Efficacy of a Superficial Cervical Plexus Block as an Alternative to General Anesthesia for Mandibular and Perimandibular Surgical Procedures: A Systematic Review
Ojasvee Hiran, Tejraj Kale, Radhika Pathak, Rahul Bichile, Kairav Vadher

TL;DR
This review finds that a superficial cervical plexus block is a safe and effective alternative to general anesthesia for certain jaw surgeries.
Contribution
The study systematically evaluates the efficacy and safety of superficial cervical plexus blocks as an alternative to general anesthesia in mandibular and perimandibular surgeries.
Findings
Superficial cervical plexus blocks provided effective intraoperative and postoperative analgesia in 9 studies involving 164 patients.
Patients receiving the block had lower postoperative analgesic requirements and pain scores compared to general anesthesia or local infiltration.
The block showed high success rates, patient satisfaction, and negligible complications in case series and reports.
Abstract
Any oral and maxillofacial surgery often requires reliable anesthesia to ensure analgesia, patient comfort, and surgical efficiency. While general anesthesia is the traditional choice, it carries risks of cardiopulmonary complications, prolonged recovery, and higher resource utilization. A superficial cervical plexus block has emerged as a potential alternative, offering simplicity, safety, and cost-effectiveness. This systematic review aimed to evaluate the efficacy and safety of the superficial cervical plexus block as an alternative to general anesthesia in mandibular and perimandibular, oral, and maxillofacial surgical procedures. Following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2020 guidelines, a comprehensive search of PubMed, Cochrane, Google Scholar, and Wiley (2000-2024) was conducted. Eligible studies included randomized controlled…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
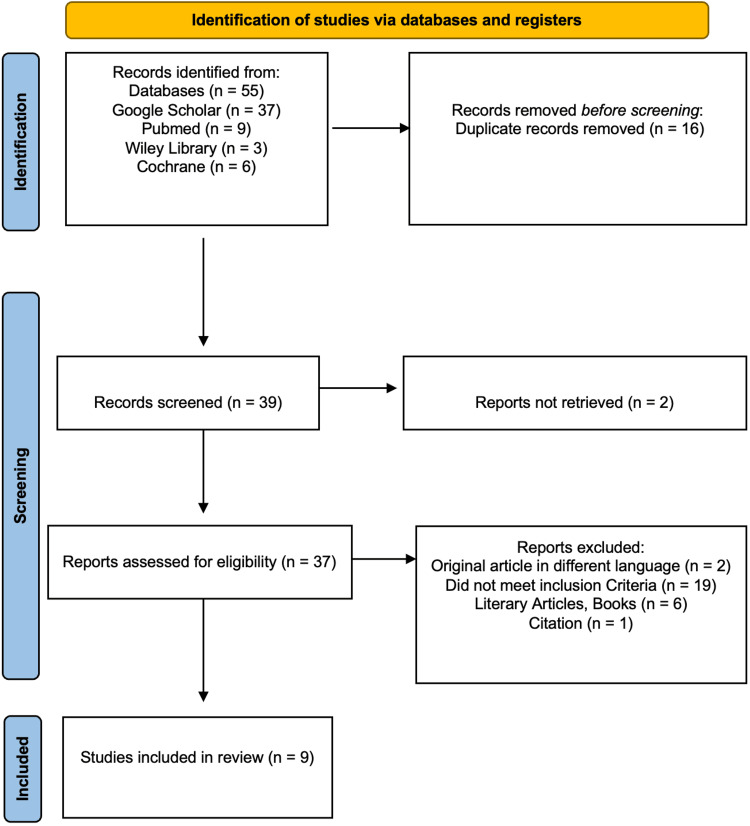 Figure 1
Figure 1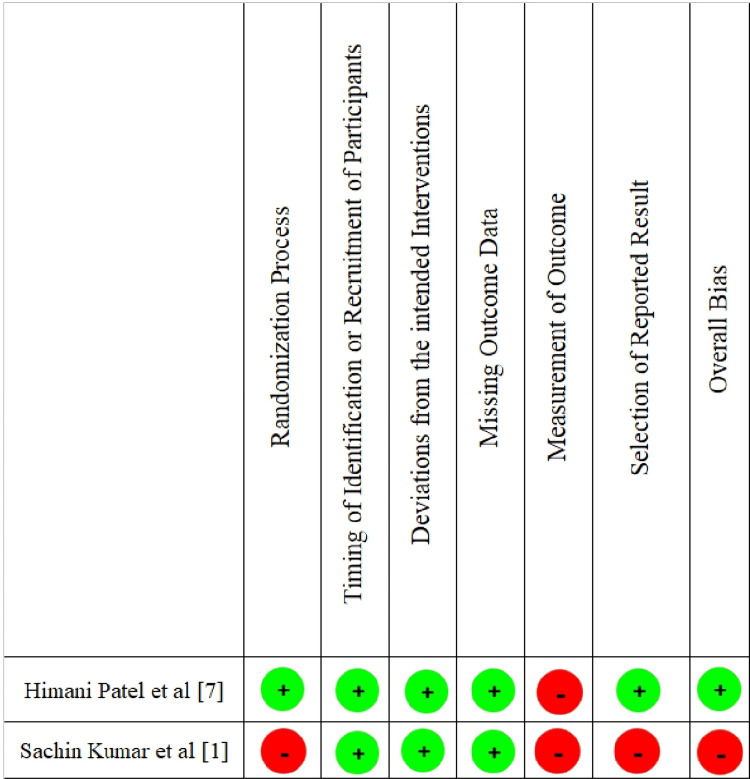 Figure 2
Figure 2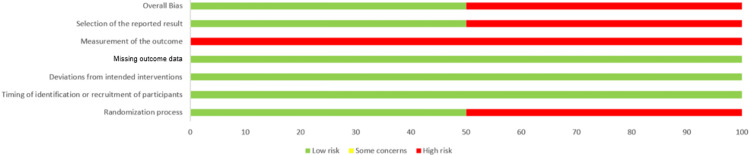 Figure 3
Figure 3| PICO criteria | |
| P (participants) | Patient undergoing mandibular and perimandibular surgeries under superficial cervical plexus block between the ages of 18 and 90 years |
| I (intervention) | Superficial cervical plexus block for mandibular and perimandibular surgeries |
| C (comparison) | With or without a control group |
| Comparison can be with general anesthesia | |
| O (outcome) | Perioperative pain and perioperative complications |
| Inclusion criteria | Exclusion criteria |
| 1. Studies including oral and maxillofacial surgical procedures performed under SCPB | 1. Articles not fulfilling the inclusion criteria |
| 2. Studies published between 2000 and 2024 | 2. Studies done in any language other than English |
| 3. Study design: randomized controlled trials (RCTs), non-RCTs, clinical trials, retrospective studies, case series, case reports, or any clinical cross-sectional study | 3. Opinion articles, letters |
| 4. Studies that assess preoperative pain and other complications | 4. Animal studies, in vivo studies |
| 5. Studies involving supplemental blocks like inferior alveolar nerve block, lingual nerve block, long buccal nerve block, and local infiltration | 5. Studies involving deep/intermediate form of cervical plexus block |
| Serial no. | Study-author name and year | Study design | Sample size | Procedures | Control group | Intervention | Outcome: perioperative analgesia | Outcome: complications | Conclusion | |||||
| 1 | Singh et al., 2020 [ | Prospective clinical trial | 24 patients: 16 females, 8 males | Incision and drainage | No control group | SCPNB with trigeminal local mandibular nerve blocks | Intraoperative VAS score: ranged from 0 to 8 with a mean of 1.5 ± 1.87 | 1 patient was taken up for GA due to unbearable pain | SCPNB with trigeminal nerve block is more effective in mandibular and perimandibular cases with a low rate of complications | |||||
| 2 | Patel et al., 2023 [ | Comparative randomized controlled trial | Group A: 30 patients; Group B: 30 patients | Procedures not specified | Group A: sedation with systemic GA | Group B: sedation with SCPNB | Intraoperative total postoperative rescue analgesic requirement in 24 hours in Group A (97.5 ± 13.75 µg and 2,566.66 ± 504 mg) and Group B (70.16 ± 13.09 µg and 833.33 ± 874.28 mg); p-value was <0.001. VAS score: 6 hours postoperatively Group A > 4 and Group B < 4 (p-value < 0.005). Postoperatively 16, 20, and 24 hours, insignificant difference between 2 groups with a p-value > 0.05 | Group A: 2 patients had nausea and vomiting postoperatively; Group B: no complications were reported | It can be concluded that in balanced anesthesia technique, superficial cervical plexus nerve block gives better results in immediate postoperative analgesia and is safe with a significantly lower rate of complications as compared to GA | |||||
| 3 | Kumar et al., 2023 [ | Prospective randomized clinical trial | Category A: 25 patients; category B: 23 patients | 1. Incision and drainage; 2. cyst enucleation; 3. open reduction and internal fixation | Category A: combination of local infiltration and regional anesthesia | Category B: regional anesthesia with SCPNB | Waiting period for analgesic requirement postoperatively: Category A: 75.12 ± 14.24 minutes; Category B: 137.23 ± 32.43 minutes. p-value: 0.0312. VAS score: duration (in mins): at 15 and 30 minutes (p ≤ 0.05); at 60 and 120 minutes (p > 0.01) | No complications reported in both groups | Postoperative analgesia is better with SCPNB; increased duration for the requirement of analgesics during the recovery period | |||||
| 10 | 15 | 30 | 60 | 120 | ||||||||||
| Category A | 4 | 4 | 3 | 2 | 1 | |||||||||
| Category B | 4 | 3 | 2 | 2 | 1 | |||||||||
| 4 | Kanthan, 2016 [ | Case series | 10 patients: 6 males, 4 females | 1. Incision and drainage; 2. open reduction and internal fixation; 3. cyst enucleation; 4. cervical lymph node biopsy | No control group | SCPNB with supplemental nerve block | Not assessed | No complications reported | SCPNB with concomitant mandibular nerve and/or long buccal nerve block has a high success rate, low complication rate, and high patient acceptability as shown in the study | |||||
| 5 | Hakim et al., 2019 [ | Case series | 10 patients: 6 males, 4 females | 1. Incision and drainage; 2. open reduction and internal fixation; 3. cyst enucleation; 4. submandibular lymph node biopsy | No control group | SCPNB with supplemental nerve block | Not assessed | No complications reported | SCPNB with concomitant mandibular nerve and/or long buccal nerve block has a high success rate, low complication rate, and high patient acceptability as shown in the study | |||||
| 6 | Zhao et al., 2024 [ | Case series | 7 patients: 4 females, 3 males | Excision of tumors in submandibular and sublingual regions | No control group | SCPNB with local infiltration anesthesia | Postoperative analgesic effect lasted for 6 hours | No complications were recorded | Ultrasound-guided SCPNB combined with local infiltration is a simple, safe, and effective anesthesia method for some patients with specific diseases, especially elderly patients with poor general condition who are at risk of GA | |||||
| 7 | Saripalli et al., 2022 [ | Case presentation | 1 male | Open reduction and internal fixation | No control group | SCPNB with supplemental nerve block | Effect of analgesia lasted from 15 mins after injection till 6 hours postoperatively | No complications | From this study, it can be concluded that mandibular fracture fixation can be performed under SCPNB and local anesthesia effectively without any complications | |||||
| 8 | Shteif et al., 2008 [ | Case report | 3 patients: 1 male, 2 females | Incision and drainage | No control group | SCPNB with long buccal or inferior alveolar nerve block | Not assessed | No complications | SCPNB with concomitant mandibular nerve and/or long buccal nerve block has a high success rate, low complication rate, and high patient acceptance rate in cases of submandibular and submental space infection | |||||
| 9 | Peksöz et al., 2022 [ | Case report | 1 male | Lipoma excision | No control group | SCPNB nerve block | Not assessed | No complications | In the short-term surgery of soft tissue lesions in the lesser occipital nerve and great auricular nerve dermatome areas, anesthesia can be achieved through a superficial cervical plexus block | |||||
| JBI questionnaire for non-RCTs | Singh et al., 2020 [ |
| 1. Is it clear in the study what the “cause” is and what the “effect” is (i.e., there is no confusion about which variable comes first)? | Yes |
| 2. Was there a control group? | No |
| 3. Were participants included in any comparisons similar? | Yes |
| 4. Were the participants included in any comparisons receiving similar treatment/care, other than the exposure or intervention of interest? | No |
| 5. Were there multiple measurements of the outcome, both pre and post the intervention/exposure? | No |
| 6. Were the outcomes of participants included in any comparisons measured in the same way? | Yes |
| 7. Were outcomes measured in a reliable way? | Yes |
| 8. Was follow-up complete, and if not, were differences between groups in terms of their follow-up adequately described and analyzed? | Yes |
| 9. Was appropriate statistical analysis used? | Yes |
| Overall score | 66.60% |
| JBI questionnaire for case series | Kanthan, 2016 [ | Zhao et al., 2024 [ | Hakim et al., 2019 [ |
| 1. Were there clear criteria for inclusion in the case series? | Yes | No | Yes |
| 2. Was the condition measured in a standard, reliable way for all participants included in the case series? | Unclear | Unclear | Unclear |
| 3. Were valid methods used for identification of the condition for all participants included in the case series? | Yes | Yes | Yes |
| 4. Did the case series have consecutive inclusion of participants? | No | Yes | No |
| 5. Did the case series have complete inclusion of participants? | Yes | Yes | Yes |
| 6. Was there clear reporting of the demographics of the participants in the study? | Yes | Yes | Yes |
| 7. Was there clear reporting of clinical information of the participants? | Yes | Yes | Yes |
| 8. Were the outcomes or follow-up results of cases clearly reported? | Yes | Yes | Yes |
| 9. Was there clear reporting of the presenting site(s)/clinic(s) demographic information? | Yes | Yes | Yes |
| 10. Was statistical analysis appropriate? | NA | NA | NA |
| Overall score | 70% | 70% | 70% |
| JBI questionnaire for case reports | Saripalli et al., 2022 [ | Shteif et al., 2008 [ | Peksöz et al., 2022 [ |
| 1. Were the patient’s demographic characteristics clearly described? | Yes | Yes | Yes |
| 2. Was the patient’s history clearly described and presented as a timeline? | Yes | Yes | Yes |
| 3. Was the current clinical condition of the patient on presentation clearly described? | Yes | Yes | Unclear |
| 4. Were diagnostic tests or assessment methods and the results clearly described? | Yes | Yes | Yes |
| 5. Was the intervention(s) or treatment procedure(s) clearly described? | Yes | Yes | Yes |
| 6. Was the post-intervention clinical condition clearly described? | Yes | Unclear | Unclear |
| 7. Were adverse events (harms) or unanticipated events identified and described? | NA | Unclear | Unclear |
| 8. Does the case report provide takeaway lessons? | Yes | Yes | Yes |
| Overall score | 87% | 75% | 62.50% |
| Outcome measure | Studies reporting | Summary across studies |
| VAS pain scores (intra-/postoperative) | Patel et al. [ | Mean intraoperative VAS: 1.5 ± 1.87 (Singh et al.); postoperative VAS lower with SCPB vs. GA at 6 h (Patel et al., p = 0.005); duration-specific reductions (Kumar et al., p < 0.05 at multiple timepoints) |
| Intraoperative fentanyl requirement | Patel et al. [ | Lower in the SCPB group (70.16 ± 13.09 μg) vs. GA (97.5 ± 13.75 μg, p = 0.001) |
| Postoperative rescue analgesics | Patel et al. [ | Lower in SCPB: 833 ± 874 mg (Patel et al., p = 0.001); waiting period 137 ± 32 min (Kumar et al.) vs. 75 ± 14 min control (p = 0.031) |
| Hemodynamic stability (pulse, SpO2, ECG) | Patel et al. [ | Stable intra-/postoperatively across studies; no significant changes reported |
| Onset/duration of anesthesia | Kumar et al. [ | Onset effective; duration extended postoperative analgesia |
| GA conversion rate | Singh et al. [ | 1/24 patients (4.2%) due to pain |
| Major complications | All 9 studies | None reported (0% across 140+ patients); minor PONV in GA control only (Patel et al.) |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAnesthesia and Pain Management · Dental Anxiety and Anesthesia Techniques · Anesthesia and Sedative Agents
Introduction and background
In order to carry out any procedure in the mandibular and perimandibular regions without pain, anesthesia is of utmost importance, which also helps in anxiety management among patients. The use of anesthesia in dental procedures dates back to 1846 in Boston, when Dr. William T.G. Morton performed the first painless dental extraction using ether. Various modes of providing anesthesia are available based on the category of procedure to be conducted [1].
Traditionally, general anesthesia (GA) has been the mainstay for achieving adequate analgesia, amnesia, and muscle relaxation in major maxillofacial procedures. However, GA carries inherent risks, especially in patients with comorbidities, and often requires more extensive perioperative care, advanced monitoring, and prolonged recovery time. In contrast, regional anesthetic techniques have garnered growing interest due to their potential advantages, including fewer systemic complications, reduced need for airway management, lower postoperative pain scores, and shorter hospital stays [2].
Among the regional techniques, the superficial cervical plexus block (SCPB) has emerged as a promising alternative. The superficial cervical plexus is formed by the ventral rami of the C2-C4 spinal nerves and emerges at the posterior border of the sternocleidomastoid muscle at the level of C3-C4 cervical vertebrae, providing sensory innervation to the anterolateral neck and lower face. The SCPB is performed by infiltrating local anesthetic along this anatomical plane, typically at the midpoint of the sternocleidomastoid's posterior border, targeting the four main terminal branches: lesser occipital, greater auricular, transverse cervical, and supraclavicular nerves. Unlike the deep cervical plexus block, which targets motor and deeper sensory structures, SCPB is a superficial technique with a favorable safety profile, avoiding risks associated with neuraxial or vascular puncture. This block can provide effective analgesia for superficial surgeries of the neck and lower face and, when combined with supplementary local infiltration or other regional blocks, may extend coverage to mandibular and perimandibular procedures [3].
SCPB has been successfully employed in a range of head and neck surgeries [4]. However, its utility in oral and maxillofacial surgery (OMFS) has only recently begun to gain attention. Preliminary studies and case reports suggest that SCPB, either alone or in combination with other local or regional blocks, can offer effective intraoperative and postoperative analgesia for procedures such as mandibular fracture fixation, submandibular gland excision, and superficial soft tissue surgeries of the face and neck [5]. The efficacy of SCPB in OMFS can be assessed by multiple parameters: quality of intraoperative analgesia, need for conversion to GA or additional sedation, patient satisfaction, postoperative pain control, complication rates, and time to recovery.
This review aims to evaluate the efficacy of the SCPB as an alternative to GA in OMFS. By aggregating findings from various studies, it will provide insights into the safety, effectiveness, and feasibility of SCPB in different clinical scenarios, thus helping clinicians make informed decisions about anesthetic planning.
The primary objectives of this review are to assess the effectiveness of SCPB in providing adequate anesthesia for OMFS procedures, to compare intraoperative and postoperative outcomes between SCPB and GA, and to evaluate patient complication rates associated with SCPB. By addressing these objectives, this review seeks to contribute to evidence-based practice in maxillofacial anesthesia, potentially broadening the use of SCPB in both routine and specialized clinical settings.
Review
Materials and methods
Protocol and Registration
The study followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines in the 2020 checklist. The review has been officially documented within PROSPERO under registration number CRD42024590655.
Eligibility Criteria
The PICO criteria for this review are presented in Table 1.
The eligibility criteria are presented in Table 2.
Information Source
A thorough electronic search was done using databases like PubMed, Google Scholar, Wiley Library, and Cochrane from January 1, 2000, to July 2024. Titles and abstracts were screened, and if the full text was not available for a potential study, the author was contacted for the same. Cross-references and citations from similar studies were also assessed. Studies other than English language were excluded. We resorted to manual methods for literature search when the full texts of relevant studies were not accessible via electronic databases.
Search Strategy
The keywords used for the literature search are “superficial cervical plexus block”, “SCPB”, “regional anaesthesia”, “oral and maxillofacial surgery”, “mandibular surgery”, “ mandibular fracture”, and “incision and drainage”. These keywords were clubbed, and an advanced search was done in each database using these keywords: [“SCPB” AND “mandibular surgery”], [“SCPB” and “mandibular fracture”], [“SCPB AND incision and drainage], [“regional anaesthesia” AND “maxillofacial procedures”], [“regional anaesthesia” AND “maxillofacial procedures” AND “mandibular fracture”], [“SCPB” AND “mandibular surgery” AND “condylar fracture”], and [“SCPB” AND “mandibular surgery” AND “Incision and drainage”].
Study Selection
Preliminary screening identified 55 studies from various databases, comprising 37 articles from Google Scholar, nine articles from PubMed, three articles from Wiley Library, and six articles from Cochrane, out of which 16 articles were removed as duplicates. Of the remaining 39 studies searched to screen for title and abstract, two articles could not be retrieved. Out of the remaining 37 articles, 28 were excluded, including 19 articles that did not meet the inclusion criteria, two articles written in languages other than English, one article that was a citation, and six articles that were books and literary articles. Thus, this systematic review included nine studies. Two independent reviewers screened titles and abstracts, followed by full-text articles, using a standardized screening form implemented in Microsoft Excel (Microsoft Corp., Redmond, WA, USA). Disagreements were resolved through discussion to reach consensus; a third reviewer was available for arbitration but was not required.
Data Extraction
Data screening was done by two reviewers individually. The first screening was done on the basis of the title and abstract. If enough information was not available, then full-text articles were obtained to review the studies. Upon acquiring the full texts, a comprehensive review was conducted by reading each article in its entirety to determine whether it met the inclusion criteria. Data extraction was conducted independently and in duplicate by two reviewers using a pre-piloted standardized Microsoft Excel template capturing authors' name and year (name of the first author and year of article publication), study design (randomized controlled trials (RCTs), non-RCTs, prospective clinical studies, case series, and case reports), sample size (number of patients included in the study), age (mean age group of the patients involved), procedure, intervention (SCPB along with type of local nerve block used), comparison (with or without any control group), analgesic effect (perioperative pain score using the Visual Analogue Scale (VAS)), other outcomes (complications such as nausea, vomiting, conversion to GA, and baseline vital parameters), results (results of each study), and conclusion (conclusions of each study, including limitations if mentioned). Any discrepancies were resolved by consensus between the extractors.
Risk of Bias Assessment
For RCTs, Cochrane’s RoB-2 tool was used. For every other study design, the appropriate Joanna Briggs Institute (JBI) critical appraisal tool was used.
Synthesis of Result
A meta-analysis was not performed due to significant clinical and methodological heterogeneity across studies, including variations in SCPB techniques, surgical procedures, outcome measures, and follow-up durations. Additionally, small sample sizes and limited RCTs precluded meaningful statistical pooling.
Results
Study Selection
This systematic review followed the PRISMA 2020 guidelines (Figure 1).
PRISMA 2020 flow diagram for study selectionPRISMA: Preferred Reporting Items for Systematic Reviews and Meta-Analyses
Study Characteristics
The characteristics of all the included studies with the above-mentioned data items have been combined in a table (Table 3).
Risk of Bias in Studies
The quality of the included studies was assessed individually by the reviewers by using the RoB-2 tool for RCTs (Figures 2, 3) and the JBI checklist for other study designs (Tables 4-6).
Summary of risk of bias for included randomized controlled trials (RoB-2)
Risk of bias summary graph showing percentage distribution of judgments across RoB-2 domains
Quality ranking was allocated as low (less than 33%), medium (33%-66%), or high (over 67%). Out of nine studies, three studies were of medium quality [1,6,11], while the other six studies were of high quality [3,5,7-10]. Due to the lack of data and heterogeneity of included studies, a meta-analysis could not be performed.
Outcome Assessment
Pain assessment utilized the VAS across multiple studies, including those by Patel et al. [7], Kumar et al. [1], and Singh et al. [6]. Intraoperative fentanyl requirements were specifically measured in Patel et al.'s study [7], while postoperative rescue analgesic requirements were also evaluated in the same study. Intraoperative and postoperative hemodynamic monitoring, including changes in pulse rate, SpO_2_, and ECG parameters, was consistently assessed by Patel et al. [7], Kumar et al. [1], and Peksöz et al. [11]. Additional outcome parameters included the waiting period for initial analgesic demand and onset/duration of anesthesia, both measured in Kumar et al.'s study [1]. These varied assessment methodologies reflect the heterogeneity in outcome reporting across the included studies. It is further summarized in Table 7.
Discussion
This systematic review investigates the efficacy and safety of the SCPB as an alternative to GA in OMFS, specifically in procedures involving the mandibular and perimandibular regions. The increasing interest in regional anesthesia as a substitute for GA is driven by multiple factors: rising healthcare costs, the need for outpatient surgical options, and an aging population with significant comorbidities [15]. As such, this review addresses a clinically relevant question that has implications for patient safety, healthcare resource allocation, and the evolution of surgical anesthesia protocols in mandibular and perimandibular procedures.
The review included nine studies encompassing various research designs, including RCTs, prospective studies, case series, and case reports. Across the studies, 164 patients underwent mandibular and perimandibular surgical procedures using SCPB either as a sole anesthetic technique or in combination with local or regional nerve blocks. The most prominent finding was that SCPB consistently provided effective perioperative analgesia with minimal complications.
Studies that included direct comparison with GA or local infiltration, such as those by Patel et al. [7] and Kumar et al. [1], demonstrated statistically significant improvements in intraoperative and early postoperative pain control in the SCPB groups. In the RCT by Patel et al., postoperative analgesic requirements and VAS scores at six hours were significantly lower in the SCPB group compared to GA. These results are indicative of SCPB's role in enhancing immediate postoperative comfort, potentially reducing reliance on opioid analgesics.
Similarly, Kumar et al. [1] found that patients receiving SCPB had an extended duration before requesting postoperative analgesia, suggesting better pain modulation. These studies lend credibility to the assertion that SCPB may enhance patient outcomes without the hemodynamic instability often associated with GA.
Case series and prospective clinical trials without control groups, such as those by Singh et al. [6], Kanthan [3], and Zhao et al. [5], further support SCPB's utility. They report high success rates and patient satisfaction, particularly in minor to moderate OMFS procedures such as abscess drainage, soft tissue lesion excision, and even mandibular fracture fixation when used adjunctively with other local blocks. Importantly, these studies did not report any major complications like nerve injury, systemic toxicity, or need for urgent conversion to GA (except one patient in Singh et al.'s study who reported unbearable pain).
GA remains the gold standard for extensive OMFS procedures, particularly those requiring absolute immobility, prolonged duration, or complex airway management. However, GA is not without drawbacks: cardiopulmonary complications, prolonged recovery time, postoperative nausea and vomiting (PONV) [16,17], and increased demand for perioperative resources. In contrast, SCPB offers several advantages: it avoids airway manipulation, maintains patient consciousness, and facilitates early ambulation and discharge. These attributes are particularly beneficial in patients with comorbidities or in outpatient surgical settings.
Moreover, the use of SCPB aligns with the principles of Enhanced Recovery After Surgery (ERAS), which emphasizes multimodal, opioid-sparing analgesia, early mobility, and minimal invasiveness [18-20]. By maintaining stable intraoperative vitals and offering superior postoperative pain control, SCPB contributes directly to these goals. As observed in the reviewed studies, none of the patients required airway support or reported severe PONV, common issues in GA [21,22].
A critical dimension of evaluating any anesthetic technique is its safety profile. SCPB is relatively safe, especially when performed using ultrasound guidance. Across the nine studies included in this review, the incidence of adverse effects was negligible. No major complications-such as phrenic nerve palsy, intravascular injection, or systemic toxicity-were reported. Only one study (Patel et al. [7]) noted two instances of PONV in the GA group, while none were reported in the SCPB cohort.
The superficial nature of SCPB reduces the likelihood of complications seen in deep cervical plexus blocks, such as epidural or subarachnoid spread. The block’s anatomical target, superficial sensory branches of C2-C4, limits motor involvement and minimizes the risk of respiratory compromise. These features make SCPB especially appealing for elderly or high-risk patients who might not tolerate GA well [23-25].
Limitations
Despite the encouraging findings, this review also highlights significant methodological limitations in the current literature, including small sample sizes and heterogeneity in study design that limit the generalizability of results. Only two studies used randomized control designs with blinding protocols, while others were observational or case-based with potential for selection and observer bias. Many studies did not use standardized tools for pain assessment, making inter-study comparisons difficult-some reported VAS scores, others did not quantify analgesic efficacy or relied on subjective feedback, and the lack of long-term follow-up data precludes assessment of sustained analgesic efficacy and delayed complications. Variations in SCPB technique (such as landmark-based versus ultrasound-guided), dosage of local anesthetics, and adjunctive block usage also contributed to heterogeneity, underscoring the need for a standardized protocol and uniform outcome measures to enable high-quality meta-analyses in future research. To date, no ERAS pathways explicitly integrating SCPB for OMFS procedures and no dedicated systematic reviews or meta-analyses of SCPB in OMFS have been reported. As a result, we relied on individual clinical studies of SCPB in OMFS together with broader literature on cervical plexus blocks, GA risk, and ERAS principles to frame our interpretation of SCPB-related outcomes.
Conclusions
This systematic review affirms the efficacy and safety of the SCPB as a viable alternative to GA in selective oral and maxillofacial surgical procedures. SCPB provides comparable and, in many cases, superior intraoperative and immediate postoperative analgesia while maintaining a superior safety profile and patient satisfaction. Though more rigorous evidence is needed, current findings support broader incorporation of SCPB into anesthetic protocols, particularly in high-risk patients and resource-constrained environments. With standardization and further research, SCPB has the potential to become a cornerstone in regional anesthesia for OMFS.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1SCPNB is an adjuvant to local anaesthesia for maxillofacial surgical practice Bioinformation Kumar S Parashar P Mallick S Abhishek D L Mane S Girija A 6056101920233788616210.6026/97320630019605 PMC 10599667 · doi ↗ · pubmed ↗
- 2Cervical plexus block Korean J Anesthesiol Kim JS Ko JS Bang S Kim H Lee SY 2742887120182996989010.4097/kja.d.18.00143 PMC 6078883 · doi ↗ · pubmed ↗
- 3The use of superficial cervical plexus block in oral and maxillofacial surgical practice as an alternative to general anesthesia in selective cases Ann Maxillofac Surg Kanthan RK 48620162756359810.4103/2231-0746.186120 PMC 4979341 · doi ↗ · pubmed ↗
- 4Cervical plexus block Stat Pearls [Internet] Hipskind JE Hendrix JM Ahmed AA Treasure Island (FL)Stat Pearls Publishing 2025 https://www.ncbi.nlm.nih.gov/sites/books/NBK 557382/32491314 · pubmed ↗
- 5Combination of ultrasound guided superficial cervical plexus block and local infiltration for oromaxillofacial surgeries: a case series Front Oncol Zhao HR Hao JS Xue LF Zhao JZ Wang YC Xiao WL 14120621420243957542910.3389/fonc.2024.1412062 PMC 11578926 · doi ↗ · pubmed ↗
- 6Use of superficial cervical plexus block in submandibular and submental space abscess drainage Birat J Health Sci Singh V KCB Giri R Bhagat P 82683042020
- 7Evaluating the analgesic efficacy of superficial cervical plexus block for head and neck surgeries: a comparative randomized control study Cureus Patel H Shah N Syed A Shah P Macwan S 015202310.7759/cureus.39303 PMC 1028161337346207 · doi ↗ · pubmed ↗
- 8The safety and effectiveness of superficial cervical plexus block in oral and maxillofacial surgery as an alternative to general anesthesia in selective cases: a clinical study J Maxillofac Oral Surg Hakim TA Shah AA Teli Z Farooq S Kosar S Younis M 23291820193072868710.1007/s 12663-017-1029-4PMC 6328819 · doi ↗ · pubmed ↗