Recurrent Hyponatremia With Central Endocrine Dysfunction: A Diagnostic Challenge
Robert Li, Harpreet Sidhu, Jennifer Y Han

TL;DR
A man with chronic hyponatremia and endocrine issues was found to have a pituitary mass, which was successfully treated, resolving his symptoms.
Contribution
This case demonstrates that pituitary masses can mimic SIADH and highlights the importance of structural evaluation in such patients.
Findings
A suprasellar cystic mass was identified as the cause of hyponatremia and endocrine dysfunction.
Transsphenoidal cyst drainage resolved hyponatremia and normalized pituitary function.
Timely intervention reversed endocrine abnormalities and sodium levels.
Abstract
A 55-year-old man with a history of chronic hyponatremia presented with recurrent nausea, vomiting, and severe hyponatremia. Initial evaluation revealed features consistent with the syndrome of inappropriate antidiuretic hormone secretion (SIADH), including hypotonic hyponatremia with inappropriately concentrated urine. Further workup demonstrated concurrent central hypothyroidism and hypogonadotropic hypogonadism, prompting neuroimaging. MRI identified a 1.7 cm suprasellar cystic mass compressing the pituitary infundibulum. The patient underwent transsphenoidal cyst drainage, resulting in the resolution of hyponatremia and normalization of pituitary function. This case highlights the importance of evaluating structural pituitary pathology in patients with hyponatremia and multiple endocrine abnormalities, demonstrating how compressive lesions can mimic idiopathic SIADH. The rapid…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
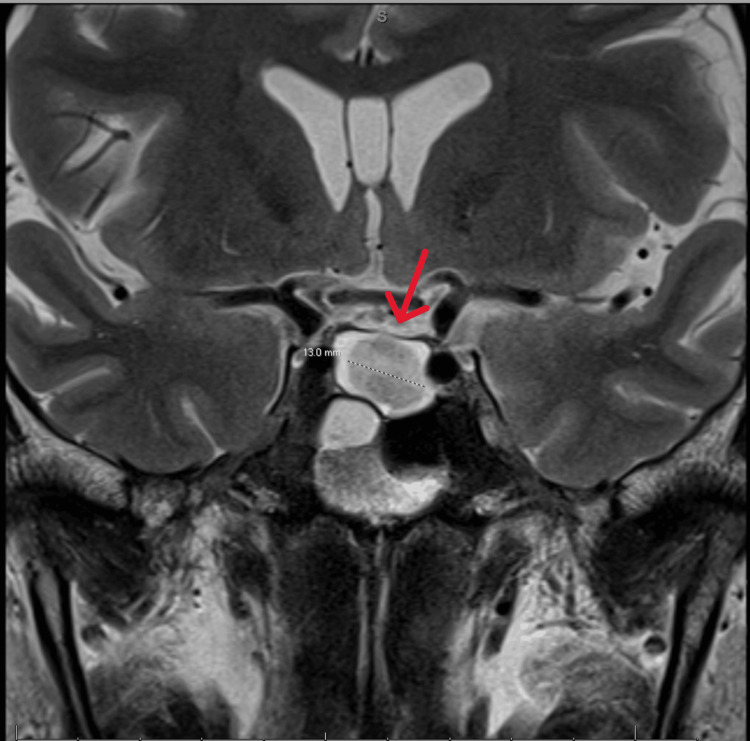 Figure 1
Figure 1| Latest Reference Range and Units | May, 22, 2024, 16:56 | May 23, 2024, 02:01 | May 23, 2024, 09:51 | May 23, 2024, 10:21 | |
| Na | 134-146 mmol/L | 118 (LL) | 118 (LL) | 116 (LL) | - |
| Osmolality, Serum | 280-300 mOsm/kg | 239 (LL) | - | - | - |
| Sodium, Urine Random | Not established mmol/L | - | - | - | 134 |
| Osmo Urine | 500-800 mOsm/kg | - | - | - | 488 (L) |
| Latest Reference Range and Units | September 13, 2023, 04:49 | September 13, 2023, 13:01 | September 13, 2023, 13:23 | September 13, 2023, 13:27 | September 14, 2023, 04:29 | |
| Na | 134-146 mmol/L | 127 (L) | 128 (L) | - | - | 128 (L) |
| Osmolality, Serum | 280-300 mOsm/kg | 260 (L) | - | - | - | - |
| Sodium, Urine Random | Not established mmol/L | - | - | - | 81 | - |
| Osmolality, Urine | 500-800 mOsm/kg | - | - | 317 (L) | - | - |
| January 6, 2023 | September 13, 2023 | February 23, 2024 | May 17, 2024 | May 22, 2024 | May 23, 2024 | Reference Range and Units | ||
| TSH | 1.52 | 0.497 (L) | 1.151 | 0.387 (L) | 0.5 (L) | 0.33 (L) | 0.550-4.780 uIU/mL | |
| Free T4 | - | 0.58 (L) | 0.92 | - | 0.74 (L) | 0.66 (L) | 0.89-1.76 ng/dL | |
| January 6, 2023 | September 1, 2023 | September 13, 2023 | November 8, 2023 | February 23, 2024 | Reference Range | |
| Testosterone | 177 (L) | <3 (L) | 38 (L) | 141.9 (L) | 177 (L) | 264-916 ng/dL |
| Luteinizing hormone (LH) | - | 6.5 | - | - | - | 1.8-8.6 mIU/mL |
| Follicle-stimulating hormone (FSH) | - | 9 | - | - | - | 1.5-12.4 mIU/mL |
| Test | October 21, 2024 | Reference Range |
| Sodium | 141 mmol/L | 136-145 mmol/L |
| Potassium | 4.3 mmol/L | 3.5-5.1 mmol/L |
| Chloride | 108 mmol/L | 98-107 mmol/L |
| CO2 | 26 mmol/L | 22-29 mmol/L |
| Cortisol | 7.2 mcg/dL | No Ref Range |
| Free T4 | 1.09 ng/dL | 0.7-1.48 ng/dL |
| Thyroid-stimulating hormone (TSH) | 0.560 μIU/mL | 0.350-4.940 μIU/mL |
| Luteinizing Hormone (LH) | 4.41 mIU/mL | No Ref Range |
| Prolactin | 7.80 ng/mL | 3.46-19.40 ng/mL |
| Testosterone Total | 371 ng/dL | 240-950 ng/dL |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsElectrolyte and hormonal disorders · Neurological and metabolic disorders · Adrenal Hormones and Disorders
Introduction
Hyponatremia, a common electrolyte disorder, has a multifactorial etiology that often presents diagnostic challenges [1]. The syndrome of inappropriate antidiuretic hormone secretion (SIADH) is a frequent cause of hyponatremia and is characterized by impaired free water excretion due to inappropriate vasopressin secretion [2]. When hyponatremia occurs together with other endocrine abnormalities, particularly pituitary hormone deficiencies, clinicians should be suspicious of central causes involving the hypothalamic-pituitary axis [3].
The pituitary gland's location and complexity make it vulnerable to mass effects from tumors, cysts, or other structural lesions [4]. Such lesions may disrupt normal hypothalamic-pituitary signaling and lead to specific patterns of hormonal dysfunction [5], including central hypothyroidism, characterized by low free thyroxine with inappropriately low or normal thyroid-stimulating hormone (TSH), and hypogonadotropic hypogonadism, characterized by low sex steroids with inappropriately low or normal gonadotropins [6].
Diagnosis and treatment of patients with hyponatremia and evidence of pituitary dysfunction requires integration of clinical presentation, biochemical testing, and neuroimaging findings [7]. Though SIADH may initially appear as an isolated disorder, the presence of additional endocrine abnormalities should prompt evaluation for structural pituitary lesions [8]. This clinical scenario underscores the importance of considering pituitary pathology in the differential diagnosis of persistent hyponatremia, particularly when it occurs in association with other hormonal deficiencies.
Case presentation
A 55-year-old man with a medical history significant for chronic hyponatremia, gout, hypogonadism, and hypothyroidism presented with nausea, vomiting, acid reflux, and severe hyponatremia (sodium 118 mmol/L). Laboratory testing on admission (Table 1) revealed low serum osmolality (239 mOsm/kg) with inappropriately elevated urine sodium (134 mmol/L) and urine osmolality (488 mOsm/kg), which is consistent with SIADH.
The pattern of laboratory abnormalities mirrored a prior hospitalization a year earlier (Table 2), where he was similarly diagnosed with SIADH and treated with two liters per day fluid restriction and 2 g per day NaCl tablets.
Further evaluation revealed a history of long-standing central hypothyroidism, with low thyroid-stimulating hormone (TSH) and free T4 (Table 3), and hypogonadotropic hypogonadism (Table 4), with testosterone levels as low as <3 ng/dL and inappropriately normal gonadotropin (luteinizing hormone (LH), follicle-stimulating hormone (FSH)) levels.
The combination of central hypothyroidism, central hypogonadism, and SIADH raised suspicion of a pituitary etiology. MRI pituitary with and without contrast (Figure 1) identified a 1.7 cm suprasellar mass in the posterior pituitary, exhibiting T1 hyperintensity, suggestive of proteinaceous or hemorrhagic content. The mass caused anterior displacement of the infundibulum and the anterior pituitary, which likely accounted for the patient’s hormonal abnormalities.
MRI pituitary with and without contrast showing a suprasellar mass in the posterior pituitaryPosterior pituitary mass (red arrow) measuring 1.6x1.6x1.7 cm with displacement of the infundibulum and anterior pituitary gland. There is a mass effect on the infundibulum. Differential diagnosis includes craniopharyngioma, neurosarcoidosis versus pituitary apoplexy.
Neurosurgery was consulted and the neurosurgery team performed a trans-nasal trans-sphenoidal (TNTS) drainage of the suprasellar cyst. Postoperatively, the patient’s hyponatremia resolved and endocrine function normalized. Follow-up laboratory testing (Table 5) four months later showed normalization of sodium levels, free T4, TSH, and testosterone, confirming restoration of pituitary-hypothalamic axis function.
Discussion
This case demonstrates important aspects of hyponatremia and pituitary dysfunction. The patient's chronic hyponatremia, initially diagnosed as SIADH, was ultimately found to be secondary to mass effect from a pituitary mass compressing the infundibulum (pituitary stalk).
Pituitary lesions compressing the infundibulum can cause hyponatremia through several mechanisms, as given below:
SIADH-like mechanism:* *Inappropriate ADH secretion as a result of compression of the infundibulum can impair normal inhibitory signals to the posterior pituitary [9]. This form is often termed "secondary SIADH" because it results from structural interference with hypothalamic-pituitary signaling [8]. Key features include impaired osmotic suppression of antidiuretic hormone (ADH) [10] and euvolemic hyponatremia with inappropriately concentrated urine (urine osmolality >100 mOsm/kg despite low serum osmolality) [2].
Secondary adrenal insufficiency (cortisol deficiency):* *Disruption of adrenocorticotropic hormone (ACTH) secretion from compression of the anterior pituitary or infundibulum can lead to glucocorticoid deficiency [4]. Since cortisol normally inhibits ADH release, its deficiency can result in hyponatremia from uninhibited ADH secretion [11] as well as impaired free water excretion [12].
Combined anterior and posterior pituitary dysfunction:* *Pituitary masses can in some cases cause a triphasic response (often seen after pituitary surgery or trauma): (a) initial ADH surge (acute hyponatremia due to excessive ADH release from injured neurons); (b) diabetes insipidus (DI) (if ADH-secreting neurons are destroyed); (c) chronic SIADH (if aberrant ADH release resumes from damaged axons) [9].
Differentiating SIADH from adrenal insufficiency is critical to the evaluation of hyponatremia. This can be done by measuring a morning cortisol. A morning cortisol <3 µg/dL suggests adrenal insufficiency, while normal or high cortisol suggests SIADH-like physiology [3]. If a pituitary lesion is suspected, an MRI is used as a diagnostic tool [5].
Treatment depends on the mechanism of hyponatremia. If the etiology of the hyponatremia is SIADH-like, fluid restriction, salt tablets, or vaptans are the preferred treatment [8]. If the hyponatremia arises from adrenal insufficiency, glucocorticoid replacement is needed [4]. Definitive management involving surgical cyst drainage or adenoma removal often corrects both the hyponatremia and any pituitary hormonal deficits [7].
In this case, the concurrent presence of central hypothyroidism and hypogonadotropic hypogonadism along with an SIADH clinical picture strongly suggested hypothalamic-pituitary dysfunction [7]. The patient's hyponatremia and pituitary hormone deficiencies completely resolved following surgical drainage of the pituitary cyst, which confirmed the diagnosis of the pituitary cyst causing secondary SIADH and hypopituitarism. The successful resolution of both hyponatremia and hormonal deficiencies after surgical intervention underscores the importance of treating the underlying pathology in such cases [7]. While hormone replacement can be used to manage symptoms and SIADH can be treated with fluid restriction and salt replacement, accurate diagnosis and definitive treatment may completely reverse the endocrine abnormalities, as seen in this patient.
Conclusions
This case emphasizes the importance of a comprehensive endocrine evaluation including early and appropriate neuroimaging in patients with persistent hyponatremia. When multiple hormonal abnormalities coexist, biochemical and radiological workup for pituitary pathology needs to be performed. With appropriate surgical intervention of the underlying pituitary pathology, a potential for complete recovery is possible.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Hyponatremia N Engl J Med AdroguéHJ Madias NE 1581158934220001082407810.1056/NEJM 200005253422107 · doi ↗ · pubmed ↗
- 2Clinical practice. The syndrome of inappropriate antidiuresis N Engl J Med Ellison DH Berl T 2064207235620071750770510.1056/NEJ Mcp 066837 · doi ↗ · pubmed ↗
- 3Clinical review: current state and future perspectives in the diagnosis of diabetes insipidus: a clinical review J Clin Endocrinol Metab Fenske W Allolio B 342634379720122285533810.1210/jc.2012-1981 · doi ↗ · pubmed ↗
- 4Hormonal replacement in hypopituitarism in adults: an Endocrine Society Clinical Practice Guideline J Clin Endocrinol Metab Fleseriu M Hashim IA Karavitaki N Melmed S Murad MH Salvatori R Samuels MH 3888392110120162773631310.1210/jc.2016-2118 · doi ↗ · pubmed ↗
- 5Pituitary incidentaloma: an endocrine society clinical practice guideline J Clin Endocrinol Metab Freda PU Beckers AM Katznelson L Molitch ME Montori VM Post KD Vance ML 8949049620112147468610.1210/jc.2010-1048 PMC 5393422 · doi ↗ · pubmed ↗
- 6Hypopituitarism Lancet Higham Higham CECE Johannsson Johannsson GG Shalet Shalet SMSM 2403241538820162704106710.1016/S 0140-6736(16)30053-8 · doi ↗ · pubmed ↗
- 7Pituitary-tumor endocrinopathies N Engl J Med Melmed S 93795038220203213081510.1056/NEJ Mra 1810772 · doi ↗ · pubmed ↗
- 8Diagnosis, evaluation, and treatment of hyponatremia: expert panel recommendations Am J Med Verbalis JG Goldsmith SR Greenberg A Korzelius C Schrier RW Sterns RH Thompson CJ 042126201310.1016/j.amjmed.2013.07.00624074529 · doi ↗ · pubmed ↗