Systematic review of the Lancet Commission on Global Surgery indicators with quality assessment of modelled estimates
Theophilus T K Anyomih, Anita E Agbeko, Alazar B Aregawi, Kathryn Chu, Richard Crawford, Ewen M Harrison, Sivesh Kamarajah, Elizabeth Li, John G Meara, Albane Mulliez, Soha Sobhy, Richard Sullivan, Elizabeth Tissingh, Thomas G Weiser, Aneel Bhangu, Dmitri Nepogodiev

TL;DR
This paper reviews global progress on surgical system benchmarks and finds significant gaps in data reporting and quality, especially in low-income countries.
Contribution
The study systematically evaluates the extent to which countries have met surgical system benchmarks and the quality of data used to estimate these metrics.
Findings
Only 39% of countries met the benchmark for access to timely essential surgery.
High-income countries were more likely to meet surgical system benchmarks than low-income countries.
Modelled estimates often lacked transparency and validation, limiting their reliability.
Abstract
The Lancet Commission on Global Surgery (LCoGS) defined six indicators with 2030 targets to track national surgical system performance. The aim of this systematic review was to evaluate national reporting and attainment of benchmarks for each indicator and to assess the quality of modelling studies used to fill data gaps. Seven bibliographic databases (1 April 2015–24 July 2024) and government domains of 48 countries committed to National Surgical, Obstetric, and Anaesthesia Plans were searched. Records providing national estimates of any LCoGS indicator were eligible. The primary outcome was the proportion of World Bank-classified countries meeting indicator benchmarks and the secondary outcome was the quality of modelled national estimates. This systematic review was prospectively registered in PROSPERO, the international prospective register of systematic reviews (CRD420250650890).…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
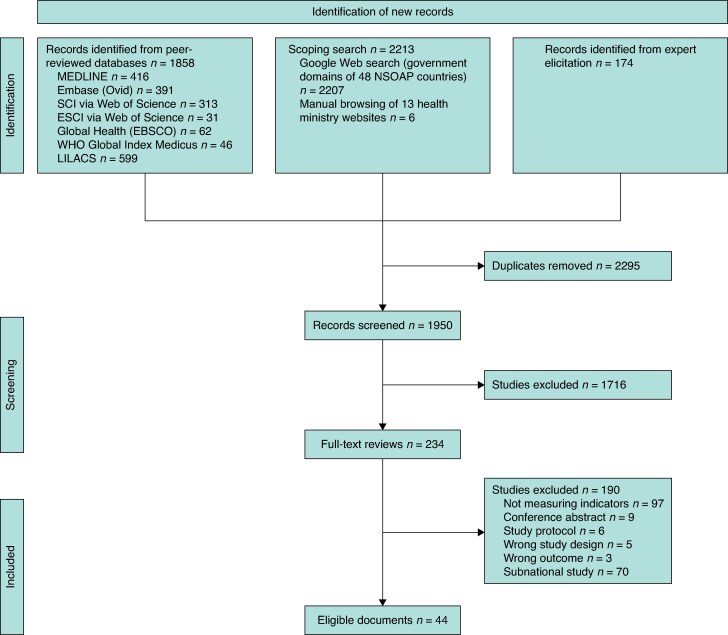 Fig. 1
Fig. 1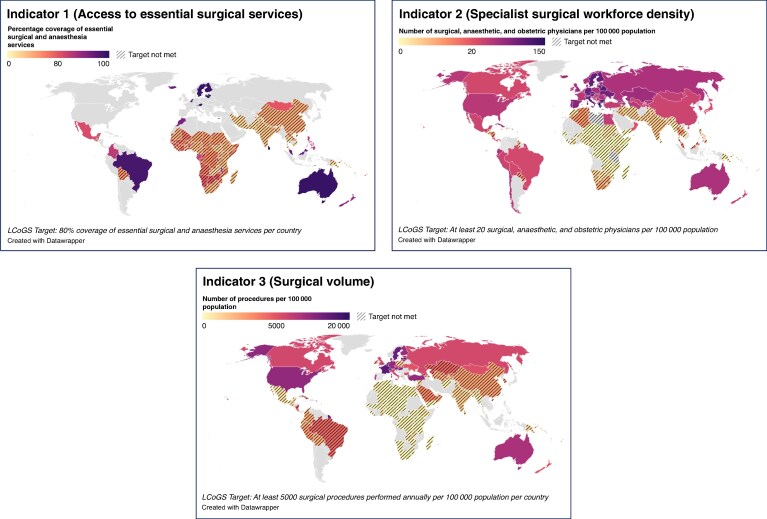 Fig. 2
Fig. 2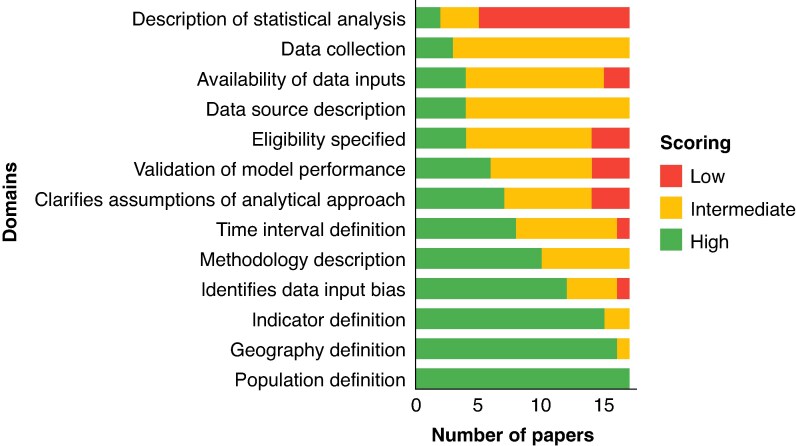 Fig. 3
Fig. 3| Study | Year | Study type | Level | Country/region | Income | Data | Indicators |
|---|---|---|---|---|---|---|---|
| Pérez Rivera | 2024 | Prospective | National | Colombia | UMIC | Observed | 4 |
| Hellar | 2024 | Retrospective | National | Tanzania | LMIC | Observed | 2 |
| Pérez-Soto | 2023 | Retrospective | National | Mexico | UMIC | Modelled | 1–3 |
| Zadey | 2023 | Retrospective | National | India | LMIC | Observed | 3 |
| Cook | 2024 | Retrospective | National | Ethiopia | LIC | Observed | 3 and 4 |
| Qin | 2023 | Prospective | Multinational | Asia/Pacific | UMIC and LMIC | Observed | 2–4 |
| Adde | 2023 | Retrospective | National | Liberia | LIC | Observed | 1 |
| Lim | 2023 | Retrospective | National | Philippines | LMIC | Observed | 1 |
| Samper | 2022 | Retrospective | National | Colombia | UMIC | Observed | 3 and 4 |
| Nunez | 2022 | Retrospective | National | Mongolia | UMIC | Observed | 1–6 |
| Buda | 2022 | Retrospective | National | Guatemala | UMIC | Modelled | 1 |
| Hoh | 2021 | Retrospective | National | Malaysia | UMIC | Observed | 1 |
| Odinkemelu | 2021 | Retrospective | National | Liberia | LIC | Observed | 2 and 3 |
| Pouramin | 2020 | Prospective | Multinational | Multiregional | LMIC and LIC | Observed | 1 |
| Nagra | 2020 | Retrospective | Multinational | Pacific | All | Modelled | 3 and 4 |
| Hanna | 2020 | Retrospective | National | Colombia | UMIC | Observed | 1–4 |
| Wigley | 2020 | Retrospective | Multinational | Sub-Saharan Africa | All | Modelled | 1 |
| Gyedu | 2020 | Retrospective | National | Ghana | LMIC | Modelled | 3 |
| Bouchard | 2020 | Retrospective | Multinational | Multiregional | LIC | Observed | 2 |
| Dahir | 2020 | Retrospective | National | Somaliland | LIC | Observed | 1–3, 5, and 6 |
| van Duinen | 2020 | Prospective | National | Sierra Leone | LIC | Observed | 1 |
| Holmer | 2019 | Retrospective | Multinational | Multiregional | All | Modelled | 1–4 |
| Juran | 2018 | Retrospective | Multinational | Sub-Saharan Africa | LIC, LMIC, and UMIC | Modelled | 1 |
| Ouma | 2018 | Retrospective | Multinational | Sub-Saharan Africa | LIC, LMIC, and UMIC | Modelled | 1 |
| Gyedu | 2018 | Retrospective | National | Ghana | LMIC | Modelled | 3 |
| Biccard | 2018 | Prospective | Multinational | Sub-Saharan Africa | LMIC | Observed | 2–4 |
| Knowlton | 2017 | Retrospective | Multinational | Multiregional | LIC and LMIC | Modelled | 1 |
| Massenburg | 2017 | Retrospective | National | Brazil | UMIC | Modelled | 1–6 |
| Guest | 2017 | Prospective | Multinational | Pacific | All | Modelled | 1–4 |
| Bruno | 2017 | Retrospective | National | Madagascar | LIC | Modelled | 1–6 |
| Stewart | 2016 | Retrospective | National | Ghana | LMIC | Modelled | 1 |
| Esquivel | 2016 | Retrospective | National | Zambia | LIC | Observed | 1 |
| Weiser | 2016 | Retrospective | Multinational | Multiregional | All | Modelled | 3 |
| Alkire | 2015 | Retrospective | Multinational | Multiregional | All | Modelled | 1 |
| Holmer | 2015 | Retrospective | Multinational | Multiregional | All | Modelled | 2 |
| Document title | Year | Level | Country/region | Income | Indicators |
|---|---|---|---|---|---|
| NSOAP for Ghana | 2024 | National | Ghana | LMIC | 1–3 |
| NSOAP for Namibia | 2023 | National | Namibia | UMIC | 2 and 3 |
| National Vision for Surgical Care 2020–2025 | 2021 | National | Pakistan | LMIC | 2 |
| Action Framework for Safe and Affordable Surgery in the Western Pacific Region (2021–2030) | 2021 | Multinational | Pacific | LMIC and LIC | 1 |
| NSOANP for Nigeria | 2019 | National | Nigeria | LMIC | 1–3, 5, and 6 |
| NSOAP for Tanzania | 2018 | National | Tanzania | LIC | 2 and 3 |
| NSOAP for Rwanda | 2018 | National | Rwanda | LIC | 1–4 |
| NSOASP for Zambia | 2017 | National | Zambia | LMIC | 2 and 3 |
| SaLTS Strategic Plan 2016–2020 | 2016 | National | Ethiopia | LIC | 2 and 3 |
| Indicator | Target | Definitions | HIC | UMIC | LMIC | LIC | Total |
|---|---|---|---|---|---|---|---|
| Access to timely essential surgery | A minimum of 80% coverage of essential surgical and anaesthesia services per country by 2030 | Reporting | 20% (17 of 86) | 35% (19 of 54) | 71% (36 of 51) | 85% (22 of 26) | 43.3% (94 of 217) |
| Benchmark met† | 94% (16 of 17) | 47% (9 of 19) | 22% (8 of 36) | 18% (4 of 22) | 39% (37 of 94) | ||
| Serial reporting‡ | 0 | 8 | 20 | 23 | |||
| Specialist surgical workforce density | 100% of countries with at least 20 surgical, anaesthetic, and obstetric physicians per 100 000 population by 2030 | Reporting | 70% (60 of 86) | 87% (47 of 54) | 80% (41 of 51) | 73% (19 of 26) | 77.0% (167 of 217) |
| Benchmark met† | 90% (54 of 60) | 51% (24 of 47) | 15% (6 of 41) | 0% (0 of 19) | 50.3% (84 of 167) | ||
| Serial reporting‡ | 2 | 3 | 2 | 1 | |||
| Surgical volume§ | 80% of countries by 2020 and 100% of countries by 2030 tracking surgical volume | Reporting | 50% (43 of 86) | 57% (31 of 54) | 61% (31 of 51) | 73% (19 of 26) | 57.1% (124 of 217) |
| 5000 procedures per 100 000 population by 2030 | Benchmark met† | 77% (33 of 43) | 19% (6 of 31) | 0% (0 of 31) | 0% (0 of 19) | 31.5% (39/124) | |
| Serial reporting‡ | 0 | 6 | 3 | 2 | |||
| Perioperative mortality§# | 80% of countries by 2020 and 100% of countries by 2030 tracking perioperative mortality | Reporting | 20% (17 of 86) | 43% (23 of 54) | 37% (19 of 51) | 58% (15 of 26) | 34.1% (74/217) |
| In 2020, assess global data and set national targets for 2030 | Not reported | ||||||
| Financial risk protection against impoverishing expenditure | 100% protection against impoverishment from out-of-pocket payments for surgical and anaesthesia care by 2030 | Reporting | 0% (0 of 86) | 4% (2 of 54) | 2% (1 of 51) | 8% (2 of 26) | 2.3% (5 of 217) |
| Benchmark met† | Not reported | 0% (0 of 2)† | 0% (0 of 1) | 0% (0 of 2) | 0 | ||
| Serial reporting‡ | Not reported | 0 | 0 | 0 | |||
| Financial risk protection against catastrophic expenditure | 100% protection against catastrophic expenditure from out-of-pocket payments for surgical and anaesthesia care by 2030 | Reporting | 0% (0/86) | 4% (2 of 54) | 2% (1 of 51) | 8% (2 of 26) | 2.3% (5 of 217) |
| Benchmark met† | Not reported | 0% (0 of 2)† | 0% (0 of 1) | 0% (0 of 2) | 0 | ||
| Serial reporting‡ | Not reported | 0 | 0 | 0 | |||
| Domain | Quality | ||
|---|---|---|---|
| Low | Intermediate | High | |
|
| |||
| 1. Provide a clear definition of the Lancet Commission indicator(s) used | No explicit definition | Definition used is slightly different to the ones used in the Lancet Commission indicators | Provides a clear definition of the indicators used, similar to the Lancet Commission indicators |
| 2. Provide a clear definition of the target population for which the modelling analysis is applicable to | No description of the population | There is a vague definition of the population (that is age or sex) or patients included in the study | Clear definition including what procedures are included and excluded |
| 3. Clear definition of the geography studied | No definitions of the scale of country or regions included | Clear definition of region covered but have had to model some of the data or have incomplete data for the region | Clearly defined catchment (for example province or state-level or national-level analysis) with complete population data |
| 4. Clear definition of the time interval | Not defined | Poorly defined | Clearly defined |
|
| |||
| 5. Description of methodology | Minimal or no description of methodology | Clearly described in text | Clearly described with conceptual overview (for example flow chart or diagram) and including mathematical formulae/statistical code if applicable |
| 6. Methodology of how underlying data were collected | No description of the nature of data collection for the inputs reported in the study | Data inputs obtained were retrospective in nature including administrative data, with high risk of potential biases | Data inputs were prospectively collected, either from cohort studies or RCTs |
| 7. Specify the inclusion and exclusion criteria | No clear specification around inclusion or exclusion criteria for the data source(s) being used | Partial specification around inclusion or exclusion criteria for the data source(s) being used | Full specification around inclusion or exclusion criteria for the data source(s) being used |
| 8. Description of data source characteristics | No information on data source or characteristics | Provides information on all included data sources and their main characteristics. | Provides information on all included data sources and their main characteristics and identifies and describes any categories of input data that have potentially important biases |
| 9. Availability of data inputs | Not available | Data sources clearly referenced but data not provided or contacts of rights to data not provided | Provides all data inputs (including all relevant meta-data) in an extractable file format; make these available as a supplementary file, or via a clearly identified contact/data custodian who retains the rights to the data |
| 10. Description of statistical analysis | Minimal or no description of statistical analysis | Clearly described in text but no statistical or mathematical code provided or how they can be assessed | Detailed description of all steps of the analysis (data cleaning, data preprocessing, data adjustments, and |
| 11. Validation of model performance | No attempt to validate the model | Attempt to validate the underlying methodology | Attempt to validate modelled data against observed data and detailed description of how validation was done |
|
| |||
| 12. Identification of potential biases relating to data inputs | Not performed | Biases identified but their potential impact on findings not discussed | Biases identified and their potential impact on findings discussed |
| 13. Identification of assumptions within analytical approach | Not performed | Assumptions identified but their potential impact on findings not discussed | Assumptions identified and their potential impact on findings discussed |
- —National Institute for Health and Care Research (NIHR) Global Health Research Unit10.13039/100018336
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGlobal Health and Surgery · Global Maternal and Child Health · Global Health Workforce Issues
Introduction
Strengthening surgical systems is recognized as a core component of universal health coverage (UHC) and health system resilience^1^. The 2015 Lancet Commission on Global Surgery (LCoGS) proposed six indicators: access to timely essential surgery (indicator 1), specialist surgical workforce density (indicator 2), surgical volume (indicator 3), perioperative mortality (indicator 4), financial risk protection against impoverishing expenditure (indicator 5), and financial risk protection against catastrophic expenditure (indicator 6)^2,3^. The Commission set targets for 2030 for each indicator to guide policy, financing, and research, drawing on learning from the WHO Safe Surgery Saves Lives programmes^4^. A subsequent consensus process merged the two financial indicators creating a streamlined framework of five indicators to improve transparency and utility^5^. Despite this, in this review, the two financial indicators are reported separately to retain comparability with previous LCoGS publications and the existing literature.
Despite global endorsement, and inclusion of four indicators (workforce, volume, and the two financial indicators) in the World Bank’s World Development Indicator (WDI) data set, national reporting remains inconsistent^6–8^. Most countries do not routinely publish these indicators and only a handful track them longitudinally^9^. This limits the ability to monitor progress toward achieving the LCoGS benchmarks^10^. These gaps are most marked in low-income countries (LICs) and lower middle-income countries (LMICs), where reliance on modelled estimates is common due to the absence of primary data^11,12^. Although modelling can fill information gaps, the quality and transparency of these estimates have not been systematically appraised.
Previous reviews have summarized indicator availability and achievement, but none has assessed both the completeness of reporting and the quality of modelled data at the national level^13–15^. Without robust, standardized, and repeatable reporting mechanisms, progress towards the LCoGS benchmarks cannot be reliably measured and surgical system strengthening risks being overlooked in UHC monitoring frameworks.
The aim of this study was to determine the extent of national reporting and benchmark attainment for each LCoGS indicator since 2015 and to evaluate the methodological quality of modelling studies used to generate national estimates.
Methods
Study design and reporting
This systematic review is reported according to the PRISMA 2020 guidelines^16^ and was prospectively registered in PROSPERO, the international prospective register of systematic reviews (CRD420250650890).
Bibliographic database search
Seven databases were searched for English-language articles published from 1 April 2015 to 24 July 2024: MEDLINE, Embase (Ovid), Global Health (EBSCO), Science Citation Index (SCI) and Emerging Sources Citation Index (ESCI) via Web of Science, WHO Global Index Medicus, and Latin American and Caribbean Health Sciences Literature (LILACS). Search strategies combined controlled vocabulary (for example Medical Subject Heading (MeSH) terms for MEDLINE) and free-text terms for each indicator (Table S1). The database search was last updated on 17 March 2025; however, because the inclusion window ended on 24 July 2024, these 2025 updates did not identify any additional eligible records. Reference lists of included papers were screened and additional records were identified via expert consultation. Search results were deduplicated in EndNote and imported into Covidence for screening.
Scoping search
To capture relevant policy documents commonly reported in government sources, a targeted web search was conducted on 24 June 2025. A Google Web search was conducted, restricted to government domains of 48 countries that have developed or committed to a National Surgical, Obstetric, and Anaesthesia Plan (NSOAP). Additionally, the health ministry websites of 13 of those countries with an NSOAP in active implementation were manually screened^17^. Structured queries combined indicator synonyms, policy document terms, and file type filters, while excluding academic domains. Details of search strings and domain blocks are available in Supplementary Methods, Table S2, S3. Search results were exported as csv, deduplicated in Excel, and screened.
Eligibility criteria
Records were included if they reported on at least one LCoGS indicator at a national level and were published between 1 April 2015 and 24 July 2024. Reviews, non-English publications, subnational studies, and documents without numerical indicator data were excluded. Conference abstracts were not included due to lacking the details or methodological rigour necessary for reporting and decision-making. Unanalysed raw data sets were also not included as the time and specialist capacity required to process such data renders them an unrealistic basis for routine reporting by researchers or policymakers.
Selection process
Titles/abstracts (or first pages) were screened independently by two reviewers (T.T.K.A. and A.M.). An initial calibration set of 100 records achieved ≥95% agreement; thereafter dual screening was applied to all remaining records. Full-text review followed the same procedure, with disagreements resolved by consensus or, if required, a third reviewer (D.N.).
Data extraction and management
Data extraction was performed independently by two reviewers (T.T.K.A. and A.M.) using a standardized spreadsheet. Extracted fields included study metadata (author, country, and year), data level (national or multinational), indicator(s) reported, indicator values, data source/method (observed or modelled), and benchmark achievement status. For each indicator, results were stratified by World Bank income group^18^. Studies reporting modelled estimates were flagged for quality assessment. Extracted values were compared directly against the benchmark thresholds defined by the LCoGS to determine whether countries had achieved each target. Table S4 outlines the indicators and corresponding benchmarks.
Outcome definitions
The primary outcome was the proportion of World Bank-classified countries, stratified by income group, meeting the LCoGS targets.
For each indicator, the number and/or proportion of all 217 World Bank-classified countries^18^ that reported the indicator at least once, that achieved the benchmark, and that reported data more than once (serial reporting) were determined. For the purposes of this review, an indicator was considered ‘reported’ if any numerical value of the indicator was presented for a country, irrespective of whether the benchmark was met. An indicator was considered ‘achieved’ if the reported estimate met or exceeded the benchmark target defined by the LCoGS (Table S4). Where multiple data points were available for a country, the most recent estimate was used for the primary benchmark analysis. In instances where multiple data points were reported for the same time interval, selection was guided by a predefined hierarchy: prospective over retrospective design, observed over modelled data, and recency. Countries with two or more published estimates were classified as having serial reporting.
Development of a quality assessment tool
Given the increasing reliance on modelled estimates in global surgical metrics, a structured evaluation of the methodological quality of such studies was warranted. To objectively evaluate the quality of studies reporting modelled estimates of LCoGS indicators and identify gaps for improvement, a quality assessment tool was developed based on the original 18-item Guidelines for Accurate and Transparent Health Estimates Reporting (GATHER) statement^19^, which was adapted to suit the indicators (Table S5). The GATHER statement outlines essential items for reporting modelled data, including disclosure of data sources, assumptions, and methods. Adherence to these principles enhances the interpretability and credibility of estimates, particularly when they are used to guide policy or investment decisions. The initial draft comprising 18 domains was grouped under four thematic sections: objectives, methodology, interpretation, and conflict of interest. Each item was scored on a three-point ordinal scale (low, intermediate, and high) based on predefined criteria reflecting completeness and transparency (Table S6).
Expert consultation
The draft tool was refined via a structured online consultation with 15 international experts in surgical systems and health metrics, purposively selected to ensure representation across diverse geographical regions and income settings. Each participant rated the importance of the 18 proposed domains using a five-point Likert scale (1 = not important to 5 = very important). Domains were retained if ≥60% of respondents rated them as four or five. Participants were also invited to provide qualitative feedback on wording, clarity, and interpretation, which was used to inform the final version of the tool. Participation was voluntary and anonymous, and the consultation was conducted in a single round. This approach enabled the identification of key domains deemed essential by the expert panel and informed the final version of the assessment tool.
Data analysis
Descriptive statistics are used to summarize the number and proportion of all 217 World Bank-classified countries^18^ reporting and achieving each LCoGS indicator benchmark. Results are stratified by income group. Meta-analysis was not undertaken due to substantial heterogeneity in data sources, study design, and reporting time frames across included studies.
Results
Study selection and characteristics
Comprehensive searches retrieved 4245 records (1858 from bibliographic databases, 2213 from the scoping search, and 174 through expert elicitation; Fig. 1). After removal of 2295 duplicates, 1950 records were screened, 234 underwent full-text review, and 44 records met the inclusion criteria: 35 peer-reviewed studies^10,20–53^ and 9 government policy documents^54–62^. Of the 44 included studies, 29 were national-level studies^20–24,26–30,33,35,37,38,40,43,45–47,51,53–62^, 6 used prospective data^20,25,31,38,41,44^, and 17 relied on modelled estimates for at least one indicator^10,22,28,32,34,35,39,40,42–46,48–50,52^. Only five studies^27,33,43–45^ reported on all six indicators (Table 1 and Table 2).
PRISMA flow diagram summarizing study selection, including the number of records identified, screened, assessed for eligibility, and included in the final systematic reviewSCI, Science Citation Index; ESCI, Emerging Sources Citation Index; LILACS, Latin American and Caribbean Health Sciences Literature; NSOAP, National Surgical, Obstetric, and Anaesthesia Plan.
Indicator reporting and benchmark attainment
Access to timely essential surgery (indicator 1) was reported by 94 countries (17 high-income countries (HICs), 19 upper middle-income countries (UMICs), 36 LMICs, and 22 LICs) representing 43.3% (94 of 217) of all World Bank-classified countries. Benchmark achievement (≥80% population coverage within 2 h) was highest in HICs (94% (16 of 17)), followed by UMICs (47% (9 of 19)), LMICs (22% (8 of 36)), and LICs (18% (4 of 22)). Serial reporting was identified in 51 countries (8 UMICs, 20 LMICs, 23 LICs, and 0 HICs).
Specialist surgical workforce density (indicator 2) was the most reported indicator with data from 167 countries (60 HICs, 47 UMICs, 41 LMICs, and 19 LICs) representing 77.0% (167 of 217) of all countries. No LICs met the workforce target of ≥20 surgical, anaesthetic, and obstetric providers per 100 000 population. The proportion meeting the benchmark was highest in HICs (90% (54 of 60)), followed by UMICs (51% (24 of 47)) and LMICs (15% (6 of 41)). Only eight countries provided more than one estimate over time.
Surgical volume (indicator 3) was reported by 124 countries (43 HICs, 31 UMICs, 31 LMICs, and 19 LICs) covering 57.1% (124 of 217) of all countries. No LMICs or LICs met the target of ≥5000 procedures per 100 000 population. The benchmark was met by most HICs (77% (33 of 43)) and a few UMICs (19% (6 of 31)). Repeated reporting was observed in 11 countries.
Perioperative mortality (indicator 4) was reported at least once by 74 countries (17 HICs, 23 UMICs, 19 LMICs, and 15 LICs) representing 34.1% (74 of 217) of all countries. No benchmark was set at country level. The commission set a global target for universal tracking at a national level by all countries.
Financial risk protection indicators (indicators 5 and 6) were the least reported, with only 2.3% (5 of 217) of countries providing any data. Of these, two were UMICs, one was a LMIC, and two were LICs. No HICs reported data on either indicator. None of the five countries met the targets of 100% financial risk protection against impoverishing expenditure and 100% financial risk protection against catastrophic expenditure (see Fig. 2 and Table 3).
World maps showing country-level attainment of LCoGS benchmarks a For indicator one (access to timely essential surgery). b For indicator two (specialist surgical workforce density). c For indicator three (surgical volume). Countries are classified as meeting the benchmark, not meeting the benchmark, or having no available data. Indicators four–six are not shown. Indicator four (perioperative mortality) was excluded as the LCoGS target applies at a global level rather than to individual countries. Indicators five and six (financial risk protection) were excluded due to limited reporting (only five countries had available data) precluding meaningful global visualization. LCoGS, Lancet Commission on Global Surgery.
Quality of modelling studies
After the expert consultation process, five domains (7, 8, 14, 15, and 18) were excluded based on failing to meet the predefined threshold of ≥60% of experts rating them as ‘important’ or ‘very important’. The final version of the quality assessment tool included 13 domains, grouped into three thematic sections, and is summarized in Table 4. Seventeen studies^10,22,28,32,34,35,39,40,42–46,48–50,52^ were assessed for quality using the final tool. Four studies had at least 8 of 13 domains rated as high quality. Performance across domains was variable. Objectives and context of modelling were generally well described, with most studies scoring ‘high’ for clearly defining the indicator (domain 1) (16 of 17 studies (94%)), target population (domain 2) (17 of 17 studies (100%)), and geographical scope (domain 3) (16 of 17 studies (94%)). Definitions of the time interval (domain 4) (8 of 17 studies (47%)) and modelling methodology (domain 5) (9 of 17 studies (53%)) were more inconsistently reported. Data sources and transparency were generally weak. Only 18% of studies (3 of 17) described prospective input data sources (domain 6). Inclusion and exclusion criteria, data source characteristics, and metadata availability (domains 7–9) were each rated ‘high’ in only 4 of 17 (24%) studies. Just 6 of 17 studies (35%) described all steps in model construction (domain 10) and only 2 of 17 studies (12%) performed any form of validation against observed data (domain 11). Potential biases (domain 12) were explicitly discussed in 11 of 17 studies (65%), while assumptions (domain 13) were clearly identified and explored in 7 of 17 studies (41%). Overall, while reporting on scope and intent was relatively strong, method transparency and quality assurance measures were frequently lacking (Fig. 3).
Domain-level quality ratings (for domain 1 to domain 13) for the modelled studies included in the reviewBars show the proportion of studies scoring high, intermediate, or low quality for each domain according to the final quality assessment tool.
Discussion
Across 217 World Bank-classified countries, fewer than half have ever published an estimate for timely access to essential surgery, only one-third have reported a perioperative mortality rate, and financial risk protection has only been documented in five countries. Benchmark attainment mirrors this data gap: almost all HICs meet the access target, yet no LIC reaches the workforce and surgical volume benchmarks. Repeated reporting is rare, limiting the ability to monitor change over time. Although modelling studies attempt to bridge these gaps, their transparency, reproducibility, and methodological rigour are often suboptimal.
Despite endorsement by global bodies and inclusion in the WDI data set in 2016, reporting of LCoGS indicators fell in 2023^6,7^. This has been attributed to barriers such as underdeveloped data infrastructure, fragmented care delivery, and lack of investment, particularly in LMICs/LICs^64^ ^,65^. Within countries, weak multisectoral coordination and variable case mix further inhibit the integration of these indicators into routine health information systems^11^. By contrast, other domains of global health, such as maternal and neonatal health and infectious disease programmes, use standardized indicator frameworks that facilitate consistent tracking and measurable gains^66–68^. Of all six indicators, indicator one (access to timely essential surgery) is among the most difficult to assess globally. In high-income settings, near-universal hospital coverage means travel times are routinely below 2 h but are rarely reported as surgical metrics. Instead, access data are embedded within broader infrastructure or emergency-care statistics. Consequently, reporting for this indicator is concentrated in LMICs, where modelling is often used to quantify deficits, while in HICs its absence reflects reporting priorities. Although HICs are generally assumed to have adequate geographical coverage, this does not preclude substantial subnational inequities in access for different population groups^69–72^. There is a need for HICs to generate and publish granular data on access to essential surgical care. Strengthening frameworks for data collection in global surgery will enhance reporting, enable benchmarking of progress, and identify areas requiring intervention.
Benchmark achievement was highly variable and mirrored human development index levels. While nearly all HICs met the surgical workforce density target, none of the LICs achieved this benchmark. In addition, the surgical volume benchmark was not met by any LMIC or LIC. Financial risk protection indicators were the least reported and none of the five countries with available data met the 100% coverage target. These findings are consistent with previous estimates and underscore both the lack of data systems and the absence of formal mechanisms to support indicator-based benchmarking in global surgery^3,10,73^. Without reliable denominators and repeated measurement, benchmarking becomes a theoretical exercise rather than a tool for accountability. The availability of disaggregated, country-level data has also supported subnational accountability and enabled targeted improvements. Within surgery for instance, national-level audit programmes such as the UK’s National Emergency Laparotomy Audit (NELA), Dutch Institute for Clinical Auditing (DICA), and the US National Surgical Quality Improvement Program (NSQIP) have demonstrated that structured indicator tracking can improve outcomes^74–77^. NELA has been associated with reductions in postoperative mortality and has enhanced accountability by providing regular feedback to hospitals and clinicians^78^. In contrast, the global surgical field lacks an equivalent mechanism for standardized indicator tracking, which undermines accountability and inhibits system-wide improvement.
In the absence of primary data, modelled estimates have gained prominence^13–15^. Yet, as this review shows, the quality of modelling studies varies considerably. Of the 16 studies assessed, only 4 met high-quality criteria in ≥8 of 13 domains. While the majority clearly defined their objectives and target populations, most studies failed to report data inputs transparently or describe their analytical methods in sufficient detail. Less than a third acknowledged assumptions or uncertainty, and only 25% validated their models against observed data. These deficiencies limit the interpretability and applicability of modelling outputs for national planning or international comparison.
This review addresses an important evidence gap by consolidating national-level reporting across all six LCoGS indicators worldwide and screening of government domains of 48 NSOAP countries while applying a novel quality appraisal tool for modelling studies. The protocol was prospectively registered and duplicate screening and extraction ensured methodological rigour. However, there were some limitations. First, although data from non-published sources (including governmental reports and policy documents) was searched for and incorporated, pre-prints, conference abstracts, and unanalysed databases, which may contain relevant data, were excluded. Second, the scoping search was confined to government domains of 48 countries committed to NSOAP development, potentially overlooking records from non-NSOAP countries. Some national surgical plans and related policy documents may exist but are not publicly available or may have limited discoverability through open-source searches. For example, Ecuador’s National Surgical Strategic Plan (NSSP) is known to exist but is not readily accessible^79^. This highlights a need for health ministries to ensure national reporting systems are transparent and publicly available. Third, the academic literature is largely skewed towards LMICs and may under-represent reporting from HICs, where data are often collected and stored through systems such as the Organisation for Economic Co-operation and Development (OECD), Demographic and Health Surveys (DHS), or the Healthcare Cost and Utilization Project (HCUP)^80–82^, which were outside the remit of this review. Fourth, heterogeneity in data sources, time frames, and health system structures limited direct comparisons across countries and reliable cross-national typologies for financing and expenditure remain uneven. Fifth, reporting remains sparse, especially in LICs, leading to potential under-representation of some settings. Finally, the restriction to English-language publications may have excluded evidence from non-English-speaking regions. This reflects a broader structural bias in global health research, where English-language dominance can obscure substantial data published in other major languages. To improve equity and completeness, future reviews should include multilingual search strategies or follow-up studies in major languages to make global surgery evidence truly global. Future studies could examine how indicator reporting and achievement vary by health system model and national health expenditure. Mapping countries by financing type and spending levels could reveal which system structures most support robust surgical metrics and financial risk protection.
Surgical indicators remain disconnected from institutionalized reporting infrastructure that gives other global health fields visibility and therefore priority. Without routine collection and reporting, surgical need is excluded from UHC benefit packages, official development assistance (ODA) allocations, and sustainable development goal (SDG) progress reviews. This invisibility perpetuates a cycle of marginalization, limiting both domestic investment and external financing for surgical care.
By contrast, maternal and newborn health programmes have advanced through coordinated indicator frameworks, dedicated financing, and regularized data collection using platforms such as DHS and Multiple Indicator Cluster Surveys (MICS). These models are transferable. Surgery does not require a new system from scratch but rather integration into proven mechanisms. The challenge is mainly structural: the absence of a unified framework continues to undermine policy action and resource allocation in this complex, high-cost area.
Embedding surgical indicators into national health information systems is essential. Existing platforms such as District Health Information Software 2 (DHIS2)—used by over 80 countries—and the WHO Operative Encounter Registry (OER) offer practical infrastructure for integrating surgical metrics^83,84^. These should be aligned with global standards on indicator definitions, thresholds, and reporting cycles. WHO must provide normative leadership by standardizing indicators and establishing minimum reporting cycles, while multilateral development banks (MDBs) should provide financing on the condition of reliable reporting. Bilateral funders should support data system investments that enable surgical metrics to be tracked alongside UHC indicators. These reforms would close visibility gaps, enable LMIC-led priority setting, and foster equity, transparency, and accountability in surgical system strengthening.
Supplementary Material
znaf289_Supplementary_Data
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Price R, Makasa E, Hollands M. World Health Assembly resolution WHA 68.15: “strengthening emergency and essential surgical care and anesthesia as a component of universal health coverage”—addressing the public health gaps arising from lack of safe, affordable and accessible surgical and anesthetic services. World J Surg 2015;39:2115–2526239773 10.1007/s 00268-015-3153-y · doi ↗ · pubmed ↗
- 2Das P, Horton R. Disease Control Priorities, 3rd edition—from theory to practice. Lancet 2018;391:e 9–e 1029221644 10.1016/S 0140-6736(17)32905-7 · doi ↗ · pubmed ↗
- 3Meara JG, Leather AJM, Hagander L, Alkire BC, Alonso N, Ameh EA et al Global Surgery 2030: evidence and solutions for achieving health, welfare, and economic development. Lancet 2015;386:569–62425924834 10.1016/S 0140-6736(15)60160-X · doi ↗ · pubmed ↗
- 4Weiser TG, Makary MA, Haynes AB, Dziekan G, Berry WR, Gawande AA et al Standardised metrics for global surgical surveillance. Lancet 2009;374:1113–719782877 10.1016/S 0140-6736(09)61161-2 · doi ↗ · pubmed ↗
- 5Davies JI, Gelb AW, Gore-Booth J, Martin J, Mellin-Olsen J, Åkerman C et al Global surgery, obstetric, and anaesthesia indicator definitions and reporting: an Utstein consensus report. P Lo S Med 2021;18:e 100374934415914 10.1371/journal.pmed.1003749 PMC 8415575 · doi ↗ · pubmed ↗
- 6Raykar NP, Ng-Kamstra JS, Bickler S, Davies J, Greenberg SLM, Hagander L et al New global surgical and anaesthesia indicators in the World Development Indicators dataset. BMJ Glob Health 2017;2:e 00026510.1136/bmjgh-2016-000265 PMC 571795629225929 · doi ↗ · pubmed ↗
- 7Torres Perez-Iglesias C, Jensen K, Raguveer V, Hyman GY, Suzuki E, Meara JG et al Tracking progress: trends in surgical indicator reporting in the world development indicators. med Rxiv. 10.1101/2024.12.24.24316011, 29 December 2024, preprint: not peer reviewed · doi ↗
- 8World Bank Open Data. https://data.worldbank.org (accessed 2 June 2025)