Impact of a Dedicated Trauma Consult Service on Burnout Among Physicians and Nurses: A Longitudinal Survey
Robert Green, Darby Green, Adam Harris, Breanne Gillis, Sarah Sturge, Daniel Cashen, Hillary Ferguson, Izabella Opra

TL;DR
A dedicated trauma consult service reduced burnout among trauma care physicians and nurses over one year in Nova Scotia.
Contribution
This study demonstrates that introducing a dedicated trauma consult service can reduce clinician burnout in trauma care.
Findings
Burnout symptoms decreased at one year after implementing the Trauma Consult Service.
Staff engagement increased across all Utrecht Work Engagement Scale measures.
Few participants used mental health resources despite reduced burnout.
Abstract
Background Trauma and emergency medicine providers have previously reported high levels of burnout, which were exacerbated by the COVID pandemic. This study evaluated the impact of trauma system change with the introduction of a novel Trauma Consult Service (TCS) on clinician burnout levels at zero, six, and 12 months for major trauma patients in Nova Scotia. Methods A longitudinal electronic survey was developed and piloted by the research team. Baseline surveys were administered in November 2022 to clinicians who pivoted from their usual career to a dedicated focus on inpatient trauma care. Demographic data and burnout symptoms were assessed using surveys, i.e., the Copenhagen Burnout Inventory, the Maslach Burnout Inventory, and the Utrecht Work Engagement Scale. Follow-up surveys were conducted at six and 12 months. Generalized estimating equations (GEE) were fitted to determine…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
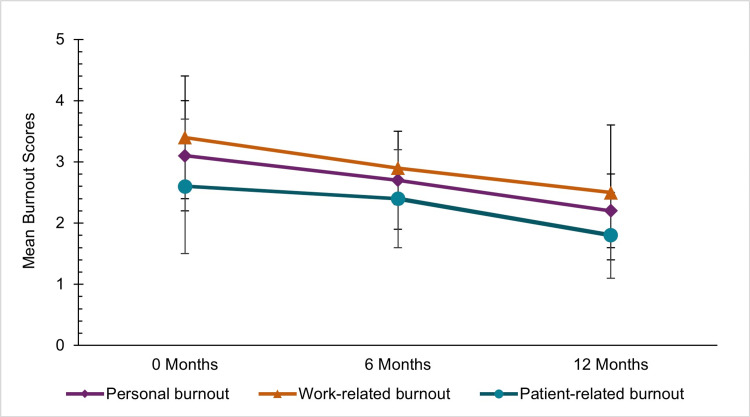 Figure 1
Figure 1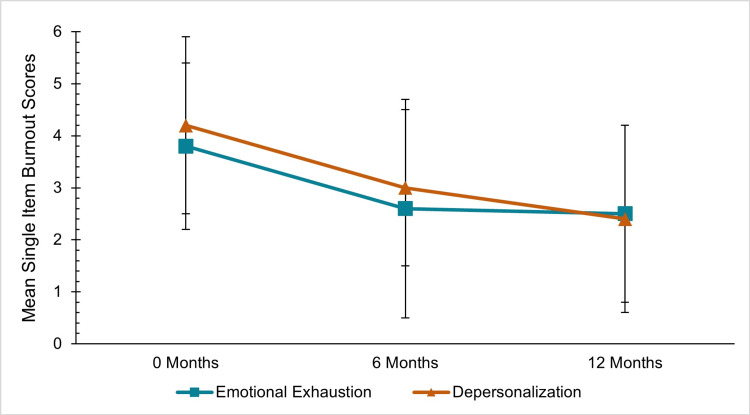 Figure 2
Figure 2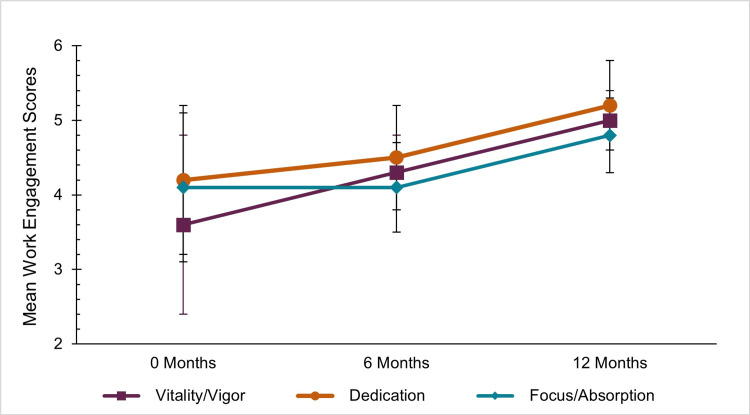 Figure 3
Figure 3| Characteristics | Overall (n=29) | 0 months (n=13) | 6 months (n=8) | 12 months (n=8) | |
| Age group in years, n (%) | 31-40 years | 14 (48.3) | 6 (46.1) | n<5 | n<5 |
| 41-50 years | 8 (27.6) | n<5 | n<5 | n<5 | |
| >50 years | 7 (24.1) | n<5 | n<5 | n<5 | |
| Sex, n (%) | Male | 27 (93.1) | 12 (92.3) | 8 (100.0) | 7 (87.5) |
| Female | n<5 | n<5 | 0 (0) | n<5 | |
| Position, n (%) | Trauma Team Leader/Trauma Consult Physician | 13 (44.8) | 5 (38.4) | n<5 | n<5 |
| Trauma Team Leader | 9 (31.0) | n<5 | n<5 | n<5 | |
| Trauma Consult Nurse | 7 (24.1) | n<5 | n<5 | n<5 | |
| Work status, n (%) | Full-time | 28 (96.6) | 13 (0.0) | 7 (87.5) | 8 (100.0) |
| Part-time | n<5 | 0 (0) | n<5 | 0 (0) | |
| Years providing trauma care, n (%) | <1-5 years | 6 (20.7) | n<5 | n<5 | n<5 |
| 6-10 years | 17 (58.6) | 7 (53.8) | n>5 | n<5 | |
| >10 years | 6 (20.7) | n<5 | n<5 | n<5 | |
| Percent of work time involving trauma care, n (%) | 0%-20% | 13 (44.8) | 6 (46.2) | n<5 | n<5 |
| 21%-40% | 6 (20.7) | n<5 | n<5 | n<5 | |
| 41%-60% | 6 (20.7) | n<5 | n<5 | n<5 | |
| 61%-80% | 2 (6.9) | 0 (0) | n<5 | n<5 | |
| 81%-100% | 2 (6.9) | 0 (0) | n<5 | n<5 | |
| Have children living at home, n (%) | 18 (62.1) | 7 (53.8) | 6 (75.0) | 5 (62.5) | |
| Had COVID in the past year, n (%) | 15 (51.7) | 10 (76.9) | n<5 | n<5 | |
| Missed work due to COVID, n (%) | 17 (58.6) | 11 (84.6) | n<5 | n<5 | |
| Approach to work was dramatically impacted by COVID, n (%) | 13 (44.8) | 8 (61.5) | n<5 | n<5 | |
| Total COVID impact, n (%) | 45 (51.7) | 29 (64.4) | 10 (22.2) | 6 (13.3) | |
| Recipient of physical abuse, n (%) | 8 (27.6) | 5 (38.5) | n<5 | n<5 | |
| Recipient of bullying, n (%) | 10 (34.5) | 5 (38.5) | n<5 | n<5 | |
| Recipient of verbal abuse, n (%) | 20 (69.0) | 10 (76.9) | 5 (62.5) | 5 (62.5) | |
| Recipient of a lack of care, n (%) | 13 (44.8) | 7 (53.8) | n<5 | n<5 | |
| Recipient of a lack of respect, n (%) | 21 (72.4) | 9 (69.2) | 6 (75.0) | 6 (75.0) | |
| Recipient of a lack of trust, n (%) | 15 (51.7) | 5 (38.5) | 5 (62.5) | 5 (62.5) | |
| Total negative experiences reported, n (%) | 79 (45.4) | 36 (45.6) | 24 (30.4) | 19 (24.1) | |
| Used mental health resources to improve well-being, n (%) | n<5 | n<5 | 0 (0) | 0 (0) | |
| Assessment tool | 0 months (n=13) | 6 months (n=8) | 12 months (n=8) | OR | 95% CI | P value | Cronbach's alpha | |
| Copenhagen Burnout Inventory | Personal burnout | 3.1±0.9 | 2.7±0.8 | 2.2±0.6 | 0.93 | 0.89-0.97 | <0.001 | 0.91 |
| Work-related burnout | 3.4±1.0 | 2.9±0.6 | 2.5±1.1 | 0.93 | 0.87-0.99 | 0.016 | 0.94 | |
| Patient-related burnout | 2.6±1.1 | 2.4±0.8 | 1.8±0.7 | 0.94 | 0.88-1.00 | 0.07 | 0.927 | |
| Overall score | 3.3±0.9 | 2.7±0.7 | 2.2±0.6 | 0.93 | 0.88-0.98 | 0.012 | 0.968 | |
| Maslach Burnout Inventory single-item measures | Emotional exhaustion | 3.8±1.6 | 2.6±2.1 | 2.5±1.7 | 0.88 | 0.79-0.98 | 0.023 | - |
| Depersonalization | 4.2±1.7 | 3.0±1.5 | 2.4±1.8 | 0.86 | 0.76-0.98 | 0.023 | - | |
| Utrecht Work Engagement Scale | Vitality/vigor | 3.6±1.2 | 4.3±0.5 | 5.0±0.4 | 1.12 | 1.06-1.19 | <0.001 | 0.9 |
| Dedication | 4.2±1.0 | 4.5±0.7 | 5.2±0.6 | 1.08 | 1.02-1.14 | 0.005 | 0.866 | |
| Focus/absorption | 4.1±1.0 | 4.1±0.6 | 4.8±0.5 | 1.06 | 1.01-1.11 | 0.019 | 0.721 | |
| Overall score | 3.9±1.0 | 4.3±0.6 | 5.0±0.4 | 1.09 | 1.03-1.14 | 0.001 | 0.937 | |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHealthcare professionals’ stress and burnout · COVID-19 and Mental Health · Posttraumatic Stress Disorder Research
Introduction
Burnout is a syndrome that has been recognized as an acute and chronic occupational stress response in medical providers, particularly in high-pressure specialties, including emergency medicine and trauma. Although burnout may manifest in various ways, it is most often characterized as a stress response that includes three components: emotional exhaustion, depersonalization, and a sense of reduced personal accomplishment [1]. Recent investigations have highlighted that the burdens of limited staffing and high turnover rates may result in moral distress and shorten career duration [2,3]. The demanding nature of the emergency medicine environment, characterized by extended work hours, administrative burdens, and an unpredictable, emotionally intense pace of patient care, increases the risk of burnout among physicians and other clinicians [4,5]. The prevalence of burnout increased among physicians and allied healthcare providers during the COVID pandemic, adding additional strain to an overburdened healthcare system [6,7]. Many clinicians experienced the very real costs of burnout (e.g., anxiety, addiction, attrition, or thoughts of suicide), which negatively affected patient care and challenged the healthcare system across Canada [8].
As part of the Nova Scotia Provincial Trauma Program, the launch of a novel inpatient Trauma Consult Service (TCS) in 2022 offered a unique opportunity to investigate the impact on physician and nurse burnout. The TCS, comprising Trauma Team Leaders from emergency medicine, critical care, and anesthesia staff, collaborates with a trauma resource nurse (RN) to provide comprehensive care for trauma inpatients throughout the duration of their hospital stay, from the time of trauma team resuscitation to patient discharge. The TCS delivers comprehensive education to inpatient and outpatient units, ensuring the continuity of care for trauma patients.
We hypothesized that clinicians who were allowed to modify part of their clinical focus from their base specialty (i.e., emergency medicine, anesthesia, and critical care) to include dedicated weeks of service within the novel TCS would experience a decrease in burnout symptoms. We investigated burnout rates among Trauma Team Leaders and TCS members at zero months (baseline), six months, and 12 months following the implementation of the service to determine whether well-being and symptoms of burnout would improve over time. Investigations that focus on the impact of occupational stress (such as burnout syndrome) are necessary to determine future interventions aimed at supporting healthy physicians and nurses in emergency medicine, trauma, and other high-stress medical specialties.
This article was previously presented as a poster at the 2024 London Trauma Conference, in London, England, from December 3rd to 6th 2024, and at the 2025 Trauma Association of Canada Annual Scientific Meeting and Congress in Gatineau, Quebec, from March 19th to 21st 2025.
Materials and methods
Study setting
The Canadian province of Nova Scotia has an inclusive trauma system where patients receive care from a dedicated trauma team and have early access to specialty consultation. In Nova Scotia, there are two level 1 trauma centers (one adult and one pediatric) and eight regional level 3 trauma centers throughout the province. All patients with major trauma are transported to the level 1 trauma center in the Queen Elizabeth II Health Sciences Centre (QEII) in Halifax, Nova Scotia.
Survey design
The study was approved by the Nova Scotia Health Research Ethics Board (approval number: 1028409). We developed and tested an electronic survey using SelectSurvey version 5.0 (ClassApps, Apollo Beach, FL) (see Appendices). This is an exploratory survey that used three different assessment tools to measure burnout. The survey was administered via email at three different data collection points: zero months (November 2022), six months (May 2023), and 12 months (November 2023). Subsequently, one reminder email was distributed within 10 days after each time point. The study was conducted in accordance with the CROSS checklist for reporting survey research [9].
Outcome measures
Data collected included demographics and burnout symptoms. Demographic questions included work experience and employment type. The participants were asked multiple questions about work-related impacts, such as negative behaviors they had experienced or witnessed while working with the Trauma Consult Service (TCS), and whether they used wellness resources.
We evaluated burnout symptoms using three previously validated scoring systems: the Copenhagen Burnout Inventory, the Maslach Burnout Inventory single-item scales, and the Utrecht Work Engagement Scale. The Copenhagen Burnout Inventory measures personal, work-related, and patient-related burnout using a 19-item survey [10]. Multiple questions were included for each of the subscales (personal, work-related, and patient-related burnout). Responses were on five-point scales, by either frequency (e.g., "never" to "always") or intensity (e.g., "to a very low degree" to "to a very high degree"), and were coded into scores of "one, two, three, four, and five" for modelling. Scores of less than two indicate low levels of burnout, and scores greater than or equal to three indicate a high degree of burnout.
The Maslach Burnout Inventory measures work-related burnout on two single-item subscales: emotional exhaustion and depersonalization [11,12]. This inventory was used with licensed permission. For this study, only emotional exhaustion and depersonalization were assessed. Each subscale includes a seven-point Likert-type frequency response scale (zero, never; one, a few times a year or less; two, once a month or less; three, a few times a month; four, once a week; five, a few times a week; and six, every day). Scales are scored such that higher scores indicate more of each construct. Scores of 4 or higher on the emotional exhaustion and depersonalization subscales indicate a greater burden of burnout symptoms.
We assessed the work engagement of survey respondents using the Utrecht Work Engagement Scale, which consists of 17 items across three dimensions (dimension one, vitality; dimension two, dedication; and dimension three, focus), with higher scores (greater than or equal to 4) indicating higher levels of work engagement [13].
Participants
The participants were recruited using convenience sampling among trauma clinicians at the QEII in Halifax, Nova Scotia. The survey was administered to all Trauma Team Leaders (n=19, including seven who are also Trauma Consult Physicians) and Trauma Consult Nurses (n=5) at a level 1 trauma center. Therefore, the maximum possible number of participants was 24, and the maximum possible number of responses across all three points was 72. The trauma center and TCS employ a mixed-model care approach, in which both the Trauma Team Leader and the Trauma Consult Physician may be surgeons or non-surgeons.
Statistical analysis
Patient demographics and characteristics were reported with descriptive statistics. To maintain privacy, cell sizes less than five are reported as "n<5," with adjacent cells reported as "n>5." Generalized estimating equations (GEE) were fitted to determine the effect of implementing the TCS on burnout symptoms. Generalized estimating equations (GEE) are a statistical method for analyzing correlated data, such as repeated measurements on the same subjects across measurement occasions. Generalized estimating equations account for this correlation, providing more accurate estimates of relationships between variables. We used generalized estimating equations to compare mean scores on each burnout scale.
A sensitivity analysis was conducted because only 10 participants responded to the survey at two or more time points (<5 responded at all three time points), yielding both paired and unpaired data. All survey responses were included in the analysis, as excluding participants with missing data may introduce potential selection bias. The sensitivity analysis consisted of a GEE model with independence correction and two linear models: a pooled and a mixed-effects model.
Results
There were 16 participants out of a possible 24 (66.7% participation rate). Of the participants, 62.5% (10/16) responded at multiple time points (<5 responded at all three time points), yielding a cumulative response rate of 40.3% (29/72) across all three time points. At each time point, the response rates were as follows: 54.2% (13/24) at zero months, 33.3% (8/24) at six months, and 33.3% (8/24) at 12 months. Table 1 shows that the majority of responses across all three time points came from Trauma Team Leaders/Trauma Consult Physicians (n=13), followed by Trauma Team Leaders (n=9) and Trauma Consult Nurses (n=7). This is equivalent to a cumulative response rate of 38.6% (22/57) among physicians and 46.6% (7/15) among nurses. Nearly all were full-time employees (96.6%), and most had 6-10 years of experience providing trauma care (58.6%). The majority of the participants at zero months reported that COVID impacted their work at the initiation of the Trauma Consult Service (TCS) (64.6%), but this decreased to 13.3% at 12 months. Table 1 illustrates the self-reported impacts of work. Few participants reported using mental health resources to improve their well-being (3.4%).
The GEE models for the Copenhagen Burnout Inventory, Maslach Burnout Inventory, and Utrecht Work Engagement Scales are summarized in Table 2. The sensitivity analysis shows consistency when the data are modelled under different assumptions (see Appendices). Trauma clinicians reported a decrease in burnout levels and an increase in engagement levels at the one-year follow-up. Generalized estimating equations demonstrate that overall, there was a downward trend in burnout symptoms and an increase in work engagement.
There were reductions in burnout demonstrated in the Copenhagen Burnout Inventory scores between zero and 12 months (odds ratio {OR}, 0.93; 95% confidence interval {CI}, 0.88-0.99) (Figure 1). Both personal (3.1±0.9) and work-related (3.4±1.0) burnout at zero months are both scores over 3, indicating high burnout. All Copenhagen Burnout Inventory measures at 12 months decreased to less than three, indicating low to intermediate burnout (overall=2.2±0.6). Notably, the decrease in personal burnout (OR, 0.93; 95% CI, 0.89-0.97) was significant (p-value<0.001). There were also significant decreases in work-related (OR, 0.93; 95% CI, 0.87-0.99) and patient-related (OR, 0.94; 95% CI, 0.87-1.99) burnout. The internal consistency of the Copenhagen Burnout Inventory measures was high (overall Cronbach's α=0.968).
Burnout symptom scores measured by the Copenhagen Burnout Inventory at zero, six, and 12 months.The Copenhagen Burnout Inventory includes three subscales: personal burnout, work-related burnout, and patient-related burnout. Scores less than 2 indicate low levels of burnout, and scores greater than or equal to 3 indicate a high degree of burnout.
For the Maslach Burnout Inventory, each of the single-item measures showed decreases in emotional exhaustion and depersonalization symptoms (Figure 2). At zero months, emotional exhaustion scores (3.8±1.6) decreased at 12 months (2.5±1.7). Similarly, for depersonalization, the score at zero months (4.2±1.7) decreased to 12 months (2.4±1.8). For emotional exhaustion (OR, 0.88; 95% CI, 0.79-0.98) and depersonalization (OR, 0.86; 95% CI, 0.76-0.98), the generalized estimating equations both showed a significant decrease from zero to 12 months, with p-values of 0.023.
Maslach Burnout Inventory single-item scale scores for emotional exhaustion and depersonalization at zero, six and 12 months.Scores greater than or equal to 4 indicate a greater burden of burnout symptoms.
There was also increased staff engagement across all three Utrecht Work Engagement Scales (overall score: OR, 1.09; 95% CI, 1.03-1.14) (Figure 3). Specifically, the vigor scores increased from zero months (3.6±1.2) to 12 months (5.0±0.4), which showed a significant effect with a p-value of <0.001 (OR, 1.12; 95% CI, 1.06-1.19). Additionally, we noted substantial increases in dedication (OR, 1.08; 95% CI, 1.02-1.14) and focus/absorption (OR, 1.06, 95%CI 1.01-1.11). The Utrecht Work Engagement Scales measured high internal consistency (overall Cronbach's α: 0.937).
Utrecht Work Engagement Scale scores at zero, six, and 12 months.The Utrecht Work Engagement Scale includes three subscales: vigor, dedication, and focus/absorption. Scores greater than or equal to 4 indicate higher levels of work engagement.
Discussion
Statement of principal findings
Our study found an association of reduced burnout symptoms (as measured by the Copenhagen Burnout Inventory, the Maslach Burnout Inventory, and the Utrecht Work Engagement Scale) among clinicians who worked for the novel Trauma Consult Service (TCS) over 12 months. The Copenhagen Burnout Inventory indicated reductions in both personal and work-related burnout. At the same time, the Maslach Burnout Inventory demonstrated reductions in emotional exhaustion and depersonalization, and the Utrecht Work Engagement Scale revealed increased work engagement. Clinicians (physicians and nurses) who initiated a change in their clinical focus (in part or in total) to include the resuscitation and longitudinal care of major trauma patients all reported significant improvement in all burnout measures, consistent with improved clinician well-being. Our results suggest that systemic changes, such as the introduction of a novel TCS, can support career redefinition and are associated with an improvement in population-level clinician resilience and job satisfaction. Features of workplace happiness and engagement include clinicians who focus on novel, challenging, and personally meaningful work [14].
This study also found reductions in the impact COVID had on staff over the 12-month period. Therefore, the TCS shows promise in reducing burnout. However, the decrease in burnout systems could be attributed to other factors, such as the decreasing COVID burden. The evaluation of system performance demonstrated that the TCS improved patient, provider, and family satisfaction, which may be important variables contributing to the improvement in our physicians' and nurses' burnout symptoms [15]. The TCS has been recognized locally and nationally for its excellence in quality of care and patient experience, which underscores the importance of the TCS to trauma care in Nova Scotia and the Maritime region [16].
Interpretation within the context of the wider literature
Similar studies conducted internationally and in Canada have not found a link between burnout and the establishment of an inpatient TCS [6,8]. A Canadian survey of emergency medicine burnout during the early COVID pandemic found that team support and access to resources were key in reducing burnout [7]. This phenomenon has also been observed in the United States and Europe, both before and during the COVID pandemic [17,18]. Organizational changes that reduce clinical burden while maximizing efficiency are viable options for reducing burnout [19,20]. Investigators recommend engaging providers before implementing organizational changes to allow them to bring forward suggestions that apply to the local setting [21]. In these cases, changes introduced have limited the unpredictability of clinical workload and patient acuity, ultimately reducing burnout [22]. Alternatively, moving from 24-hour call to 12-hour blocks improved burnout among staff without compromising clinical productivity [23].
Our study focused on a partial career shift as the intervention itself. In contrast, other studies have explored wellness interventions, such as mindfulness-based programs and those improving communication and physician well-being [24]. Wellness leadership interventions have been shown to decrease burnout symptoms, as demonstrated in a six-week program in the provincial health system in Nova Scotia [2]. Other wellness interventions that may be effective in decreasing burnout symptoms include regular physical activity, healthy dietary habits, social engagement, mentorship programs, and regular health checkups [25].
Interventions to reduce burnout symptoms have demonstrated some effectiveness, including adjustments to job demands, changes in work structure, and physical activity initiatives [23,26]. Our investigation suggests that organizational changes may impact burnout symptoms, especially when clinicians find renewed purpose and satisfaction in their work. In this study, a system-level change was introduced (i.e., the new TCS), which enabled trauma clinicians to refocus their clinical work, transitioning in part from their base specialty to trauma resuscitation combined with inpatient consulting. This change resulted in a positive impact on their burnout levels within 12 months. As healthcare systems evolve to support optimal patient care, prioritizing clinician well-being through such role shifts when viable is essential to optimize both patient care and career satisfaction. However, the specific reasons for this reduction remain unclear. Improvement in burnout may have been due to a combination of role changes, team dynamics, or other factors. Clinicians in this study experienced new roles and/or career change, and it should be explored whether these changes are transferable to other trauma centers and clinicians.
Strengths and limitations
This study has several strengths. First, it offers a longitudinal analysis of burnout symptoms over a 12-month period, which allows insight into the impact of the TCS. The use of multiple validated burnout and engagement measures enhances the robustness of our findings, which can be compared to a wide range of studies that used the same measures [10,11,13]. Additionally, the diverse sample of Trauma Team Leaders and Nurses from different disciplines added to the generalizability of the results within similar high-stress healthcare settings.
Limitations to consider include a limited sample size due to the select group of clinicians involved with the TCS. While the cumulative response rate for all possible respondents across all time points was 40%, only eight respondents were included in six months and eight in 12 months. Only 10 participants responded to the survey at two or more time points, with <5 responding at all three time points. While only 24.1% (7/29) of responses were from nurses, 20% of the trauma staff are nurses, making the response rate proportional. We also relied on self-reported measures, which may be susceptible to response and recall biases. As the number of responses decreased for the subsequent time points (six and 12 months), there could also be bias, as clinicians with less burnout were more likely to respond to the survey. We reported burnout levels at all time points, and the sensitivity analysis attests to the downward trend in burnout symptoms. However, the low response rate and incomplete follow-up at six and 12 months mean that the results reflect a population-level trend rather than a within-subject change. Further investigations are needed to affirm that the TCS did reduce burnout symptoms.
We did not explicitly ask our clinicians to explain why they believed they had burnout symptoms, which would be of interest in a future investigation. Multiple factors may have contributed to the clinician's burnout, including the fact that the TCS was initiated during the COVID pandemic, which likely had a significant impact. This makes COVID likely a confounding variable in the study. The study asked about COVID, including whether it had affected their work, and found a decrease in the percentage of respondents who answered yes compared to 12 months earlier. Because there was no control group, a comparison of burnout symptoms among different clinician groups was not evaluated. This addition in future studies could help determine if reductions were attributable to the TSC or other confounding factors, such as COVID. We also received the highest number of responses from Trauma Team Leaders/Trauma Consult Physicians, who would have been the ones to choose to change their practice to include inpatient care. This may have increased the chances of the burnout symptoms decreasing, because they actively decided to change their practice. Although we believe that the TCS contributed to the reported improvement in burnout scores, it is possible that the lessening impact of COVID or other factors could be cofounding variables.
Implications for policy, practice, and research
The reduction in burnout symptoms among TCS clinicians is promising, but long-term sustainability remains uncertain. Investigating burnout symptoms at the initiation of the TCS was essential for understanding its impact. Other studies found that burnout levels increased post-pandemic, therefore requiring ongoing assessments to determine whether our TCS can sustain its positive impact on burnout symptoms. Follow-up studies that address the limitations of a low response rate, COVID's impact, and the lack of a control group would be beneficial for continued evaluations. Continued evaluation is crucial to ensure that clinicians receive adequate support and to explore how systemic changes can have a lasting time-related association with clinician well-being. Additionally, investigating barriers to mental health resource utilization and implementing targeted interventions may lead to improved long-term outcomes. For example, mindfulness-based interventions have shown modest but sustained reductions in burnout [27]. In contrast, other researchers have focused on the qualitative features of addressing burnout, such as fostering healthy team environments, addressing toxic collegial behaviors, and helping staff process the emotions associated with being exposed to intense situations [14]. Further studies should explore the impact of the TCS on patient outcomes, as organizational strategies, such as those summarized by Zhang et al. (2022), suggest that bundled interventions may be most effective [28].
Conclusions
Over 12 months, the implementation of a dedicated inpatient TCS was associated with a reduction in burnout symptoms and increased engagement among trauma clinicians. Further investigation is warranted to confirm whether these findings are attributable to a change in practice rather than to other factors, such as the COVID pandemic. The critical need to address burnout among emergency medicine staff globally cannot be overstated, as improving clinician well-being ultimately improves care and the functioning of healthcare systems as a whole.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Staff burn-out J Soc Issues Freudenberger HJ 159165301974
- 2Impact of a wellness leadership intervention on the empathy, burnout, and resting heart rate of medical faculty Mayo Clin Proc Innov Qual Outcomes Gilin DA Anderson GG Etezad S Lee-Baggley D Cooper AM Preston RJ 545555720233807542910.1016/j.mayocpiqo.2023.09.005PMC 10708962 · doi ↗ · pubmed ↗
- 3Examining the empathy profiles and work outcomes of trauma workers J Career Assess Anderson GG Gilin DA 739759332024
- 4A longitudinal survey on Canadian emergency physician burnout Ann Emerg Med de Wit K Tran A Clayton N 5765848320243832395110.1016/j.annemergmed.2024.01.009 · doi ↗ · pubmed ↗
- 5Impact of burnout on self-reported patient care among emergency physicians West J Emerg Med Lu DW Dresden S Mc Closkey C Branzetti J Gisondi MA 99610011620152675964310.5811/westjem.2015.9.27945 PMC 4703144 · doi ↗ · pubmed ↗
- 6Impact of the COVID-19 pandemic upon self-reported physician burnout in Ontario, Canada: evidence from a repeated cross-sectional survey BMJ Open Gajjar J Pullen N Li Y Weir S Wright JG 012202210.1136/bmjopen-2021-060138 PMC 949030036130759 · doi ↗ · pubmed ↗
- 7Canadian emergency physician psychological distress and burnout during the first 10 weeks of COVID-19: a mixed-methods study J Am Coll Emerg Physicians Open de Wit K Mercuri M Wallner C 10301038120203290502510.1002/emp 2.12225 PMC 7461319 · doi ↗ · pubmed ↗
- 8Canadian emergency medicine physician burnout: a survey of Canadian emergency physicians during the second wave of the COVID-19 pandemic CJEM Mercuri M Clayton N Archambault P 2882922420223508471010.1007/s 43678-021-00259-9PMC 8792132 · doi ↗ · pubmed ↗