Unfavorable fractures during Sagittal Split Osteotomy. What are the Risk Factors? A Retrospective Tomographic Study
Thalles Moreira Suassuna, Elenisa Glaucia Ferreira dos Santos, Sérgio Murilo Cordeiro de Melo Filho, Maria Taywri Almeida Costa, Fábio Andrey da Costa Araújo, José Rodrigues Laureano Filho

TL;DR
This study identifies risk factors for unfavorable fractures during jaw surgery, finding that surgical technique is more important than anatomy.
Contribution
The study provides new insights into the technical and anatomical risk factors for 'Bad Split' fractures during mandibular osteotomy.
Findings
The incidence of 'Bad Split' fractures was 3.2% with a left-side predominance.
Technical factors like incomplete osteotomy execution were more significant than anatomical variables in causing fractures.
Class A fractures were most common and associated with anterior lingula position and lower alveolar crest.
Abstract
This study aims to analyze the epidemiology of "Bad Split" (BS) during Sagittal Osteotomy of the Mandible, identifying anatomical and technical risk factors associated with its occurrence. A retrospective analysis was conducted on 157 patients (314 osteotomies) over five years. Multi-slice helical CT scans, both pre- and post-operative, were examined to classify BS and identify potential risk factors. Anatomical variables included the presence of third molars, edentulism, prior fixation systems, mandibular ramus dimensions, lingula position, and alveolar crest height. Technical aspects of osteotomy execution were also assessed. Measurements were performed using Dolphin Imaging Software 11.95 after orienting the skull in the Natural Head Position. The incidence of BS was 3.2% (10 patients), with a slight left-side predominance (60%). Class A BS (distal fracture of the proximal segment)…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
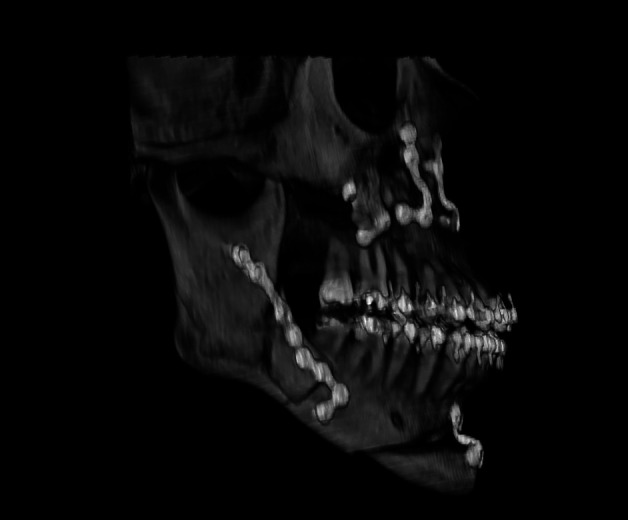 Figure 1
Figure 1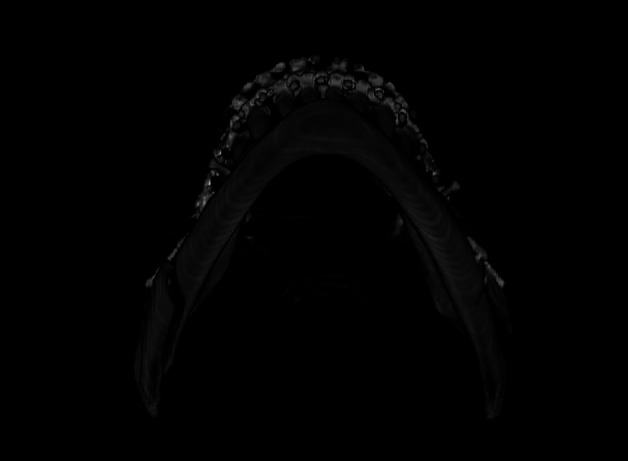 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsOrthodontics and Dentofacial Orthopedics · Spinal Fractures and Fixation Techniques · Facial Trauma and Fracture Management
Introduction
Unfavorable fracture, or "Bad Split" (BS), during Sagittal Osteotomy of the Mandible remains one of the primary complications associated with this technique, from its initial description and the present day (1 - 3).The incidence can reach up to 15%.The occurrence of this complication can make the procedure significantly more challenging, time-consuming, and morbid for the patient, leading to instability, infection, and malunion. Several factors have been identified that may increase the risk of BS. These factors can relate to the patient, such as age, anatomy, and the presence of teeth in the region, or to the execution of the procedure itself. However, the literature is not yet conclusive about which factors are most determining and lacks tomographic studies that evaluate anatomical parameters and the execution of the osteotomy. To epidemiologically study the patterns of Bad Split and identify risk factors that may contribute to its occurrence (4 - 6).
Material and Methods
This was a retrospective study involving 157 patients (314 osteotomies) operated on over five years by a hospital's surgical team, using the classic Sagittal Osteotomy popularized by Traunner and Obwegeser, later modified by Dal Pont and revised by Epker. The sample comprised patients diagnosed with intraoperative unfavorable fractures, necessitating additional osteotomies for appropriate separation between the proximal and distal segments. Multi-slice helical CT scans, both pre- and post-operatively, were studied to classify BS and identify possible risk factors. The analyzed criteria included: presence of third molars; edentulism; presence of prior fixation systems; thickness, height, and length of the ramus; anteroposterior location of the lingula; and height of the alveolar crest. Comparisons were always made with the contralateral side of the same patient. The executed osteotomies were also analyzed to assess whether there were differences compared to the opposite side, deviation, or incomplete cuts. The examinations were analyzed using Dolphin Imaging Software 11.95, where, after orienting the skull in the Natural Head Position, measurements were performed using the "Digitize-Measure - 2D line" tool. The research was conducted in accordance with the Code of Ethics of the World Medical Association (Declaration of Helsinki) and was approved by the Ethics Committee, under the umbrella project CAAE 74613823.2.0000.5207. It posed no risk to participants, as the intervention had already been performed and no additional examinations beyond routine were required.
Results
Ultimately, 10 patients (6.4%) with intraoperative diagnosis of unilateral BS were included, representing 3.2% of the total osteotomies. BS occurred in 40% on the right side and 60% on the left. The mean age of patients was 30 years, with only one patient over 40 years. The male-to-female ratio was 1:1. The most affected deformity was Facial Pattern III, accounting for 60% of cases. The presence of a third molar was found in two cases. In two patients, there was an absence of at least one molar on the osteotomy side, and one BS case showed the presence of bicortical plates and screws from prior trauma surgery. Class A BS (fracture of the distal part of the proximal segment) was the most common, occurring in 60% of cases, followed by Class B (fracture of the distal part with involvement of the coronoid) in 30% of cases (Table 1, Fig. 1).
Figure 1. Type A of badsplit. The most common type found in our study, accounting for 60% of cases.
Regarding the anatomical study of the affected side compared to the unaffected side, it was observed that in 40% of patients, the affected mandibular ramus was slightly thicker, 40% were similar, and 20% were narrower. In 50% of patients, the ramus presented decreased height compared to the other side, while 30% had similar height and 20% had greater height. Concerning the positioning of the lingula, 50% of the affected sides had the lingula in a more anterior position, 30% in a similar position, and 20% more posterior with the differences not being statistically significant. The measurements of anteroposterior length of the mandibular ramus and height of the crest showed balance between the sides (Table 2).
The technical evaluation of the osteotomy lines found that in 8 individuals (80%), there was a deviation from the opposite side or from what would be the recommended technique, with incomplete osteotomy at the basal level being the most identified alteration (60%) (Table 3, Fig. 2).
Figure 2. Example of technical deviation on the left side of the mandible, where the badsplit occurred. Note that the basilar osteotomy did not extend to the lingual side.
Discussion
Among the existing classifications of Bad Split (BS) (7), we utilized the Beukes et al. (2013) classification due to its practicality and representation of the patterns observed in our study. We found that 90% of BS cases affected the oral region of the proximal segment (Type A or B), with one-third involving the coronoid process (Type B), indicating that the oblique line region is the most susceptible to fractures. We recorded a total incidence of 3.2% for unfavorable fractures, with an equal distribution between genders. There was no significant influence from the type of occlusion or age, which ranged from 18 to 43 years (mean age 30.1). These findings are consistent with other studies on the subject (8 - 12), suggesting that age, gender, and type of deformity are not risk factors. The possibility of a third molar contributing to the occurrence of BS is often raised. Several studies (13 , 8 , 14 , 15) have indicated an increased intraoperative difficulty and a risk escalation of up to 9 times in the presence of these elements (15). However, systematic reviews on this topic (4 , 16) concluded that the scientific evidence is not robust enough to indicate a positive correlation. In our study, we found that 20% presented with a third molar, 20% had edentulism, and 10% had previous osteosynthesis. This suggests that these factors may contribute to an increased risk of BS, as patients with these conditions are exceptions in our sample. Additionally, numerous studies have analyzed mandibular anatomy through measurements to identify more susceptible patterns. It has been found that mandibles with less cancellous bone, where the distance from the canal to the cortex was shorter, were more prone to BS (5 , 12 , 17 - 19). It was also identified that, besides thickness, decreased height may increase the risk of BS (8 , 11). Fujii et al. (22) further found that a high difference in thickness before and after entering the canal may favor BS. In contrast to previous studies, we did not find a difference in ramus thickness, but rather similar measurements between the sides when all BS cases were grouped together (Table 2). However, when isolating only Class A fractures, the most prevalent at 60%, we found that 83.3% of cases had the lingula closer to the anterior edge than the control side, and 66% had a lower height of the bony crest. This suggests that anatomy may influence the type of BS when it occurs (Table 4).
This data indicates that future research should separate anatomical analyses by BS pattern rather than grouping them together. The objective of the evaluation method (split mouth) was to investigate the reason for BS occurring on one side and not the other, observing the differences between them. Thus, technically assessing the executed osteotomy would also be crucial for this study. In this evaluation, it was found that in 80% of BS cases, there was a "deviation" in the execution of the osteotomy, with incomplete osteotomy at the basal level being the most common deviation (60%) (Table 4). Several authors have highlighted the importance of the surgeon as a crucial factor. Studies involving a single surgeon have reported lower incidence rates (7 , 9 , 15) compared to studies from teaching hospitals (20 , 19). Thisunderscores the importance of the surgeon's experience in reducing the number of cases, even in "prone" mandibles. Efforts should always be made to avoid complications, and precautions with the osteotomy should include positioning the lingual cut just above the lingula, extending to the end of this structure; performing an oblique and vertical cut throughout its length down to the medullary area; and progressing the vertical cut at the base to the lingual (20 , 4 , 19 , 15 , 12).Furthermore, the cleavage should be approached very cautiously, starting from the basal and anterior regions before progressing posteriorly, always using fine chisels and applying light force. In case of resistance, the osteotomies and angles should be reassessed (20 , 4 , 19 , 15). In cases of BS, one should aim to complete the separation of the segments as atraumatically as possible, typically through osteotomy in the proximal region of the distal segment. Intermediate segments should be kept adhered to the soft tissues and fixed to the main segments as much as possible (20 , 4 , 19 , 15).
Conclusions
Factors such as the presence of third molars, edentulism, and fixation plates in the region appear to have a minor influence on the occurrence of Bad Splits. Mandibles with more anterior lingulae and lower heights of the alveolar crest are more susceptible to the occurrence of Class A Bad Split. Technical factors can strongly influence the occurrence of Bad Split, potentially being more determining than anatomical factors, placing the onus on the surgeon to execute the entire procedure as carefully as possible.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Bockmann R Meyns J Dik E Kessler P The modifications of the sagittal ramus split osteotomy: a literature review Plast Reconstr Surg Glob Open 20142 e 271.2558750510.1097/GOX.0000000000000127 PMC 4292253 · doi ↗ · pubmed ↗
- 2Mac Intosh RB Experience with the Sagittal Osteotomy of the Mandibular Ramus: A 13-Year Review J Maxillofac Surg 19818151165.10.1016/s 0301-0503(81)80036-76974211 · doi ↗ · pubmed ↗
- 3Peleg O Mahmoud R Shuster A Arbel S Manor Y Ianculovici C Orthognathic surgery complications: The 10-year experience of a single center J Cranio-Maxillofac Surg 20214910891897.10.1016/j.jcms.2021.04.00633994296 · doi ↗ · pubmed ↗
- 4Steenen S Avan Wijk AJ Becking AG Bad splits in bilateral sagittal split osteotomy: systematic review and meta-analysis of reported risk factors Int J Oral Maxillofac Surg 20164589719.2698013610.1016/j.ijom.2016.02.011 · doi ↗ · pubmed ↗
- 5Fujii Y Hatori A Horiuchi M Sugiyama-Tamura T Hamada H Sugisaki R Computed tomography evaluation of risk factors for an undesirable buccal split during sagittal split ramus osteotomy P Lo S One 2023183 e 0279850.3686269210.1371/journal.pone.0279850 PMC 9980734 · doi ↗ · pubmed ↗
- 6Steenen SA Becking AG Bad splits in bilateral sagittal split osteotomy: systematic review of fracture patterns Int J Oral Maxillofac Surg 201645788797.2693637710.1016/j.ijom.2016.02.001 · doi ↗ · pubmed ↗
- 7Beukes J Reyneke JP Becker PJ Variations in the anatomical dimensions of the mandibular ramus and the presence of third molars: its effect on the sagittal split ramus osteotomy Int J Oral Maxillofac Surg 20134233037.2310302510.1016/j.ijom.2012.09.020 · doi ↗ · pubmed ↗
- 8Wang T Han JJ Oh HK Park HJ Jung S Park YJ Evaluation of Mandibular Anatomy Associated With Bad Splits in Sagittal Split Ramus Osteotomy of Mandible J Craniofac Surg 2016275 e 5004.2739152210.1097/SCS.0000000000002798 · doi ↗ · pubmed ↗