Periodontitis, colorectal cancer and associated factors: A cross-sectional study
Rosita Elena Espejo-Carrera, María Elizabeth Mendoza-Rubio, Carlos Alberto Minchón-Medina, César Abraham Vásquez-Plasencia, José Antonio Caballero-Alvarado, César León-Vega, Oscar Martín Del Castillo-Huertas, Angel Steven Asmat-Abanto

TL;DR
This study investigated if periodontitis severity is linked to colorectal cancer but found no significant association in a Peruvian patient population.
Contribution
The study provides new evidence from a Peruvian cohort on the lack of association between periodontitis severity and colorectal cancer diagnosis.
Findings
No association was found between periodontitis severity and colorectal cancer diagnosis (p=0.068).
Stage IV and III were the most common CRC stages, with rectum and sigmoid colon as primary tumor locations.
Abstract
Periodontitis can cause systemic alterations associated with various oncological diseases, including colorectal cancer (CRC), with little information on this possible association and its related factors. Objectives: To determine the association between periodontitis severity, CRC, and related factors in adult patients. This cross-sectional study was conducted between January and March 2025 at the Trujillo Regional Teaching Hospital and the "Dr. Luis Pinillos Ganoza" Regional Institute of Neoplastic Diseases - North IREN, Trujillo, Peru. A total of 320 adult patients were evaluated: 160 without colorectal cancer (non-CRC) and 160 with colorectal cancer (CRC). Inter- and intra-rater reliability was determined for the diagnosis of periodontitis, bleeding on probing (BOP), and dental plaque control (DPC). The corresponding specialist physician performed the diagnosis of colorectal cancer…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
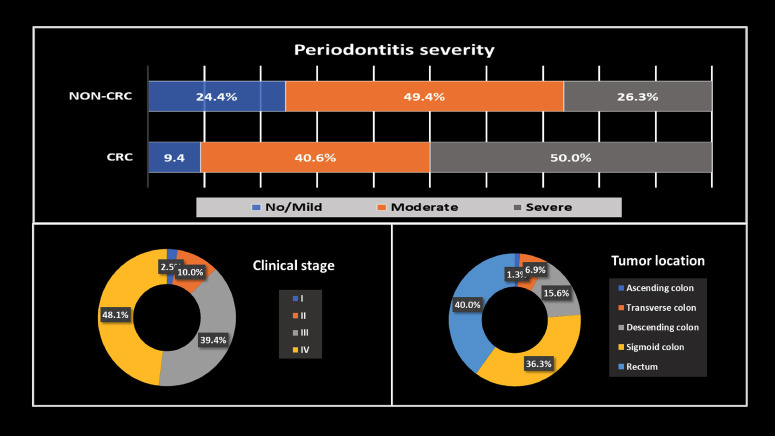 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsOral microbiology and periodontitis research · HIV/AIDS oral health manifestations · Dental Radiography and Imaging
Introduction
Periodontitis is a chronic inflammatory condition associated with an imbalance in the oral microbiome. This condition causes gradual, permanent deterioration of the tissues that support the teeth, potentially leading to tooth mobility and tooth loss (1). Worldwide, it is estimated that 45%-90% of individuals have some degree of periodontitis, with its severe form affecting 11.2%-20% of the population (2). Nearly one-third of recent studies on periodontitis have focused on exploring its link to various systemic diseases, including diabetes mellitus, cardiovascular and respiratory diseases, Alzheimer's disease, and some types of cancer (3 , 4). Cancer is a disease characterized by the unregulated growth of abnormal cells, which evolve through natural selection via genetic and epigenetic alterations, developing a potentially lethal phenotype (3). Colorectal cancer (CRC) represents one of the leading causes of disease and death worldwide. Globally, it is the second most common malignant neoplasm with the highest number of deaths in both sexes (1), with a strong association with age, being more common in people over 80 years of age, with a less favorable prognosis (5). Several factors have been linked to the development of CRC, such as male gender, low socioeconomic status, presence of diabetes mellitus, excess body fat, family history of CRC in first-degree relatives, smoking habits, high intake of red and processed meats, and excessive alcohol consumption, among others (4). Specifically, two periodontopathogenic bacteria have been identified in CRC: Fusobacterium nucleatum (F. nucleatum) and Porphyromonas gingivalis (P. gingivalis). F. nucleatum adheres to tumor cells and fibroblasts via its surface proteins FadA, Fap2, and RadD, and induces the production of inflammatory factors, suppressing the immune cellular function of macrophages and T and NK lymphocytes, contributing to the development of CRC (4 , 6). In addition, it has been associated with regional lymph node metastasis (1). P. gingivalis can alter the balance of the intestinal microbiota, elevating blood endotoxin concentrations, inducing a systemic inflammatory response, modifying host metabolism, and facilitating evasion of the immune system, thus generating favorable pathophysiological conditions for colorectal carcinogenesis (7). Based on the above, this study aimed to determine the association between periodontitis and CRC in adult patients, while accounting for potentially confounding factors, including sociodemographic characteristics, diverticulosis, type 2 diabetes mellitus (T2DM), cigarette and alcohol consumption, dental plaque control (DPC), and bleeding on probing (BOP). The findings of this research aim to provide relevant information to understand better periodontal medicine and health in relation to oncological diseases. It also motivates future researchers to explore potential clinical links that may promote periodontal health and develop interventions that improve the prognosis and quality of life of cancer patients.
Material and Methods
This cross-sectional study was conducted at the Department of Surgery of the Trujillo Regional Teaching Hospital (TRTH) and the Department of Abdominal Surgery of the "Dr. Luis Pinillos Ganoza" North Regional Institute of Neoplastic Diseases (North IREN), Trujillo, Peru, between January and March 2025. The sample consisted of 320 patients: 160 with CRC and 160 without CRC (non-CRC). The sample size was calculated using the formula for comparing patients with CRC and non-CRC using data generated through a pilot study conducted with 30 patients per group and with the following parameters: n (Sample size for each group), Z/2=1.96 (Normal value with type I error of =5%), Z=1.645 (Normal value with test power of 1-=95%), p1=0.830 (Prevalence of moderate or severe periodontitis in CRC patients, estimated based on the pilot sample), p1=0.655 (Prevalence of moderate or severe periodontitis in non-CRC patients, estimated based on the pilot sample), p = 0.743 (Prevalence of moderate or severe periodontitis in CRC and non-CRC patients). The selection method was non-probabilistic and accidental. The study included adult patients aged 40 - 79 years with a histological diagnosis of CRC who attended the North IREN, as well as non-CRC patients from the TRTH surgical outpatient clinic. North IREN is the referral center for cancer patients at hospitals in Northern Peru, including TRTH. Patients with fewer than six teeth, underlying immunosuppression, hereditary CRC (including Lynch syndrome), or those who refused to participate were excluded from the study. Approval from the Faculty of Human Medicine (RESOLUTION No. 4567-2024-FMEHU-UPAO) and the Bioethics Committee of the "Antenor Orrego" Private University (Bioethics Committee Resolution No. 000396-2025-UPAO), the Board of Directors of the Research Ethics Committee of the TRTH (No. 001-2025), and the North IREN Institutional Research Ethics Committee (No. 000225-2025-GRLL-GGR-GRS-IREN) was obtained for this study. These units strictly comply with the principles established in the Declaration of Helsinki, adopted by the 75th General Assembly of the World Medical Association, and the General Health Law of Peru No. 26842. Before requesting their participation, all patients received information about the research purposes. Upon acceptance, they were given the informed consent form to read and sign. The diagnosis of CRC was established or ruled out by specialist physicians from the respective departments through biopsy and appropriate complementary tests. The presence of periodontitis was subsequently evaluated according to the CDC/AAP classification, validated and agreed upon by the Centers for Disease Control and Prevention and the American Academy of Periodontology. This classification requires evaluation of clinical attachment level (CAL) and probing depth (PPD). The North Carolina periodontal probe was used and the following criteria were considered: no periodontitis, mild periodontitis (2 interproximal sites with CAL 3 mm and 2 interproximal sites with PPD 4 mm, not on the same tooth, or 1 interproximal site with PPD 5 mm), moderate periodontitis (2 interproximal sites with CAL 4 mm, not on the same tooth, or 2 interproximal sites with PPD 5 mm, not on the same tooth), and severe periodontitis (2 interproximal sites with CAL 6 mm, not on the same tooth, and 1 interproximal site with PPD 5 mm). Results were recorded on the corresponding data collection form, which also included basic demographic information and information about the other covariates. The reliability of the method for measuring periodontitis using the CDC/AAP index was assessed in the pilot study through intra- and inter-rater calibration (a prior-trained examiner with a specialist professor in Periodontology from the "Antenor Orrego" Private University), with a complete sextant per patient. The same procedure was followed for the dental biofilm and BOP measurement. The intra-rater intraclass correlation for PPD and CAL was estimated at RHO=0.910 and RHO=0.995, respectively; and, for the presence of plaque and BOP, Kappa=0.820 and Kappa=0.938, respectively. Regarding the inter-rater intraclass correlation (examiner-specialist), RHO=0.904 and RHO=0.994 were adopted for PPD and CAL, respectively, and Kappa=0.825 and Kappa=0.934 for plaque presence and BOP, respectively. The collected data were entered into Excel and subsequently processed using IBM SPSS software version 29 (IBM, Armonk, NY, USA). Results are presented in frequency tables, bar graphs, and donut charts. The analysis of the association between the severity of periodontitis and CRC, along with other factors, was conducted using the bivariate Chi-square test, ordinal logistic regression, and binary logistic regression models, with a significance level of p < 0.05.
Results
The study included 320 patients, 155 male and 165 female, with mean ages of 58.2 (±11.7) and 55.6 (±11.1) years, respectively. The most common CRC stages were stage IV (48.1%) and stage III (39.4%), and the most common tumor locations were the rectum (40.0%) and sigmoid colon (36.3%), as shown in Figure 1.
Figure 1. Periodontitis severity by study group, clinical stage and tumor location in CRC patients.
Furthermore, in non-CRC patients, severe periodontitis was 26.3%, but in CRC patients, it was 50%. Table 1 presents the bivariate analysis of periodontitis severity with CRC and other factors.
An association was found between periodontitis severity and CRC (p=0.000), as well as with the other factors studied (p<0.05), except for T2DM (p=0.881). Severe periodontitis was more frequently present in patients aged 60-79 years (54.1%), female gender (59.8%), non-diverticulosis (64.8%) and non-T2DM patients (67.2%), patients with inadequate DPC (85.2%), and BOP >30% (75.4%). Table 2 shows the bivariate analysis, in which CRC was associated with periodontitis severity (p=0.000) and other factors (p<0.05), except gender (p=0.576).
In the CRC group, patients with severe periodontitis (50%), age 60-79 years (58.8%), diverticulosis (55%), and daily toothbrushing frequency 1 (73.8%) were predominantly observed. In the non-CRC group, a higher smoking rate was observed (79.4%); while in both groups, lower DPC was observed (85.6% for CRC and 66.9% for non-CRC), lower alcohol consumption (39.4% for CRC and 53.1% for non-CRC), and the majority of non-T2DM patients (61.3% for CRC and 73.8% for non-CRC). Tables 3 and 4 present the multivariate analysis using logistic regression, in which the effect of each factor is evaluated while adjusting for the other covariates, with no association between severe periodontitis and CRC observed in either model.
Table 3 shows that a higher probability of severe periodontitis in females (p=0.011), in non-smoking patients (p=0.044), with inadequate DPC (p=0.040), in heavy alcohol consumption compared to moderate consumption (p=0.014), as well as in those who do not brush their teeth daily (p=0.045) and in those who brushed twice a day (p=0.049), compared to those who brush three or more times. Greater severity was also observed in those with BOP >30% (p=0.031 for <10% and p=0.000 for 10-30%). While, as observed in Table 4, there was a higher probability of CRC only in patients aged 60-79 years (OR=0.192, p=0.000) and in non-smokers (OR=3.074, p=0.014).
Discussion
Periodontitis can lead to the release of inflammatory mediators in the blood, such as IL-6 and IL-1, triggering a systemic response. Likewise, opportunistic pathogenic bacteria such as F. nucleatum and P. gingivalis can reach the colon via the bloodstream, producing harmful metabolites that trigger maladaptive immune responses, inflammation, DNA damage, and genomic instability, thereby favoring the onset of pathological processes that could contribute to the development of CRC (1). In the present study, the most frequent CRC stages were IV and III, while in the study by Antonacci et al. (8) (Italy), stages II and III were the most prevalent. This difference may be due to European countries allocating more resources to early cancer prevention and diagnosis (3). Furthermore, these countries are leaders in research against this disease, promoting knowledge exchange and scientific development (9). On the other hand, in Peru, with a weakened healthcare system, cancer treatment is hampered by insufficient infrastructure, diagnostic delays, and inaccessible treatments in public facilities. Moreover, in public attention in Peru, dental care is precarious, with no health policy prioritizing its implementation for cancer patients. In the present study, more than 50% of CRC patients suffered from severe periodontitis at the time of evaluation. These results are consistent with the findings of Antonacci et al. (8) and Idrissi et al. (4), who reported prevalence of 76% and 46%, respectively. It is worth noting that the latter assessed periodontal disease, specifically self-reported gingivitis and periodontitis. The findings of the present study are concerning because cancer treatments such as chemotherapy and radiotherapy generate inflammatory processes in the oral cavity, delaying treatment and increasing medical costs (10). Direct tissue damage and inflammation, along with predisposing factors, can promote the progression of periodontitis if not promptly controlled (11). Likewise, preexisting periodontitis represents a high-risk chronic infectious focus in patients immunosuppressed due to cancer treatment, as it can trigger systemic infections, impair healing, aggravate mucositis, and increase the risk of osteoradionecrosis, especially in the presence of deep periodontal pockets (12). Moreover, limitations in oral hygiene, associated with pain, xerostomia, and tooth loss, negatively affect nutrition, quality of life, and patient recovery. Therefore, periodontal evaluation and treatment before the start of cancer therapy is essential to reduce complications and improve clinical outcomes. Using multivariate analysis, the present investigation found no association between periodontitis severity and CRC, in contrast to the bivariate analysis. It should be noted that multivariate analysis is more potent for simultaneously studying multiple associated factors and their effects. In this sense, bivariate analysis results should always be taken with caution. The results of the present study were consistent with the studies by Nwizu et al. (13), Michaud et al. (14), Kim et al. (15), and Pu et al. (16) However, they differ from the studies by Antonacci et al. (8), Idrissi et al. (4), Hu et al. (17), and Momen-Heravi et al. (18) These discrepancies are possibly due to multiple factors, such as comorbidities, biological characteristics of the tumor and access to health and food systems. The study design and the heterogeneity in the definition of periodontitis could also represent essential limitations. The standard method for diagnosing periodontitis is clinical and/or radiographic, while hospital records, even when specialist dentists perform them, may have certain limitations (2); the same occurs with self-reports, which may be subject to information bias, since patients may forget relevant information or give answers influenced by social norms (1). On the other hand, with respect to covariates, greater periodontitis severity was observed in females, nonsmokers, in those with inadequate DPC, heavy alcohol consumers, in those who do not brush their teeth daily, in those who brush their teeth twice a day, and in those with more than 30% of BOP sites. Women have higher concentrations of salivary inflammatory mediators, increased IL-1 and TNF- levels in the blood (19), and reduced estrogen levels, which negatively affect bone density and periodontal tissues. This hormonal deficiency can weaken dental support and promote inflammation. Heavy alcohol consumption promotes osteoclast formation and periodontal tissue damage (20); furthermore, it impairs neutrophil, macrophage, and T lymphocyte function, increasing susceptibility to infections and the progression of periodontitis (21). BOP, as a clinical indicator of periodontal inflammation, reflects disease activity and is associated with the progression of periodontitis (22). The presence of dental biofilm increases the risk of gingival inflammation and contributes to the loss of periodontal support tissues associated with periodontitis. Furthermore, there is a condition that affects the periodontal apparatus regardless of the presence of dental plaque, caused by neoplastic diseases (23). A strange finding was greater periodontitis severity in nonsmokers; however, these results should be interpreted with caution because these factors are covariates in the present study. Additionally, there was a higher probability of presenting CRC in patients aged 60-79 years and, strangely, also in nonsmokers; however, this last result should be taken with caution due to behavioral changes after the cancer diagnosis or because patients could be changing their responses to avoid criticism. The main limitation of the present study was that it did not allow for causal inference; instead, it only allowed for associations between variables, which should be further assessed in longitudinal studies. Furthermore, although some confounding factors were considered in the evaluation, the authors believe that additional factors may be involved; therefore, we recommend that these be identified and incorporated into future studies using multivariate analyses. On the other hand, because some data, such as alcohol consumption and smoking, were self-reported, they could be subject to the risk of information bias. The examiner's training and calibration are among the strengths of this study, which increase data reliability and ensure greater accuracy of results. Furthermore, the multivariate analysis, along with the large sample size, provides greater statistical power to reach conclusions, accounting for oral and medical factors that are more likely to exert confounding effects. Public health strategies should be established to promote the control of periodontitis in cancer patients, as well as longitudinal studies evaluating the presence of specific periodontopathogenic bacteria as a risk factor for CRC.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Espejo-Carrera RE Honores-Solano TM Ulloa-Cueva TV Caballero-Alvarado JA Minchón-Medina CA Asmat-Abanto AS Periodontitis as a risk factor for colorectal cancer: systematic review and meta-analysis Med Oral Patol Oral Cir Bucal 2025304 e 568e 577.4019211610.4317/medoral.27118 PMC 12225763 · doi ↗ · pubmed ↗
- 2Asmat-Abanto AS Espejo-Carrera RE Honores-Solano TM Del Castillo-Huertas OM Caballero-Alvarado JA Minchón-Medina CA Is periodontitis a risk factor for ischemic stroke?: Systematic review and meta-analysis J Clin Exp Dent 2025173 e 329e 340.4023114610.4317/jced.62538 PMC 11994202 · doi ↗ · pubmed ↗
- 3Asmat-Abanto AS Portocarrero-Reyes A Espejo-Carrera RE Minchón-Medina CA Timaná-Palacios DJ Bibliometric analysis in Scopus of scientific production on the relationship between periodontitis and gastrointestinal cancer (2014 - 2023)Med Oral Patol Oral Cir Bucal 2025303 e 422e 430.3986408410.4317/medoral.26969 PMC 12019650 · doi ↗ · pubmed ↗
- 4Idrissi Janati A Karp I Latulippe JF Charlebois P Emami E Periodontal disease as a risk factor for sporadic colorectal cancer: results from COLDENT study Cancer Causes Control 2022333463472.3507992410.1007/s 10552-021-01541-y PMC 8821510 · doi ↗ · pubmed ↗
- 5Oh SY Park JY Yang KM Jeong SA Kwon YJ Jung YT Oncologic outcomes of surgically treated colorectal cancer in octogenarians: a comparative study using inverse probability of treatment weighting (IPTW)BMC Gastroenterol 2025251276.4025457210.1186/s 12876-025-03882-3PMC 12010669 · doi ↗ · pubmed ↗
- 6Eskandari-Malayeri F Rezeai M Narimani T Esmaeil N Azizi M Investigating the effect of Fusobacterium nucleatum on the aggressive behavior of cancer-associated fibroblasts in colorectal cancer Discov Oncol 2024151292.3903044510.1007/s 12672-024-01156-0PMC 11264641 · doi ↗ · pubmed ↗
- 7Ajalcriña-Martensen AA Minchón-Medina CA Astigueta-Perez J Gamboa-Vicente WG Ganoza-Larrea LJ Asmat-Abanto AS Periodontitis associated with prostate cancer and other urological cancers in patients over 50 years of age: a cross-sectional study Med Oral Patol Oral Cir Bucal 2025305 e 681e 689.4081813810.4317/medoral.27179 PMC 12395600 · doi ↗ · pubmed ↗
- 8Antonacci A Bizzoca C Barile G Andriola V Vincenti L Bartolomeo N Evaluation of Periodontitis and Fusobacterium nucleatum Among Colorectal Cancer Patients: An Observational Cross-Sectional Study Healthcare (Basel)202412212189.3951740110.3390/healthcare 12212189 PMC 11545387 · doi ↗ · pubmed ↗