Factors Associated with Hypercementosis: A Cone Beam Tomography Study of Local Dental Conditions
María Victoria Martiren, Jhoana Mercedes Llaguno-Rubio, Gustavo Adolf Fiori-Chincaro, Luis Ernesto Arriola-Guillén

TL;DR
This study used 3D imaging to find that missing opposing teeth is the main cause of hypercementosis, a condition where extra cementum builds up on tooth roots.
Contribution
The study identifies the absence of an antagonist tooth as the primary local factor for hypercementosis using CBCT in a Uruguayan population.
Findings
Hypercementosis was found in 19% of patients, mostly affecting upper and lower molars.
The absence of an antagonist tooth was the most common local factor (24.71%).
Male sex was a protective factor for fewer affected teeth, while age had no significant effect.
Abstract
To evaluate the morphological characteristics of hypercementosis and its association with local factors using cone beam computed tomography (CBCT) in a population from Uruguay. This observational, cross-sectional, retrospective study analyzed CBCT scans from 1,830 patients aged 25 and older. The study recorded the presence and type of hypercementosis (diffuse, focal, maggot-shaped), the types of teeth affected, and associated local factors, including the absence of an antagonist, dental impaction, occlusal trauma, periodontal disease, periapical processes, and endodontic or orthodontic treatments, among others. Statistical analysis included chi-square tests and multiple linear regression, with a significance level set at p < 0.05. Hypercementosis was observed in 19% of the patients, affecting 595 teeth, primarily upper molars (48.6%) and lower molars (23.6%). The diffuse type was…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
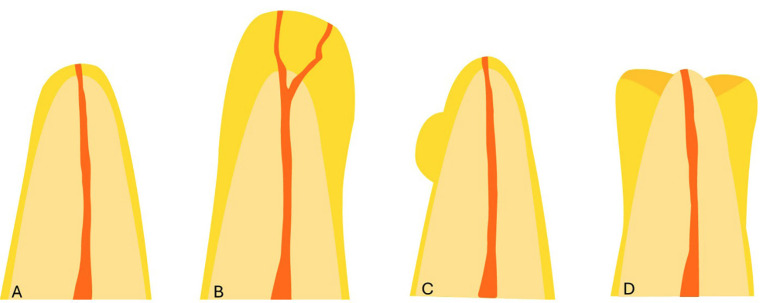 Figure 1
Figure 1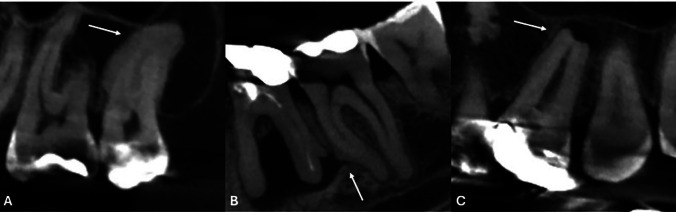 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsDental Radiography and Imaging · dental development and anomalies · Forensic Anthropology and Bioarchaeology Studies
Introduction
Hypercementosis is a non-neoplastic condition characterized by excessive deposition of root cement beyond normal levels (1). Macroscopic changes in the root of the tooth are evident (2 , 3). This condition is typically asymptomatic, and its diagnosis is based on radiographic findings (4). On radiographs, one may observe partial or total thickening of the root contour, while the lamina dura and periodontal ligament remain intact (5 , 6). Morphologically, hypercementosis can be diffused, focal, or sleeve-shaped, with the diffuse form being the most commonly observed (1 - 3 , 7). Its etiology is considered idiopathic and may be related to the patient's age (1 , 8); however, it is also associated with local factors such as the absence of an antagonist tooth, occlusal trauma, chronic periodontal inflammation, tooth impaction, and various systemic factors (3 , 6 , 8 - 10). Literature indicates that hypercementosis is a common condition, although it is rarely reported (1 , 2 , 7). Recent studies reveal prevalence rates of 16.3% in the Mexican population, 10.8% in the Turkish population, 9.8% in the Saudi Arabian population, 2.4% in southeastern Turkey, 1.3% in the German population, and 0.2% in the Iranian population (5 , 11 - 15). It is found to occur more frequently in mandibular molars and premolars (1 , 5 , 11 , 12 , 15). Hypercementosis usually does not require treatment; however, it is important to recognize this condition because it can lead to complications during endodontic (root canal) and orthodontic procedures, as well as during tooth extractions. Understanding hypercementosis is particularly crucial since the apical foramen can be in different positions (2). Additionally, there is a risk of partial ankylosis (the fusion of the tooth to the surrounding bone) associated with hypercementosis (8). Therefore, this study aims to evaluate the characteristics and types of hypercementosis in relation to local associated factors using cone-beam computed tomography (CBCT). This approach could improve the assessment and classification of the condition.
Material and Methods
- Study design This study obtained authorization and ethical approval from Centro Universitário do Norte de São Paulo (UNORTE), São Paulo, Brazil. We utilized a cross-sectional, observational, and retrospective design. The study group included 2107 CBCTs images. - Sample size calculation The sample size was calculated using a formula to estimate the proportion of patients with hypercementosis in the absence of an antagonist tooth, set at 25% based on data from a previous pilot study. A precision level of 3% indicated a minimum required sample size of 800 patients; however, the final study included 1830 patients. - Selection criteria We included CBCT scans from adult patients, aged 25 years and older, of both genders, who were treated at a private radiological imaging center in Montevideo, Uruguay, between 2018 and 2024. The scans could clearly show identifiable teeth with hypercementosis. We excluded any scans that did not meet quality standards, such as those affected by movement, noise, flashes, or artifacts. Additionally, scans with orthodontic or rehabilitation appliances, or those demonstrating pathologies or surgeries that could hinder accurate observation, were also excluded. - Image Acquisition All images were obtained using a Trophy brand CBCT device, model Trophypan Smart SC 3D, CS 8100, manufactured in Finland in 2017. The fields of view measured 5 cm x 5 cm, 5 cm x 8 cm, and 8 cm x 9 cm, with a voxel size resolution of 150 m. The device was set to a Kv of 60-90, an mA of 2-15, and an exposure time of 7-15 seconds. The patient's position was adjusted per the manufacturer's manual, ensuring the Frankfort plane was parallel to the floor and that the bite and positioning support points were correct. - Reading and Recording Images were evaluated in a controlled, semi-lit environment using a 32-inch Samsung M8 flat-screen monitor. Evaluations were conducted between 7:00 a.m. and 10:00 a.m. All data was recorded in an Excel database according to the specified criteria. - Training and Pilot Test Prior to conducting the study, the examiner underwent a training phase using a randomly selected set of CT scans, focusing on radiographic identification of hypercementosis and on standardizing the CBCT evaluation procedure, under the guidance of an oral and maxillofacial radiology specialist with more than 5 years of experience. An intra- and inter-observer agreement index (kappa coefficient) of 0.9 or higher was achieved. Subsequently, a pilot test involving 10% of the study sample was conducted, allowing for adjustments in the observation order and confirming the feasibility of the proposed methodology. Results from the pilot test were included in the final analysis. - Variables measurements Hypercementosis was evaluated based on three types: diffuse (characterized by a club-shaped root), focal or localized (appearing as an isolated root surface), or sleeve-shaped (where the apex is laterally surrounded but not compromised at its most apical part), as illustrated in Figure 1 and 2.
Figure 1. Morphological types of hypercementosis: A) Normal root; B) Diffuse hypercementosis; C) Focal or localized hypercementosis; D) Sleeve-shaped hypercementosis.
Figure 2. The arrows indicate: A) Diffuse hypercementosis in the buccal roots of an upper molar. B) Focal hypercementosis located in the middle third of the mesial root of a lower molar. C) Sleeve-like hypercementosis observed in the palatal root of an upper molar.
We considered the subjects' age (in years) and sex (female or male). Additionally, we evaluated local triggering factors, which included: Dental impaction (when teeth have not erupted due to insufficient space, malposition, or obstructive elements). Absence of an antagonist tooth (either partial or complete retention of the opposing tooth). Occlusal trauma (resulting in faceting of the tooth surface). Periodontal disease (characterized by loss of alveolar bone height and increased periodontal ligament space). Periapical inflammation (identified by osteolytic images associated with the root of the tooth). Increased surrounding bone density, indicating signs of a periapical lesion. Existence of endodontic or orthodontic treatment. - Statistical Analysis Statistical analyses were conducted using SPSS version 19 for Windows. We examined the association between the number of hypercementosis cases and various factors, including sex, age, and local dental conditions, utilizing the chi-squared (²) test. Additionally, we employed multiple linear regression to assess whether the incidence of hypercementosis was influenced by age and sex. All analyses were performed using a significance level of p < 0.05.
Results
A total of 1,830 patients were evaluated, with hypercementosis observed in 348 (19%) and affecting 595 teeth overall. Table 1 presents the number of teeth with hypercementosis by sex, with a p-value of 0.156, indicating no statistically significant association.
Most patients had hypercementosis in a single tooth, accounting for 57.2% of the total (199 patients). Within this group, females predominated with 138 patients (62.7%), while males accounted for 61 patients (47.7%). Additionally, 27.3% of patients had two affected teeth (24.5% in females and 32% in males), while up to 7 teeth with hypercementosis were found in a single patient (0.3%). Regarding the types of teeth affected by hypercementosis, the most commonly affected were the upper molars (169 teeth, 48.6%), followed by lower molars (82 teeth, 23.6%) and upper premolars (57 teeth, 16.4%). Upper canines were more affected than lower premolars (27 teeth, 7.8%, compared to 11 teeth, 3.2%). No significant association was found between sex and the type of tooth affected (p=0.272) (Table 2).
Concerning the morphological patterns of hypercementosis, the diffuse form was the most prevalent, accounting for 91.7% (319 teeth), followed by focal hypercementosis at 6% (21 teeth) and the sleeve form at 2.3% (8 teeth). There was no significant association between sex and the type of hypercementosis (p=0.991) (Table 3).
As shown in Table 4, there was a significant association between the type of hypercementosis, and the teeth evaluated (p < 0.001). The diffuse form predominated across all tooth types, except the lower incisors, where focal hypercementosis was more common (66.7%).
The highest number of focal cases was found in upper and lower molars (8 teeth in each group) and upper canines (4 teeth). Sleeve-shaped hypercementosis was more common in lower molars (6 teeth, 4.4%), followed by upper molars (2 teeth). When examining the association between hypercementosis type and contributing factors, the most frequently observed factors were: first, the absence of an antagonist (147 affected teeth); second, tooth impaction (125 teeth); and third, idiopathic cases (79 teeth). The type of hypercementosis was mainly diffuse, with 99.3%, 98.4%, and 97.5% prevalence for these factors, respectively. Other factors had less influence. The significance testing showed that combinations of specific factors-such as apical lesions, endodontic treatment, and increased bone density-can lead to focal or sleeve-type hypercementosis (Table 5).
In exploring the relationship between the type of tooth with hypercementosis and related local factors, significant results were observed (p<0.001). The most affected teeth in the absence of antagonist were primarily upper molars (81%). In cases of impaction, the upper molars were affected in 47.2% and the lower molars in 44.8%. For cases without local factors (idiopathic), the distribution among dental groups showed that upper premolars were most affected (34.2%), followed by lower molars (21.5%), upper canines (16.5%), upper molars (15.2%), and lower premolars (8.9%) (Table 6).
Table 7 presents a multiple linear regression analysis evaluating the influence of sex and age on the number of teeth with hypercementosis. The analysis indicated that sex significantly influences this occurrence (p=0.010), demonstrating that being male is a protective factor against increased number of teeth with hypercementosis in 69.5% of cases.
Discussion
There is limited research examining the relationship between different types of hypercementosis and the local factors that contribute to them. Most studies are based on small retrospective studies of X-rays or on individual case reports. Recognizing the prevalence and associated factors of this condition is crucial because it can lead to complications during endodontic (root canal) treatments, orthodontic procedures, and tooth extractions. Understanding hypercementosis is essential, as the position of the apical foramen may vary, which can impact the treatment of affected teeth (16 - 20). Furthermore, there is a risk of partial ankylosis, the fusion of the tooth to the surrounding bone, associated with hypercementosis. In our study, the idiopathic factor was the third most prevalent (present in 13.3% of cases), unlike in Mexican (5) and Turkish (12) populations, where it was the most prevalent. The most frequent factor in our evaluation was the absence of an antagonist tooth (24.71%), in which occlusal forces are almost nil, and cement overproduction can be explained, according to Consolaro et al. (20), as an adaptive response to increase tooth-bone fixation. In this regard, a study conducted in Tokyo observed that functional teeth have a lower frequency of hypercementosis, suggesting that continuous occlusal forces prevent cement formation, thereby favoring the absorption of masticatory forces. The second factor evaluated in our study was tooth impaction (21,01%). As in the study conducted in the Mexican population, impaction ranked second in prevalence (23.3%). Unlike the findings of Defne et al. (12) in the Turkish population, tooth impaction was only observed in 1.25% of cases, making it the second least frequent factor. According to the literature, these cases of hypercementosis can be explained as a response to continuous tooth eruption (17 , 21). In our study, we also evaluated various local factors to a lesser extent. These factors included periodontal disease (4,03%), orthodontic treatment (3.87%), periapical infections (3,03%), faceting (2.52%), and endodontic issues (2.18%). Additionally, we noted the presence of other factors, such as deep caries, extensive restorations, dental malpositions, and maxillary lesions, which, combined, accounted for a total incidence of 8.4%. Regarding hypercementosis type, we observed that the diffuse form was the most frequent and the sleeve-shaped form was the least frequent, in agreement with other studies (5 , 12 , 20 , 22). The most affected teeth were the upper and lower molars, with a higher incidence in the maxilla (72%) than in the mandible (5 , 11 , 12 , 14 , 15), contrary to what is observed in the literature. Although the prevalence of hypercementosis in the lower incisors was low, two of the three cases were focal. Nevertheless, given the small sample size, we cannot conclude that lower incisors with hypoplastic enamel will always exhibit the focal type; this may be specific to the sample studied. However, this research did reveal a significant difference. In our research, although we can see significance between the association of local factors and the type of hypercementosis, with a higher incidence of focal or sleeve-shaped hypercementosis observed in cases where some factors coexist (endodontics, periapical lesion, increased bone density), there are few cases evaluated, so this association should be taken with caution. While our study found no significant association between the teeth affected by hypercementosis and sex, we observed that a higher proportion of the number of teeth with this condition occurred in women than in men. This observation was supported by multiple linear regression analysis, which suggested that being male might serve as a protective factor. We chose to use linear regression analysis to evaluate the number of teeth impacted by hypercementosis. In contrast, other studies often compare groups with and without hypercementosis, whereas our study included only cases that presented hypercementosis. Additionally, in most of the studies reviewed, sex was not a significant factor, except for one study conducted in a German population, which reported that females were 10 times more affected than males (14). As observed by Bernal Ruíz et al. (5) in the Mexican population and by Eren et al. (15) in the Turkish population, the majority of patients had only one tooth with hypercementosis (57.2%). Hypercementosis is a condition linked to a patient's age; however, in our study, age did not show a significant association (p=0.273). This finding aligns with the research conducted by Elsayed et al. (11) in Saudi Arabia, where age also had a non-significant correlation (p=0.633). Besides, our study found that the absence of an antagonist tooth was the local factor most commonly associated with hypercementosis. Interestingly, males demonstrated a lower incidence of hypercementosis, suggesting a possible protective effect regarding the number of affected teeth. Overall, age did not appear to be a significant factor, and diffuse hypercementosis was identified as the most prevalent type. One limitation of our study was the small sample size; we could have benefited from comparing it with a control group and from exploring additional interesting variables. While the results of this study cannot be generalized, the substantial sample size and methodology offer a solid foundation for formulating hypotheses for future research using different methodological approaches.
Conclusions
The local factor most frequently associated with hypercementosis was the absence of an antagonist tooth. Males had a lower incidence of hypercementosis, which could be considered a protective factor for the number of teeth with this condition. Age was not a determining factor, and diffuse hypercementosis was the most prevalent type.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Warrier SA Vinayachandran D Irregular periapical radiopacity in mandibular premolars and molars Case Rep Dent 20142014910843.2471600310.1155/2014/910843 PMC 3970047 · doi ↗ · pubmed ↗
- 2Pinheiro BC Pinheiro TN Capelozza AL Consolaro AA scanning electron microscopic study of hypercementosis J Appl Oral Sci 20081663804.1908239510.1590/S 1678-77572008000600005 PMC 4327707 · doi ↗ · pubmed ↗
- 3Consolaro A Cementum, apical morphology and hypercementosis: A probable adaptive response of the periodontal support tissues and potential orthodontic implications J Orthod 20121712130.
- 4Stavrou E Tosios KI Stavrou IE Globular radiopacity around the apex of an impacted maxillary third molar Oral Surg Oral Med Oral Pathol Oral Radiol Endod 200710355948.1733175710.1016/j.tripleo.2006.11.050 · doi ↗ · pubmed ↗
- 5Bernal Ruiz MA Fiori Chíncaro GA Patterns of hypercementosis and their relationship with possible local etiological factors in radiographs of individuals from a mexican population Rev Cient Odontol (Lima)2023113 e 163.3828799610.21142/2523-2754-1103-2023-163PMC 10810069 · doi ↗ · pubmed ↗
- 6Basdra EK Stellzig A Komposch G Generalized hypercementosis in a young female patient Oral Surg Oral Med Oral Pathol Oral Radiol Endod 19978344189.10.1016/s 1079-2104(97)90137-29127369 · doi ↗ · pubmed ↗
- 7MasséL Garot E Maureille B Le Cabec A Insights into the aetiologies of hypercementosis: A systematic review and a scoring system Arch Oral Biol 2023146105599.3649581210.1016/j.archoralbio.2022.105599 · doi ↗ · pubmed ↗
- 8Humerfelt A Reitan K Effects of hypercementosis on the movability of teeth during orthodontic treatment Angle Orthod 196636317989.522125010.1043/0003-3219(1966)036<0179:EOHOTM>2.0.CO;2 · doi ↗ · pubmed ↗