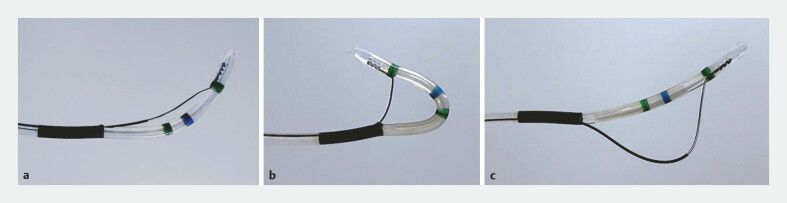 Fig. 1
Fig. 1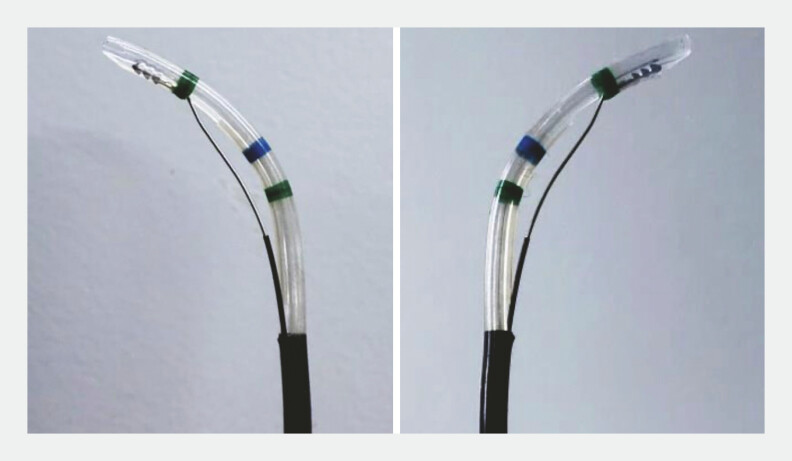 Fig. 2
Fig. 2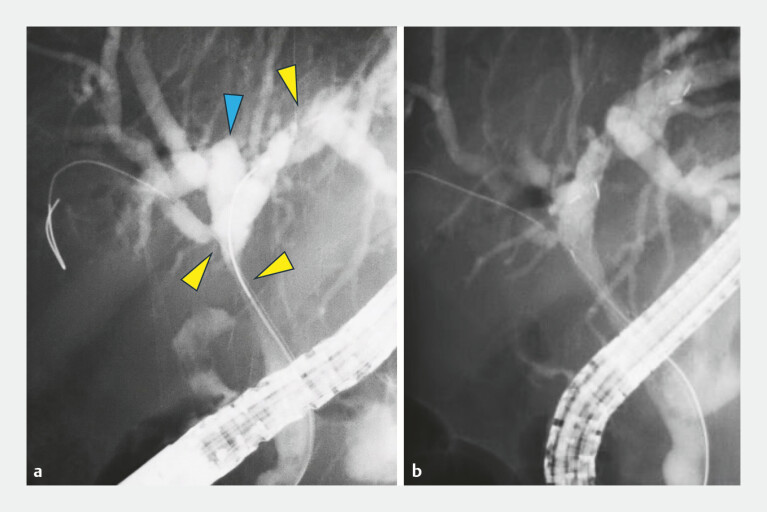 Fig. 3
Fig. 3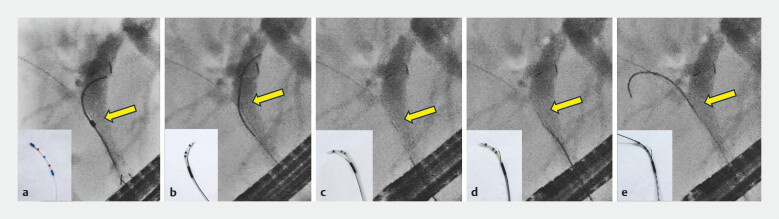 Fig. 4
Fig. 4 Fig. 5
Fig. 5Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGallbladder and Bile Duct Disorders · Aortic aneurysm repair treatments · Coronary Interventions and Diagnostics
The stent-in-stent technique using metal stents is widely employed for the management of perihilar biliary strictures caused by cholangiocarcinoma 1 . However, guidewire passage through the mesh of a previously placed metal stent remains technically challenging when the target bile duct axis is not aligned with the stent lumen 2 . Recently, a novel sphincterotome (ENGETSU; Kaneka Corp., Osaka, Japan) designed for endoscopic sphincterotomy has become available. Owing to its wide range of motion and rotational capability ( Fig. 1 , Fig. 2 ), this device has been reported to be effective for endoscopic sphincterotomy in patients with surgically altered anatomy 3 4 and for selective biliary cannulation, including transpapillary gallbladder drainage 5 . Herein, we report a case in which this sphincterotome facilitated guidewire passage through the stent mesh during the stent-in-stent technique ( Video 1 ).
The novel sphincterotome (ENGETSU; Kaneka Corp., Osaka, Japan) has two cutting functions. a Normal configuration. b Pull configuration. c Push configuration.
The novel sphincterotome also demonstrates superior rotational performance, enabling stepwise 180-degree rotation in both clockwise and counterclockwise directions.
Use of a novel sphincterotome to facilitate guidewire passage through the metal stent mesh during the stent-in-stent technique.Video 1
A 75-year-old man receiving chemotherapy for gallbladder cancer presented with jaundice due to occlusion of a previously placed inner stent. The stent was removed, and endoscopic retrograde cholangiopancreatography (ERCP) revealed multiple strictures involving the common hepatic duct, the origin of the anterior segmental branch, and the left hepatic duct ( Fig. 3 a ). Initially, an uncovered self-expandable metallic stent (8 mm × 8 cm) was deployed into the B2 segment ( Fig. 3 b ). Subsequent attempts to advance a 0.025-inch guidewire through the stent mesh using a standard injection catheter were unsuccessful because of misalignment with the axis of the anterior segmental branch. The catheter was therefore exchanged for the ENGETSU sphincterotome. Under fluoroscopic guidance, counterclockwise rotation combined with a push maneuver enabled successful guidewire passage through the stent mesh into the anterior segmental branch ( Fig. 4 ). Additional stent placement using the stent-in-stent technique was successfully performed, resulting in the resolution of jaundice ( Fig. 5 ).
Fluoroscopic images during biliary metal stent placement using the stent-in-stent technique. a ERCP revealed an irregular stricture extending from the common hepatic duct to the origin of the anterior segmental branch (yellow arrowheads). An abnormality was also noted in the posterior segmental branch, originating from the left hepatic duct (blue arrowhead). b Initially, an uncovered self-expandable metallic stent (8 mm × 8 cm) was deployed into the B2 segment.
Fluoroscopic images demonstrating guidewire passage through the mesh of a previously placed metal stent during the stent-in-stent technique. Yellow arrows indicate the catheter tips of the devices used: a standard injection catheter (MTW Endoskopie Manufaktur, Wesel, Germany) and a novel sphincterotome (ENGETSU; Kaneka Corp., Osaka, Japan). a An initial attempt to advance a 0.025-inch guidewire through the metal stent mesh using the standard injection catheter failed because of misalignment with the axis of the anterior segmental branch. b The standard catheter was exchanged for the ENGETSU sphincterotome, which was initially oriented toward the left hepatic duct. c Under fluoroscopic guidance, counterclockwise rotation was applied to the ENGETSU. d A push maneuver applied to the ENGETSU blade corrected the alignment with the anterior segmental branch. e The guidewire was subsequently advanced successfully through the stent mesh.
A final fluoroscopic view demonstrating successful bilateral metal stent placement using the stent-in-stent technique.
This case highlights the usefulness of a novel sphincterotome for guidewire manipulation through the metal stent mesh in technically challenging stent-in-stent procedures.
Endoscopy_UCTN_Code_TTT_1AR_2AZ
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Lee TH Moon JH Park SH Biliary stenting for hilar malignant biliary obstruction Dig Endosc 20203227528610.1111/den.1354931578770 · doi ↗ · pubmed ↗
- 2Takenaka M Lee TH Kudo M Recent advances in metallic stents used in the stent-in-stent method for hilar malignant biliary obstruction Dig Endosc 20243637037210.1111/den.1468437798137 · doi ↗ · pubmed ↗
- 3Kunogi Y Irisawa A Yamamiya A All-in-one sphincterotome with high rotation performance and freely bendable blade for endoscopic sphincterotomy in patients with surgically altered anatomy (a case series with video)DEN Open 20255 e 7001910.1002/deo 2.7001939386274 PMC 11461899 · doi ↗ · pubmed ↗
- 4Tanisaka Y Ryozawa S Mizuide M Successful endoscopic sphincterotomy using a novel rotatable sphincterotome in a patient with Roux-en-Y gastrectomy Endoscopy 202456 E 1038 E 103910.1055/a-2463-396639592099 PMC 11597894 · doi ↗ · pubmed ↗
- 5Ishikawa T Kumano R Kawashima H Endoscopic transpapillary gallbladder drainage using a novel sphincterotome Dig Endosc 20253729729910.1111/den.1494339438418 PMC 11884956 · doi ↗ · pubmed ↗