Pediatric fractures in northern China: hospital-based epidemiology and high-risk factors from a regional cohort study
Fei-hu Li, Bin Dong, Chen-jing Li, Bin-bin Xing

TL;DR
This study examines pediatric fractures in northern China, identifying risk factors like age, sex, and season to guide prevention strategies.
Contribution
The study provides region-specific insights into pediatric fracture epidemiology and high-risk factors in northern China.
Findings
Males had a significantly higher fracture rate than females, especially during adolescence.
Summer had the highest fracture burden, while winter had the lowest.
Falls were the leading cause of fractures, followed by traffic accidents and bicycle-related injuries.
Abstract
To identify high-risk factors for pediatric fractures in a hospital-based regional cohort. We conducted a retrospective hospital-based cohort study including children ≤15 years treated for fractures at Yuncheng Central Hospital, Shanxi Province, between September 2021 and August 2024. Demographic (age, sex, BMI z-score, residence), injury-related (mechanism, time, season), and fracture characteristics were collected. Case identification and reporting were conducted in accordance with STROBE guidelines. Multivariable logistic regression models were prespecified to estimate adjusted odds ratios (aORs) with 95% confidence intervals (CIs), alongside descriptive statistics. Among 1,664 cases, males accounted for a significantly higher proportion than females (male:female ratio 1.70:1; 95% CI: 1.54–1.88), with disparity increasing in adolescence. Adolescents (11–15 years) were more…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
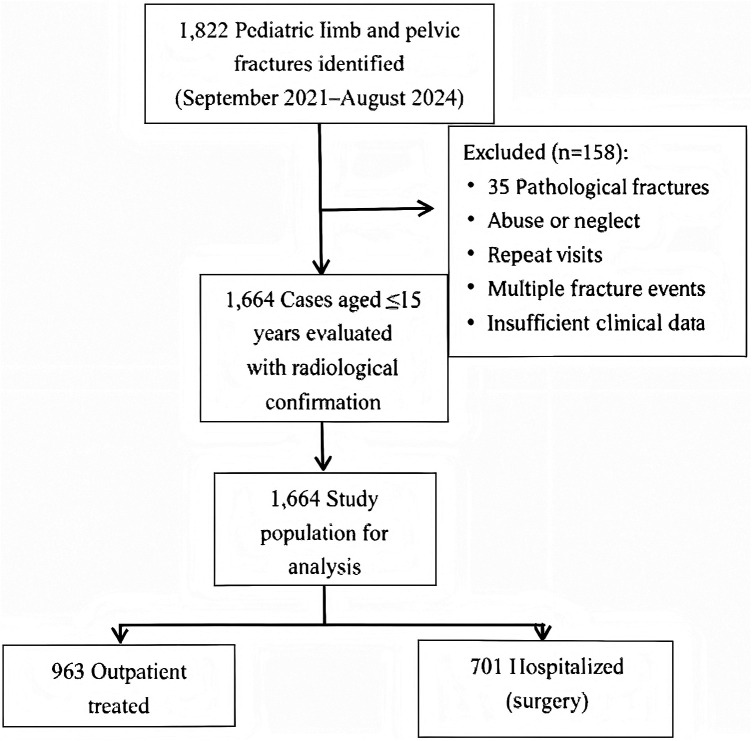 Figure 1
Figure 1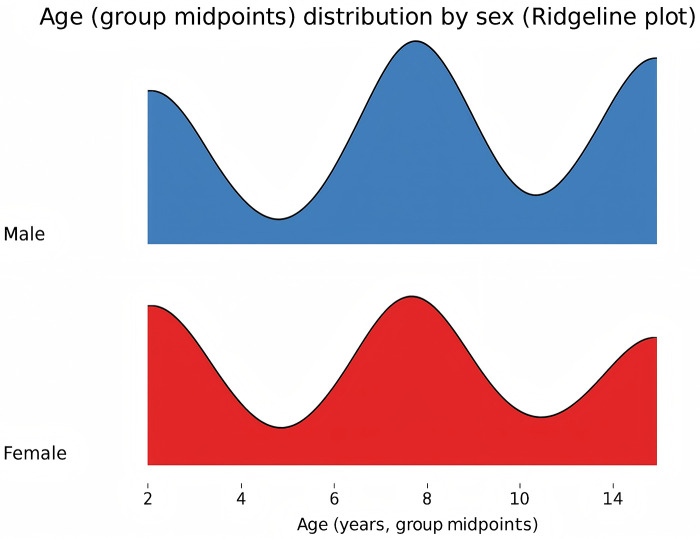 Figure 2
Figure 2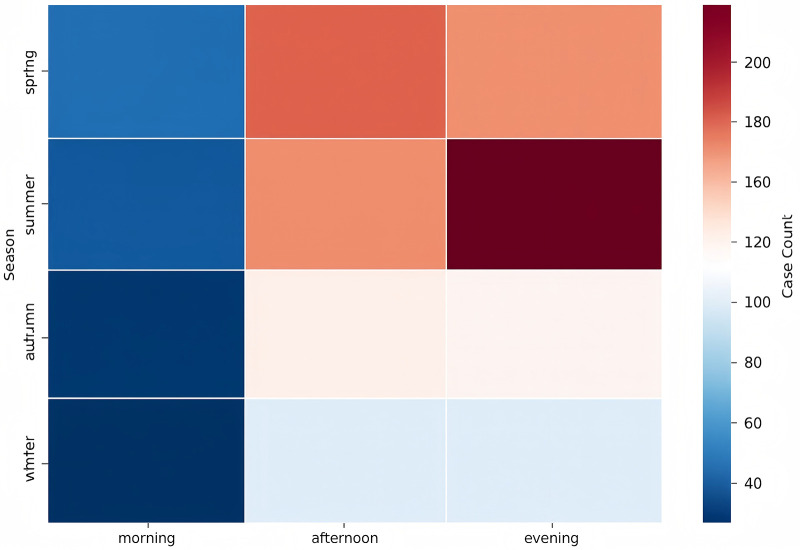 Figure 3
Figure 3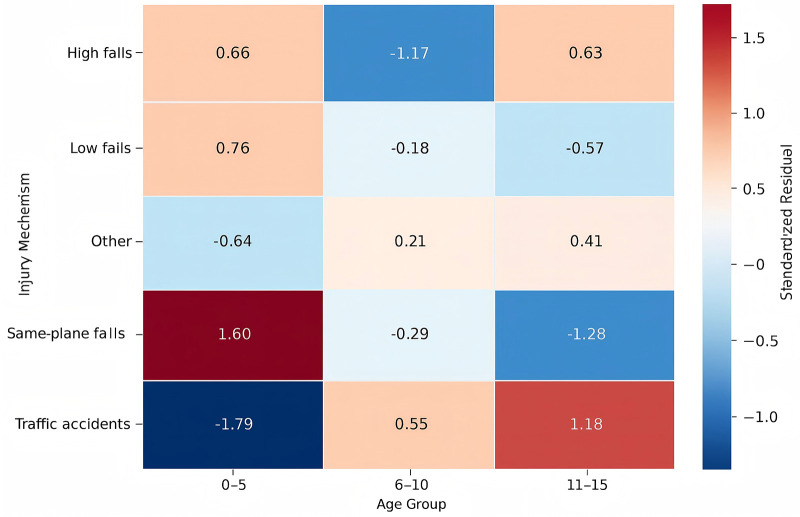 Figure 4
Figure 4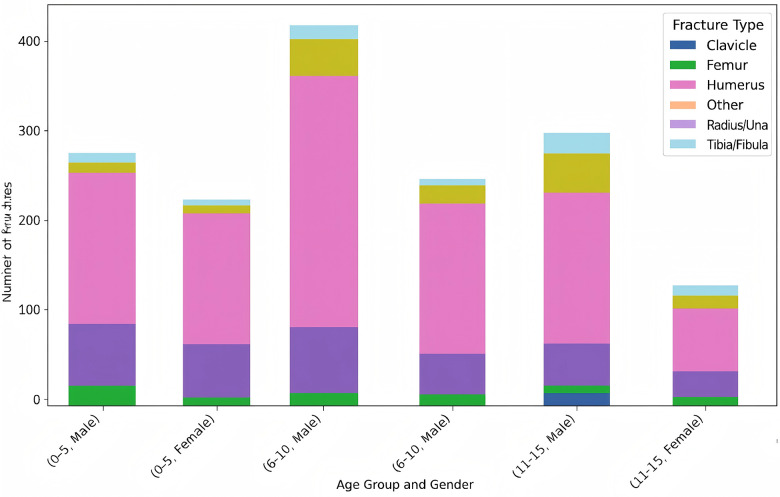 Figure 5
Figure 5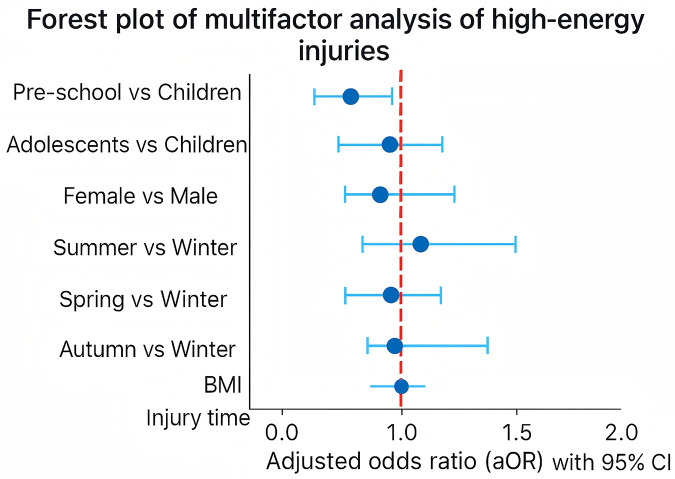 Figure 6
Figure 6| Characteristic | Outpatient ( | Inpatient ( | |
|---|---|---|---|
| Age group (0–5/6–10/11–15 yrs) | 32.1/ 45.3/ 22.6% | 31.1/37.4/ 31.5% | <0.001 |
| Sex (Male %) | 62.1% | 64.1% | 0.42 (NS) |
| BMI ≥25 (%) | NA | 6.5% | NA |
| Residence (Urban %) | NA | 46.5% | NA |
| Time of occurrence (Day vs. Night) | 45.3% vs. 54.7% | 53.6% vs. 46.4% | <0.01 |
| Season (Summer vs. Winter) | 35.4% vs. 17.5% | 33.5% vs. 15.2% | 0.12 (NS) |
| Injury mechanism (Falls/Traffic/Bicycle/Other) | NA | 68.2%/15.4%/8.6%/7.8% | NA |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsInjury Epidemiology and Prevention · Bone fractures and treatments · Bone health and osteoporosis research
Introduction
Pediatric fractures remain a frequent reason for clinical visits and are largely the result of accidental injuries. As congenital and disease-related causes of injury have declined with improvements in healthcare and nutrition, unintentional trauma has become a major contributor to morbidity in children (1). Previous epidemiological reports suggest that roughly one quarter of children experience some form of traumatic injury each year, and fractures account for a substantial proportion of these events (2). Seasonal and regional differences in fracture occurrence have been described (3–5), yet how these injuries present across different hospital settings has not been fully characterized.
Climatic conditions and children's daily activity patterns have been linked to variations in fracture incidence in many settings (6–8). For instance, distal radius fractures often peak during winter, although colder regions may paradoxically report fewer cases during the same season compared with temperate areas (9). Despite these observations, detailed cohort studies from single, high-volume regional centers are still limited. Such data are valuable because hospitals in different regions may receive distinct types of cases, influenced by local healthcare access, parental decision-making, and children's living and play environments. These factors can create regional differences not only in overall fracture incidence but also in the types of cases that present to hospitals, which has implications for prevention planning and resource allocation.
This study was carried out in a northern Chinese city (35°N, population approximately five million) with a typical monsoon climate and a single pediatric orthopedic referral center, allowing for comprehensive capture of local fracture cases. Because many continental and temperate regions share similar seasonal patterns, the observations from this setting may also be informative for comparable areas. Over a three-year period, we reviewed pediatric fracture cases to describe demographic patterns, seasonal and temporal trends, injury mechanisms, and fracture characteristics. We also examined how environmental and behavioral factors may contribute to injury risk. Based on prior evidence, we anticipated that sex, age group, season, and time of day would be associated with fracture occurrence. These findings may help guide local prevention efforts and contribute to future regional planning.
Methods
Study population
This study was carried out in Yuncheng, a northern Chinese city with a population of about five million. We included children aged 15 years or younger who were treated for extremity or pelvic fractures at the city's only pediatric orthopedic center between September 2021 and August 2024. All fractures were verified through imaging, including X-ray, CT, or MRI. We excluded cases involving spinal or pathological fractures, suspected abuse, duplicate entries, and repeated fracture events in the same patient. The case selection process is summarized in Figure 1.
Pediatric fracture cohort selection flowchart.
Study design & data collection
We collected information on a range of demographic, clinical, and injury-related variables to describe fracture patterns and explore potential risk factors. Key variables included:
- Demographics: sex, age group (0–5, 6–10, 11–15 years), BMI (WHO z-scores), residence (urban/rural)
- Injury Mechanisms: classified via ICD-10 codes (V01–Y99) (10), including traffic accidents, falls, mechanical injuries, blunt trauma, bicycle-related injuries, and others.
- Temporal Distribution: season (spring, summer, autumn, winter), time of injury (daytime: 07:00–18:00, including morning and afternoon; nighttime: 18:00–07:00)
- Clinical Characteristics: fracture site (e.g., humerus, radius/ulna, femur, tibia/fibula, pelvis) and type (e.g., greenstick, fissure, open/closed).
Data quality and statistical analysis
Data were extracted from the hospital information system and reviewed independently by two authors. Cases with unclear information were discussed with a senior investigator, and a random 10% sample was checked to maintain data accuracy. Missing values were handled using listwise deletion. High-energy trauma was defined as injuries caused by traffic or bicycle accidents, falls from height, skateboarding, or similar mechanisms. To examine factors associated with hospitalization and high-energy trauma, we used multivariable logistic regression. Adjusted odds ratios (aORs) and 95% confidence intervals (CIs) were calculated with Python (v3.14), and statistical significance was set at P < 0.05.
Ethical approval
The study was approved by the Institutional Review Board (YXLL-YJ2023017). Informed consent was obtained from the parents or legal guardians of all participants.
Results
General characteristics
Between September 2021 and August 2024, our hospital treated 1,664 children aged 15 years or younger for limb or pelvic fractures. Among them, 701 patients (42.1%) were admitted for surgical management, while the rest received outpatient care. Key demographic and clinical characteristics—including age, sex, BMI, residence, season, and treatment setting—are presented in Table 1.
Age and gender distribution
A total of 1,047 boys and 617 girls were included, giving a male-to-female ratio of 1.70 (95% CI: 1.54–1.88). The proportion of boys rose with age (χ^2^ = 47.59, P < 0.001) and reached 70.8% in the 11–15-year group (95% CI: 66.6–75.1; Figure 2). Among hospitalized patients, 322 (46.5%) lived in urban areas and 378 (54.0%) in rural areas. The relative proportion of urban to rural cases was slightly lower (RR = 0.85, 95% CI: 0.73–0.99), suggesting broadly similar distributions.
Age and gender distribution chart.
Temporal and seasonal distribution
Seasonal variation was evident, with the highest number of fractures occurring in summer (34.5%) and the lowest in winter (16.5%; χ^2^ = 109.0, P < 0.001). Compared with summer, winter showed a markedly lower risk (RR = 0.48, 95% CI: 0.41–0.55). Injuries also varied by time of day: 57.9% occurred during daytime hours and 42.1% at night (RR = 1.37, 95% CI: 1.24–1.51; Figure 3).
Heatmap of fracture cases by season and time of day.
Injury mechanisms and fracture patterns
Ground-level falls were the main cause of injury in younger children, whereas adolescents experienced relatively more traffic- and bicycle- related trauma. Fracture patterns also differed by age: supracondylar humerus fractures were most common in preschoolers, clavicle and distal radius fractures were frequent in school- aged children, and forearm fractures were more typical among adolescents (Figures 4, 5).
Standardized residuals of injury mechanisms by age group.
Distribution of fracture types by age group and gender.
Multivariable analysis of high-energy trauma
High-energy trauma included injuries caused by traffic or bicycle accidents, falls from height, skateboarding, and similar mechanisms. In multivariable analysis, adolescents had higher odds of sustaining high-energy trauma (aOR = 1.79, 95% CI: 1.06–3.02), as did children injured at night (aOR = 1.45, 95% CI: 1.01–2.08). Compared with winter, both summer (aOR = 0.44, 95% CI: 0.26–0.75) and autumn (aOR = 0.51, 95% CI: 0.27–0.97) were associated with lower risk. Preschool children also showed reduced odds (aOR = 0.48, 95% CI: 0.30–0.78). No significant associations were observed for sex, elevated BMI, or spring season. Results are shown in Figure 6.
Forest plot of multivariable logistic regression analysis for risk factors of high-energy trauma among hospitalized pediatric fracture patients.
Discussion
In this cohort, notable differences in fracture patterns were observed across age and sex. Boys accounted for a larger proportion of cases, a trend also described in previous studies and often attributed to higher activity levels and greater exposure to risk during adolescence (11). The mechanisms of injury varied by developmental stage: younger children were mainly injured by ground-level falls, school-aged children experienced more object-related trauma, and adolescents were more frequently involved in traffic- or bicycle-related incidents. These observations point to the need for age-appropriate prevention efforts, such as closer supervision for preschoolers and strengthened traffic safety education for older children. Similar age-stratified patterns have been reported in other regions, including findings from Shenzhen, where fall-related injuries predominated in younger children and traffic- or sports-related trauma increased with age (12).
Clear seasonal differences were observed, with more fractures occurring during summer and fewer in winter. These fluctuations likely reflect changes in outdoor activity associated with weather conditions. Injuries were also more common in the afternoon and evening. Although this pattern may simply mirror higher activity levels later in the day, we cannot rule out the possibility that some families delay seeking care; our dataset did not include time-to-presentation information to explore this further (13). Similar seasonal and diurnal trends have been described in studies from Switzerland, Malawi, and other regions, suggesting that environmental exposure and daily activity routines play a consistent role in pediatric fracture risk (14–16).
The distribution of injury mechanisms in our cohort differed somewhat from reports in other regions. For example, the proportion of fall-related fractures was higher than that reported by Mansoor K and colleagues (51% vs. 44.2%), whereas the proportion of traffic-related injuries was similar (22.9% vs. 26.7%) (17). These variations may be influenced by differences in local environments, community safety practices, and healthcare-seeking behaviors, and they underscore the importance of considering regional context when comparing epidemiological data.
Upper-limb fractures were the most frequent injuries in our cohort, with supracondylar humeral fractures particularly common in younger children. Femoral fractures, in contrast, were more likely to require hospitalization. These patterns highlight the importance of appropriate triage and timely surgical evaluation for high-energy trauma (18, 19). Prevention efforts may also benefit from being tailored to developmental stages. For younger children, closer supervision and safer home environments could help reduce fall-related injuries. School- aged children may benefit from safety education focused on playground and sports activities, while adolescents could be encouraged to use protective equipment such as bicycle helmets to reduce the risk of traffic- and cycling-related fractures.
Conclusion
Pediatric fractures in this regional cohort varied by sex, age, season, and injury mechanism, with boys and adolescents showing the highest overall risk. Younger children were mainly affected by fall-related injuries, while adolescents experienced more traffic- and sports-related trauma. Upper-limb fractures were the most common overall, and femoral fractures were more likely to require hospitalization. These patterns suggest that prevention and clinical management may benefit from being tailored to different age groups. Although this study reflects the experience of a single center, the findings offer useful epidemiological information that may help guide future multicenter work and support the development of locally appropriate injury-prevention strategies.
Limitations
This study has several limitations that should be taken into account when interpreting the results. First, it was conducted at a single tertiary care center, which may limit the generalizability of the findings to other settings. Second, referral bias may exist, as more severe cases are likely to seek hospital care, potentially inflating the proportion of high-energy injuries and surgical admissions. Third, the study lacked denominator data on the underlying population distribution by age group, preventing calculation of true incidence rates and restricting comparisons across age strata. These factors highlight that our results should be interpreted cautiously and may not be universally applicable. Future multicenter studies incorporating population-based data are needed to validate and extend these findings.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Hedström EM Svensson O Bergström U Michno P. Epidemiology of fractures in children and adolescents. Acta Orthop. (2010) 81(1):148–53. 10.3109/1745367100362878020175744 PMC 2856220 · doi ↗ · pubmed ↗
- 2Hu X Lin X Dai Z Fang K. Global burden of pediatric fracture (1992-2021) and projections of future disease burden trends. BMC Pediatr. (2025) 25(1):416. 10.1186/s 12887-025-05767-640413433 PMC 12102943 · doi ↗ · pubmed ↗
- 3Segal D Slevin O Aliev E Borisov O Khateeb B Faour A Trends in the seasonal variation of paediatric fractures. J Child Orthop. (2018) 12(6):614–621. 10.1302/1863-2548.12.18011430607209 PMC 6293327 · doi ↗ · pubmed ↗
- 4Cooper C Dennison EM Leufkens HG Bishop N van Staa TP. Epidemiology of childhood fractures in Britain: a study using the general practice research database. J Bone Miner Res. (2004) 19(12):1976–81. 10.1359/jbmr.04090215537440 · doi ↗ · pubmed ↗
- 5Mamoowala N Johnson NA Dias JJ. Trends in paediatric distal radius fractures: an eight-year review from a large UK trauma unit. Ann R Coll Surg Engl. (2019) 101(4):297–303. 10.1308/rcsann.2019.002330855170 PMC 6432966 · doi ↗ · pubmed ↗
- 6Talbot C Davis N Majid I Young M Bouamra O Lecky FE Fractures of the femoral shaft in children: national epidemiology and treatment trends in England following activation of major trauma networks. Bone Joint J. (2018) 100-B(1):109–118. 10.1302/0301-620X.100B 1.BJJ-2016-1315.R 329305459 · doi ↗ · pubmed ↗
- 7Rennie L Court-Brown CM Mok JY Beattie TF. The epidemiology of fractures in children. Injury. (2007) 38(8):913–22. 10.1016/j.injury.2007.01.03617628559 · doi ↗ · pubmed ↗
- 8Jones IE Williams SM Dow N Goulding A. How many children remain fracture-free during growth? A longitudinal study of children and adolescents participating in the dunedin multidisciplinary health and development study. Osteoporos Int. (2002) 13(12):990–5. 10.1007/s 00198020013712459942 · doi ↗ · pubmed ↗