New pathways with high-sensitivity cardiac troponin testing at the point of care in the ambulance and primary care
Tonje Rambøll Johannessen, Richard Body, Johannes Mair, Nicholas L Mills, Louise Cullen, Bertil Lindahl, Bertil Lindahl, Jasper Boeddinghaus, Louise Cullen, Lori Daniels, Ola Hammarsten, Kurt Huber, Evangelos Giannitsis, Allan S Jaffe, Dorien M Kimenai, Konstantin A Krychtiuk

TL;DR
This paper explores new care pathways using high-sensitivity cardiac troponin testing in ambulances and primary care to improve outcomes for chest pain patients.
Contribution
The paper introduces pre-hospital point-of-care testing for cardiac troponin to enhance early diagnosis and care for possible myocardial infarction.
Findings
Pre-hospital testing can enable faster diagnosis of myocardial infarction.
Point-of-care testing in ambulances and primary care improves care pathways for chest pain patients.
Early troponin testing supports timely decision-making and resource allocation.
Abstract
Graphical AbstractImproving care with pre-hospital high-sensitivity cardiac troponin testing at the point of care: pathways and considerations. (A) Usual care for patients with chest pain and possible myocardial infarction. (B) Improving care pathways with pre-hospital high-sensitivity cardiac troponin at the point of care in primary care and the ambulance.For image description, please refer to the figure legend and surrounding text. Improving care with pre-hospital high-sensitivity cardiac troponin testing at the point of care: pathways and considerations. (A) Usual care for patients with chest pain and possible myocardial infarction. (B) Improving care pathways with pre-hospital high-sensitivity cardiac troponin at the point of care in primary care and the ambulance.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
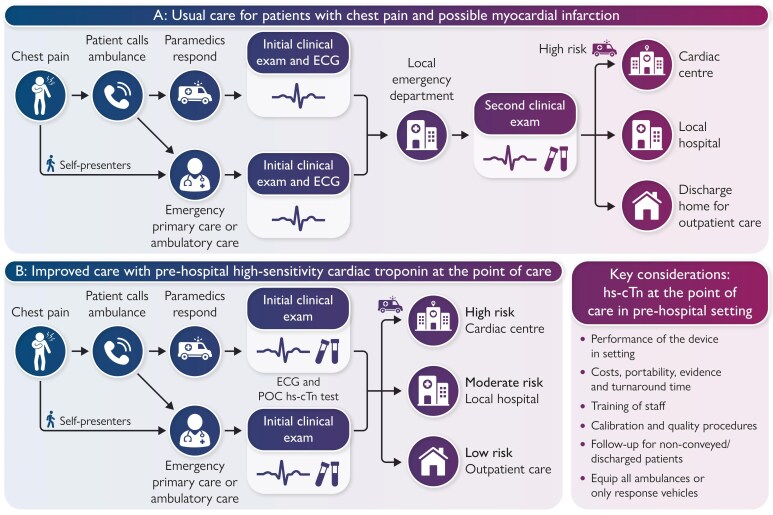 Figure 1
Figure 1- —NIHR Manchester Biomedical Research Centre10.13039/100014653
- —British Heart Foundation10.13039/501100000274
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAcute Myocardial Infarction Research · Cardiac, Anesthesia and Surgical Outcomes · Sepsis Diagnosis and Treatment
Chest pain is one of the most common reasons for emergency ambulance response. If myocardial infarction (MI) is suspected, patients are routinely conveyed to hospital for further investigations, which include one or more high-sensitivity cardiac troponin (hs-cTn) tests to confirm or exclude the diagnosis. In countries with a well-developed primary care network, chest pain is often initially assessed in a community setting. However, as no clinical decision tools can exclude MI without cardiac troponin testing, many patients are transferred to the hospital for further evaluation. With only 1 in 10 patients ultimately diagnosed with MI or an alternative serious condition requiring urgent treatment, the development of hs-cTn testing at the point of care (POC) has major potential to guide clinical decisions in a primary care and pre-hospital setting (Graphical Abstract).^1^
Point-of-care testing in primary care
Chest pain assessment relies on clinical evaluation and an electrocardiogram. While some clinics have access to conventional POC cardiac troponin assays, it is challenging to undertake serial testing in this setting.^2^ In an observational cohort study, patients in Norway were assessed in emergency primary care setting with samples sent to a central laboratory for hs-cTnT testing. The majority were identified as low risk using the ESC 0/1-hour algorithm with a sensitivity of 98.4% and a negative predictive value (NPV) of 99.9%.^3^ The estimated cost saving was €1794 per patient by avoiding an unnecessary hospital admission.^4^ Access to hs-cTn POC testing and use of single-sample rule out pathways in this setting would further improve efficiency and could yield substantial cost reductions.
Point-of-care testing in the ambulance
Point-of-care hs-cTn testing use by ambulance services involves paramedics performing the test at the scene, often in parallel with a 12-lead electrocardiogram during the initial assessment to improve the identification of appropriate patients for transfer. Though the time from symptom onset to testing is shorter in this setting than in an emergency department, hs-cTn testing has excellent sensitivity and NPV for MI when measured at least 3 h from symptom onset.^5^ A recent randomized trial found that prehospital testing with a non-high-sensitivity assay combined with a risk score significantly reduced costs (mean saving €717) with a similar incidence of major adverse cardiac events at 1 year.^6^
Improving care pathways and overcoming logistical challenges
In both settings, POC hs-cTn testing could change care pathways in three ways. First, patients with high probability of MI could be conveyed directly to a cardiac centre for coronary angiography and revascularization, eliminating the need for secondary transfers and expediting specialist treatment. This would be especially beneficial in rural areas. Second, those with very low probability of MI or other serious conditions could be safely left at the scene or sent home from the clinic. Follow-up would need to be provided. Third, stable patients with low probability of MI could be assessed at a Same Day Emergency Care facility or referred to a cardiology outpatient clinic.
Implementation will require logistical challenges to be overcome. Cartridges may require storage in cold bags or refrigerators; cartridges must be at room temperature before testing; charging of the analyser must be guaranteed (power supply needed), paramedic and primary care staff training will be essential; follow-up arrangements must be clear; and when deployed by ambulance services, it is necessary to decide whether to deploy devices on all vehicles or have dedicated POC-enabled response vehicles.
If these challenges can be overcome, the opportunity to re-invent current care pathways with hs-cTn POC testing could provide more efficient, safe, patient-centred, and local care while reducing the burden on crowded EDs and stretched ambulance services.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Cullen L, Mair J, Hammarsten O, Stengaard C, Boeddinghaus J, Daniels LB, et al High-sensitivity point-of-care measurement of cardiac troponin. Eur Heart J;doi:10.1093/eurheartj/ehaf 407. Published online ahead of print 7 August 2025.40795130 · doi ↗ · pubmed ↗
- 2Lindberg BH, Blinkenberg J, Morken T, Allertsen M, Rebnord IK. Diagnostic equipment and point-of-care tests in Norwegian emergency primary healthcare clinics: a cross-sectional study. Scand J Prim Health Care 2025;43:880–889.40537405 10.1080/02813432.2025.2519658 PMC 12632221 · doi ↗ · pubmed ↗
- 3Johannessen TR, Vallersnes OM, Halvorsen S, Larstorp ACK, Mdala I, Atar D. Pre-hospital one-hour troponin in a low-prevalence population of acute coronary syndrome: OUT-ACS study. Open Heart 2020;7:e 001296.32719074 10.1136/openhrt-2020-001296 PMC 7380862 · doi ↗ · pubmed ↗
- 4Johannessen TR, Halvorsen S, Atar D, Munkhaugen J, Nore AK, Wisløff T, et al Cost-effectiveness of a rule-out algorithm of acute myocardial infarction in low-risk patients: emergency primary care versus hospital setting. BMC Health Serv Res 2022;22:1274.36271364 10.1186/s 12913-022-08697-6PMC 9587629 · doi ↗ · pubmed ↗
- 5Lowry MTH, Doudesis D, Boeddinghaus J, Kimenai DM, Bularga A, Taggart C, et al Troponin in early presenters to rule out myocardial infarction. Eur Heart J 2023;44:2846–2858.37350492 10.1093/eurheartj/ehad 376PMC 10406338 · doi ↗ · pubmed ↗
- 6Camaro C, Aarts GWA, Adang EMM, van Hout R, Brok G, Hoare A, et al Rule-out of non-ST-segment elevation acute coronary syndrome by a single, pre-hospital troponin measurement: a randomized trial. Eur Heart J 2023;44:1705–1714.36755110 10.1093/eurheartj/ehad 056PMC 10182886 · doi ↗ · pubmed ↗