Maternal Knowledge of Oral Health During Pregnancy and Early Childhood: A Systematic Review
Alicia Aznar-Marín, María Dolores Casaña-Ruiz, Alfredo Perales-Marín, Montserrat Catalá-Pizarro

TL;DR
This review finds that pregnant women lack sufficient knowledge about oral health during pregnancy and early childhood, highlighting the need for better education and professional support.
Contribution
The study systematically identifies gaps in maternal oral health knowledge and proposes integrated educational strategies for prenatal care.
Findings
Most pregnant women have insufficient knowledge about oral changes during pregnancy and their impact on gestation.
Misconceptions such as 'a tooth is lost with every pregnancy' and incorrect beliefs about dental treatment safety are common.
Many women are unaware of when to start infant oral hygiene or schedule a child's first dental visit.
Abstract
Pregnant women's knowledge about the changes that occur in the oral cavity during pregnancy, as well as their impact on the course of pregnancy, is insufficient. Likewise, there is limited awareness of early childhood caries and of preventive oral-health measures. The aim of this study is to assess the level of knowledge, attitudes, and practices related to oral health among pregnant women, and to identify the main knowledge gaps concerning their own oral health and that of their future children. Scopus, Web of Science, Embase, and PubMed electronic databases were searched. Observational and cross-sectional studies published in different languages were included. Studies assessing adult pregnant women's knowledge, attitudes, and practices regarding their own oral health and that of their children were selected. Studies were excluded if they were qualitative in nature or focused solely…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
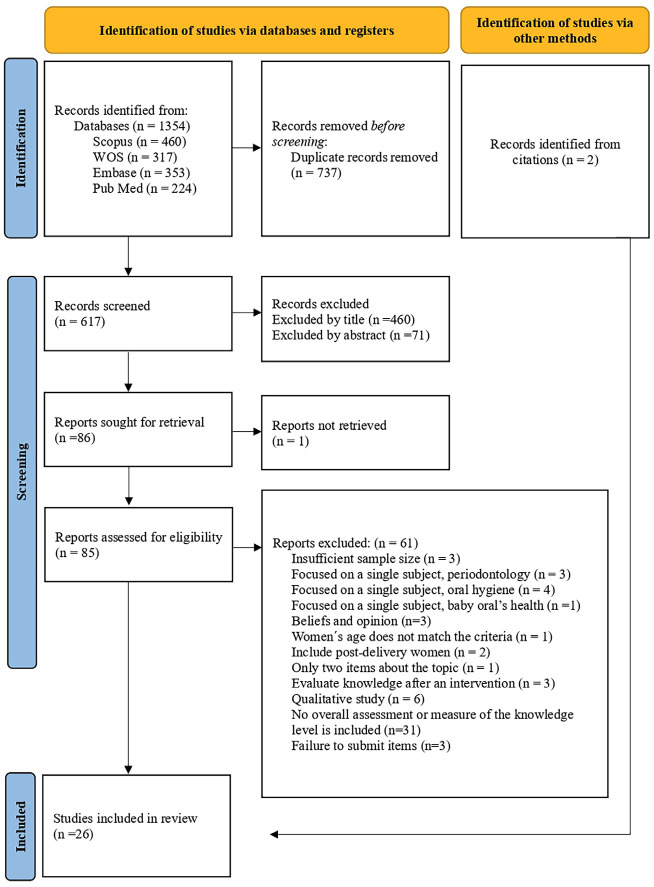 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsOral microbiology and periodontitis research · Dental Health and Care Utilization · HIV/AIDS oral health manifestations
Introduction
Pregnancy, defined as the period of fetal gestation within the maternal uterus (1), involves a series of physiological and hormonal changes that significantly modify a woman's body, including the oral cavity. Understanding these transformations is essential for anticipating their impact on the mother-child dyad, identifying potential associated problems, and determining the most appropriate timing for their management. Maintaining good oral health before and during pregnancy helps protect women's general health and quality of life, while also reducing the transmission of pathogenic bacteria from mother to child (2). The American Academy of Pediatric Dentistry (AAPD) acknowledges that perinatal and early childhood oral health constitutes the foundation upon which preventive education and dental care should be built, with the aim of increasing the likelihood that children grow up free from preventable oral diseases. In this process, the family plays a crucial role as the primary learning environment where children acquire knowledge, attitudes, and habits related to oral health (3). Despite the relevance of oral health during pregnancy, many women do not seek dental care during this stage. Nevertheless, this period represents a critical window of opportunity to promote oral care habits in both expectant mothers and their infants. In some contexts, it may also be the only time when women can access dental services. Barriers to improving oral health and dental service utilisation among pregnant women and their children are multifactorial, involving both healthcare system-related factors and individual determinants (4). In recent years, the international community has increasingly recognized the role of prenatal care providers-such as family physicians, midwives, gynecologists, and obstetricians-in implementing preventive oral health strategies within their clinical practice, as reflected in clinical guidelines and practice protocols (5). This systematic review aims to assess pregnant women's oral health knowledge, identify key knowledge gaps, and examine variables associated with knowledge levels, based on the available scientific evidence.
Material and Methods
The present study was conducted following the guidelines of the PRISMA (Preferred Reporting Items for Systematic Reviews) 2020 statement (6). It was registered in PROSPERO under the following reference: [CRD42023406157]. 1. Study Question and Eligibility Criteria The PICO question was: "What is the level of knowledge about oral health during pregnancy among pregnant women?" Eligibility criteria were established according to the PICO model as follows: Population (P): Pregnant women. Intervention (I): No informational intervention. Comparison/Control (C): Not applicable. Outcome (O): Knowledge, attitudes, and practices. 2. Inclusion and Exclusion Criteria Cross-sectional observational studies published in English, French, Italian, or Spanish that assessed baseline knowledge, attitudes, and oral health practices during pregnancy among adult pregnant women were included. Qualitative studies or those focused exclusively on beliefs and opinions were excluded, as well as studies that included a limited number of knowledge-related questions (3 items) or samples of fewer than 50 participants, and those addressing unrelated topics or conducted after an informational intervention. Studies focused solely on children or on women who were not primiparous or not newly delivered were also excluded, as were studies that did not provide the questionnaire or the items used for the assessment in the publication, and those that, despite using a questionnaire, did not evaluate knowledge qualitatively. 3. Data Sources and Search Strategy In January 2023, an electronic search was conducted in the Scopus, Web of Science (WOS), Embase, and PubMed databases. The search terms used were: (mother OR wom OR mater*) AND (pregnan*) AND (knowledge OR awareness) AND ("oral health") *, combined using the Boolean operators "AND" and "OR", and applied to the title, abstract, and keyword fields. The selection of terms was based on previous studies in this field. In addition, after the selection of the articles, a manual review of the references of the included studies was carried out to identify any further relevant research. The search was last updated on 17 April 2025. The advanced search equations and the results obtained for the individual and combined fields are presented in Table 1.
- Study Screening and Selection Process After searching each database, the records were imported into the EndNote Reference Manager (version 21.2), and duplicates were removed. Subsequently, two independent reviewers (A-AM and A-PM) performed the initial screening of the titles and abstracts. When the abstract did not provide sufficient information to determine whether the study should be included or excluded, the full text was assessed. Discrepancies between reviewers (which accounted for approximately 10% of the studies during the screening phase) were resolved by consensus. When consensus could not be reached, a third reviewer (M-CP) was consulted. In the second phase, the full texts of the selected articles were evaluated to determine their final eligibility according to the established inclusion and exclusion criteria. 5. Data Extraction and Recorded Variables A table was prepared containing the variables to be recorded for each study. Two independent reviewers (A-AM and MD-CR) performed the data extraction in parallel. Any discrepancies were resolved by consensus or, if necessary, through consultation with a third reviewer (M-CP). The extracted data included Study characteristics: author, year of publication, country or study location. Sociodemographic characteristics: age, parity, education, employment status. Questionnaire characteristics: type (self-developed non-validated; validated/reliability-tested), structure (closed-ended multiple-choice; subscales for knowledge), and topics covered (oral hygiene during pregnancy, mother-to-child bacterial transmission, early childhood caries prevention, dental visits, nutrition, fluoride use). Knowledge outcomes: overall mean scores and specific domains (pregnancy-related oral changes/periodontal disease/adverse gestation effects, cariogenic bacteria transmission to newborns, infant oral hygiene timing/first dental visit, dental treatment safety during pregnancy, misconceptions e.g., "a tooth lost per pregnancy"). The results of this extraction are presented in Table 2.
- Quality Assessment To assess the methodological quality of the included studies, the Newcastle-Ottawa Quality Assessment Scale (NOS) (33) was used for longitudinal studies, and the modified Newcastle-Ottawa Scale (NOS) (34 , 35) was applied for cross-sectional studies. This tool is structured into three domains: selection (sample representativeness, non-response rate, and instrument validation), comparability, and outcomes (assessment and statistical analysis). For longitudinal studies, each domain can achieve a specific maximum score: 4 points for selection, 2 points for comparability, and 3 points for outcomes, with a maximum total score of 9 points per study. For cross-sectional studies, the maximum possible score for each domain is: 5 points for selection, 2 points for comparability, and 3 points for outcomes, resulting in a maximum total score of 10 points per study. The results of the assessment are presented in Table 3 and Table 4.
- Data Synthesis Due to heterogeneity in the questionnaires and scoring systems employed, a quantitative synthesis (meta-analysis) was not feasible; therefore, a narrative synthesis was undertaken. No statistical pooling was performed, and heterogeneity was not formally assessed (e.g., using the I² statistic). Given the narrative approach and the clinical and methodological heterogeneity of the included cross-sectional studies, no formal assessment of publication bias (e.g., funnel plots or Egger's test) or certainty of evidence (e.g., GRADE) was conducted.
Results
- Search Results and Study Selection A total of 1.354 studies were identified through the electronic databases: Scopus (n = 460), Web of Science (n = 317), Embase (n = 353), and PubMed (n = 224). After removing 737 duplicate records, 617 studies remained for evaluation. During the initial screening, 460 records were excluded after reading the titles and 71 after reviewing the abstracts, leaving 86 potentially eligible studies. One of these could not be retrieved in full text. A total of 85 articles were assessed in full, of which 61 were excluded for not meeting the inclusion criteria. This process resulted in the selection of 24 studies. Additionally, two studies were identified through reference list screening, yielding a final total of 26 studies included in the review. Figure 1 presents the PRISMA flow diagram, detailing the stages of identification, screening, selection, and inclusion of the studies.
Figure 1PRISMA flow diagram.
- Results of the Studies Given the substantial heterogeneity in study populations, questionnaire designs, scoring systems, and outcome definitions, the results are synthesized using a qualitative and descriptive narrative approach. No pooled estimates, summary measures, or graphical representations (e.g., forest plots) are presented, as quantitative comparison across studies was not feasible. 2.1. Variables related to oral health knowledge It should be noted that the classification of knowledge levels (e.g., low, moderate, high) was defined by the original authors of each study and was based on study-specific cut-off points. Given the differences in questionnaire length, scoring ranges, and validation status, these qualitative categories are not directly comparable across studies and should be interpreted within the context of each individual investigation. The included studies primarily assessed the level of maternal knowledge about oral health during pregnancy and/or early childhood. This variable was measured using structured questionnaires, most of which were self-developed and non-validated (n = 11) (7 - 12 , 19 , 21 - 23 , 28), although 15 studies (13 - 18 , 20 , 24 - 27 , 29 - 32) employed validated instruments or reported reliability analyses (e.g., Pearson correlation coefficient or prior pilot testing). Two studies did not report this information. Overall findings revealed wide variability in maternal knowledge levels, influenced by sociodemographic factors such as education, age, and previous maternal experience. Studies that used validated instruments and larger samples (15 , 17 , 29) demonstrated greater methodological rigor and higher mean scores, suggesting a trend toward improved knowledge in settings with active preventive programs. Sociodemographic variables. The most frequently described variables were as follows: Maternal age ranged between 26 and 32 years on average, with minimum values of 24 years (19 , 24 , 30) and maximums of 35 years (15 , 29). Educational level was commonly categorized as primary, secondary, technical/university, or postgraduate, with most studies reporting a positive association between higher education and better oral health knowledge. Parity was classified as nulliparous, primiparous, or multiparous, with multiparous women predominating in most samples, representing between 40% and 76% of participants (11 , 17 , 18 , 21 , 23 , 26 , 29 , 32). Employment status (employed/unemployed) was reported in at least ten studies (11 , 14 , 15 , 21 - 23 , 25 , 27 , 29 , 32). Marital status, when provided, was categorized as "with partner" or "without partner," with over 80% of women reporting a stable partnership (9 , 10 , 13 , 32). Finally, ethnic or cultural background was reported mainly in multicentre studies or in countries with highly diverse populations (7 - 9 , 11 , 13 , 15 , 21 , 22 , 24 , 27 - 29 , 32). Variables related to oral health knowledge. In studies that specified the scoring system, knowledge scores ranged between 0.13 and 8.39 out of a maximum of 12 points, or between 40% and 82.8% correct responses, depending on the format and scoring criteria used in each questionnaire. The questionnaires covered topics such as oral hygiene during pregnancy, mother-to-child bacterial transmission, prevention of early childhood caries, dental visits, nutrition, and fluoride use. In most studies, approximately two-thirds, knowledge levels were rated as low or moderate, whereas only a few investigations conducted in Saudi Arabia (18 , 22), Malaysia (29), Poland (17), and Italy (15) reported high levels of adequate knowledge, exceeding 70% correct responses. Type and structure of questionnaires. The number of items varied between 14 (30) y 42 (27), with a predominance of closed-ended items with multiple-choice responses. Non-validated instruments were used mainly in studies conducted in Asia (10 , 12 , 14 , 16 - 18) and in America (9 , 11 , 28), whereas validated questionnaires originated from more recent European and Asian contexts such as Poland (17), Italy (15), Iran (31), and Malaysia (29). Some studies incorporated thematic subscales distinguishing maternal oral health knowledge from child oral health knowledge, as observed in the studies by Gavic et al. (20) and Hammad et al. (22). 3. Result of the Quality Analysis The results obtained were statistically analysed in all included studies. After applying the Newcastle-Ottawa Scales (NOS), the following findings were observed: Longitudinal studies. Two studies did not use randomized samples (16 , 24), and one did not provide evidence that the outcome or condition was absent in participants at baseline (16). Cross-sectional studies. The studies were classified as follows: 2 displayed very good quality (27 , 32); 4, good quality (7 , 13 , 17 , 18); 12, satisfactory quality (9 , 10 , 14 , 15 , 19 , 20 , 22 , 25 , 26 , 29 - 31); and 5, unsatisfactory quality (11 , 12 , 21 , 23 , 28) . Most of the included studies had limitations in the areas of 'non-respondents', 'comparability' and 'validated measurement tools'. A lack of information regarding response rates and the characteristics of non-respondents implies a risk of selection bias, as it prevents an adequate assessment of whether the respondents were representative of the target population. Cross-sectional studies (n = 23) demonstrated weaknesses in this area; 11 of these studies used non-validated, self-developed questionnaires, which could introduce measurement error through ambiguous items and potentially lead to an underestimation of true knowledge deficits. The detailed results of this assessment are presented in Table 3 and Table 4.
Discussion
- Main findings The results of this review confirm the existence of a significant gap in pregnant women's knowledge, attitudes, and practices regarding oral health. The studies show clear associations between knowledge level and sociodemographic variables such as educational attainment (11 , 13 , 17 , 18 , 20 , 22 , 24 , 27 , 29 , 31), employment status (22 , 27 , 32), cultural background (13 , 27), and parity (9 , 11 , 27). In this regard, Barbieri et al. (11) found higher knowledge among multiparous women, whereas Llena et al. (27). observed the opposite, and Baker et al. (9) found no significant differences between groups. Hormonal changes during pregnancy, together with dietary modifications, are identified as factors that may exacerbate oral conditions and affect fetal health (36). However, the degree of awareness among pregnant women regarding this relationship varies. Gaffar et al. (18), Hans et al. (23), and George et al. (21) reported that fewer than 50% of women recognize the link between oral health and general or fetal well-being, whereas Chawla et al. (24) and Gaszyska et al. (19), found higher levels of awareness, likely due to differences in education, access to information, or methodological approaches. Most pregnant women are unaware of the association between periodontitis and gestational complications, such as preeclampsia, low birth weight, or preterm delivery, despite periodontitis affecting up to 40% of pregnant women (36 , 37). Ten of the included studies addressed this topic, and none reported more than 50% correct responses (7 , 10 , 14 , 15 , 20 - 23 , 27 , 28). This lack of awareness is consistent with uncertainty among healthcare professionals, including gynecologists and obstetricians, which Montoya et al. (38) attribute to the complexity and lack of consensus regarding the causal relationship between periodontal disease and adverse pregnancy outcomes. 2. Comparison with previous literature Regarding dental caries, the studies consistently indicate insufficient knowledge about its etiology and transmissible nature. Adeniyi et al. (8) and Barbieri et al. (11) found that many participants were unfamiliar with the causes of caries, whereas Gaffar et al. (18), Chawlowska et al. (25), and George et al. (21) observed that most women were unaware of the transmission of cariogenic bacteria from mother to child, such as Streptococcus mutans (3). This lack of knowledge may lead to negligent attitudes toward preventive care for both mother and child, compounded by the underestimation of the importance of the primary dentition (19 , 26) 3. Implications for clinical practice and public health Although international clinical guidelines highlight the need to integrate oral health education into prenatal care (39), the studies agree that pregnant women seldom seek dental advice or receive treatment during pregnancy. In the United States, only 44.7% attend dental visits (40), and in Australia the figure drops to 30% (21). Frequent barriers include the cost of visits (17 , 21 , 28 , 30), low perceived risk or importance (21 , 31), the belief that they already have good oral health (9 , 10 , 19 , 21), and fear regarding the supposed harmfulness of dental treatment during pregnancy (21 - 23 , 28 , 30 , 31). Persistent myths include the belief that "a tooth is lost with each pregnancy" (13), "the fetus extracts calcium from the mother's teeth" (16), for that "caries are inevitable during pregnancy" (14). With respect to hygiene habits, although toothbrushing is widely practiced, the use of dental floss (18 , 21 , 29 , 30), mouthrinses (21 , 29), and fluoride (17 , 27 , 29) remains limited. This gap between knowledge and practice underscores the need to strengthen health education, as maternal habits directly influence children's oral health. In line with WHO, ADA, and AAPD recommendations, establishing a "dental home" before the child's first year of life and initiating toothbrushing with fluoride toothpaste upon eruption of the first tooth are advised (4). However, pregnant women's knowledge of these recommendations varies widely: Barbieri et al. (11) and Hammad et al. (22) reported that more than 60% of women knew when to begin brushing, while Bhaskar et al. (12) and Cagetti et al. (15) found rates below 40%. Regarding fluoride, Llena et al. (27) reported that only 28% were aware of its preventive effect, and Lakshmi et al. (26) and Gaszyska et al. (19) found that over 80% lacked this knowledge. The timing of the first dental visit is another area of deficiency: in the studies by Chawlowska et al. (17), George et al. (21), Hammad et al. (22), and Llena et al. (27), fewer than 33% responded correctly. Finally, sources of information about oral health vary across contexts. Gaszyska et al. (19) identified physicians and dentists as the main references (58%), followed by magazines and media (57%) and the internet (30%). In contrast, Gaffar et al. (18) and Chawlowska et al. (17) found that information mainly came from the internet and family members, with limited involvement of healthcare professionals. This educational gap reflects missed opportunities in prenatal care, associated with lack of time, limited training, or uncertainty regarding responsibility among gynecologists and midwives (41 - 47). 4. Limitations of included studies Among the limitations of this review, language restrictions (English, French, Italian, Spanish) may have introduced geographical publication bias by favouring studies from countries with stronger English-language research infrastructure, potentially underrepresenting non-Western contexts that publish primarily in local languages (e.g., additional sub-Saharan African or South Asian studies in Portuguese, Arabic, or regional dialects). Exclusion of non-indexed sources and grey literature (theses, institutional reports, conference proceedings) risks missing unpublished or locally disseminated evidence from low-resource settings, where oral health knowledge gaps may be more pronounced due to limited research dissemination capacity. Moreover, estimating overall levels of knowledge, attitudes, or practices proved challenging due to population and sociocultural heterogeneity, as well as methodological variability among included studies. These factors may contribute to underrepresentation bias toward contexts with more established research ecosystems. Additionally, methodological weaknesses within individual studies may systematically bias reported knowledge levels. Eleven studies (42%) utilized non-validated, self-developed questionnaires (7 - 12 , 19 , 21 - 23 , 28), potentially introducing measurement error through ambiguous items that overestimate knowledge by failing to capture nuanced gaps. Convenience sampling generated selection bias toward more health-literate participants, artificially elevating scores compared to population-representative samples. Self-reported knowledge, universal across all studies, is susceptible to social desirability bias. These factors contribute to the observed heterogeneity in scores (40-82.8% correct). Higher-quality studies employing validated instruments consistently reported lower knowledge levels, suggesting that methodological weaknesses may underestimate true deficits. Despite these limitations, the convergent pattern of insufficient knowledge across quality strata and regions supports the robustness of the primary findings. Despite these limitations, the findings of this review show that most pregnant women have insufficient knowledge about oral health during pregnancy and early childhood. Myths such as "losing a tooth per pregnancy" or the belief that dental treatments are harmful during gestation persist, and fewer than half of pregnant women are aware of the association between periodontal disease and pregnancy complications. Likewise, knowledge of mother-to-child transmission of cariogenic bacteria and of the appropriate timing to initiate infant oral hygiene remains low. Information available to pregnant women often comes from non-professional sources, such as the internet or magazines, highlighting the need to strengthen health education during pregnancy and to integrate dentists into prenatal care programs, along with specific training of healthcare personnel in perinatal oral health. Although integration of oral health into prenatal care has been proposed, more specific interventions are warranted, such as educational programs led by midwives and gynecologists, targeted informational resources for pregnant women, structured dentist referral pathways, and community-based initiatives aimed at improving access oral health information and care during pregnancy. Additionally validated standardized questionnaires would enable periodic assessment of pregnant women's oral health knowledge, support systematic identification of knowledge gaps, inform the adaptation of preventive programs, and facilitate comparisons across settings and countries.
Conclusions
In conclusion, the available evidence indicates that pregnant women generally exhibit low to moderate levels of oral health knowledge. Most studies included in this systematic review report limited awareness of pregnancy-related oral changes, the association between periodontal disease and adverse pregnancy outcomes, and the prevention of early childhood caries. Although modest improvements are observed in contexts with active preventive programs or higher educational attainment, substantial knowledge gaps and persistent misconceptions remain, particularly regarding the safety of dental treatments during pregnancy and the initiation of oral care in infancy. These findings underscore the need to strengthen oral health education during pregnancy through greater involvement of healthcare professionals and the integration of dental care into maternal health programs.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Pregnancy. Eunice Kennedy Shriver National Institute of Child Health and Human Development.[Internet]2025 cited 2025 https://www.nichd.nih.gov/health/topics/pregnancy.
- 2Latin American Association of Pediatric Dentistry. Guidelines on oral health in pregnant women for the multidisciplinary team 2016 Latin American Association of Pediatric Dentistry
- 3American Academy of Pediatric Dentistry, Policy on early childhood caries (ECC): classifications, consequences and preventive strategies, in The Reference Manual of Pediatric Dentistry 2020 Chicago American Academy of Pediatric Dentistry 7981
- 4American College of Obstetricians and Gynecologists. Perinatal Oral Health Practice Guidelines: Evidence-Based Guidelines for Health Professionals During Pregnancy & Early Childhood California Dental Association Foundation[Internet]2010 cited 2010 https://www.cda.org/wp-content/uploads/2023/01/CA Perinatal Oral Health_guidelines_2010-02.pdf.20645626 · pubmed ↗
- 5Ending childhood dental caries: WHO implementation manual 2021 Geneva World Health Organization
- 6Page MJ Mc Kenzie JE Bossuyt PM Boutron I Hoffmann TC Mulrow CDPRISMA 2020 statement: an updated guideline for reporting systematic reviews Rev Esp Cardiol 20217497909.3444626110.1016/j.rec.2021.07.010 · doi ↗ · pubmed ↗
- 7Abiola A Olayinka A Mathilda B Ogunbiyi O Modupe S Olubunmi OA survey of the oral health knowledge and practices of pregnant women in a Nigerian teaching hospital African journal of reproductive health 20111541419.22571100 · pubmed ↗
- 8Adeniyi AA Oyapero A Ajieroh V Sofola O Asiyanbi O Effect of health education intervention conducted by Primary Health Care workers on oral health knowledge and practices of nursing mothers in Lagos State J Public Health Afr 201892833.3068747910.4081/jphia.2018.833PMC 6325422 · doi ↗ · pubmed ↗