Case Report: Fabrication of a plumper-type music splint for saxophone performance in a patient with a full-arch implant-supported prosthesis
Mariko Hattori, Yuichi Yamatani, Yuka Sumita, Noriyuki Wakabayashi

TL;DR
A custom splint improved a saxophone player's performance after dental implants reduced mouth support.
Contribution
A novel plumper-type splint was developed to enhance embouchure stability in wind instrument players with implant-supported prostheses.
Findings
The splint improved playing comfort and reduced fatigue in a saxophone player with a full-arch implant prosthesis.
Buccal stability and low-register tone production improved to clinically meaningful levels after splint use.
After one year, the patient reported increased ease and confidence during performance with prolonged note duration.
Abstract
The orofacial region, particularly the lips, tongue, and teeth, plays a critical role in wind instrument performance. Wind instrument players may experience lip pain, trauma, or discomfort during performance. In patients rehabilitated with fixed implant-supported full-arch prostheses, reduced soft tissue support and intraoral volume may compromise embouchure stability and endurance. A 55-year-old male amateur saxophone player reported early fatigue and difficulty maintaining embouchure stability after receiving a fixed implant-supported full-arch prosthesis. Clinical examination revealed a space between the prosthetic superstructure, residual alveolar ridge, and buccal mucosa. To compensate for the reduced intraoral tissue volume, a plumper-type music splint worn exclusively during instrument playing was planned. The appliance was initially fabricated as a provisional music splint,…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
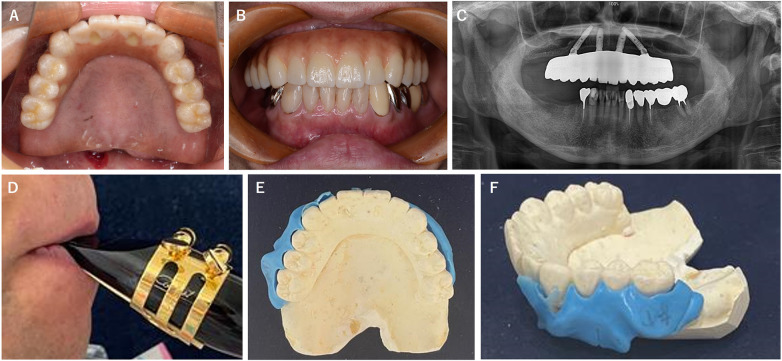 Figure 1
Figure 1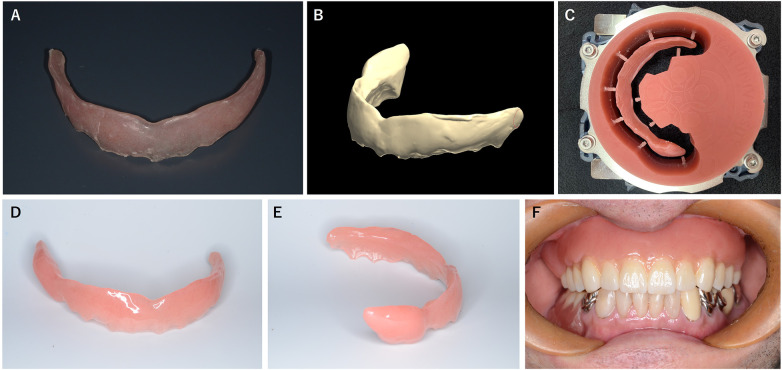 Figure 2
Figure 2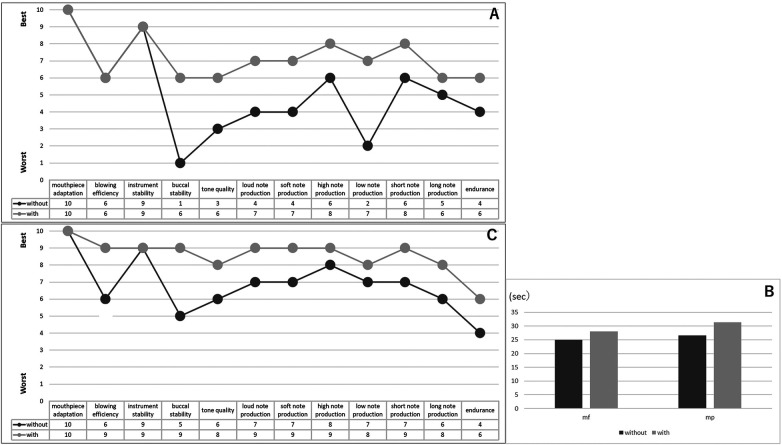 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMusicians’ Health and Performance · Music Technology and Sound Studies · Voice and Speech Disorders
Introduction
1
The orofacial region, particularly the lips, tongue, and teeth, plays an important role in wind instrument performance (1, 2). Wind instrument players may experience pain, trauma, or discomfort of the lips, occasionally leading to ulceration (3, 4). Appliances designed to protect the lips during playing have long been described in the literature. Porter introduced a lip shield for woodwind players (5), and similar devices have been referred to as embouchure aids, intended to reduce lip irritation during performance (6). The term music splint is a collective designation for removable intraoral performance-assist devices used during wind instrument playing (7). Previous studies have demonstrated that music splints can influence both the produced sound and the player's subjective evaluation of performance (4).
In addition to performance aids, prosthetic dental treatment is sometimes required for wind musicians who have lost teeth in order to continue their musical career. Removable prostheses have been reported in the literature for such patients (8), and implant-supported prostheses have also been applied in cases of partial tooth loss with consideration of musical performance (9). In recent years, however, fixed prosthetic rehabilitation using dental implants has become more common than removable prostheses, even in full-arch cases. Although fixed implant-supported prostheses offer many benefits, the lack of a denture base often results in insufficient restoration of alveolar bone and soft tissue volume, which can affect speech (10), facial contour, and potentially wind instrument performance.
A plumper is a removable maxillofacial prosthesis designed to provide additional bulk to the soft tissues. It is commonly used in patients with maxillofacial defects who require increased lip support following tumor resection and reconstructive surgery (11) or in cases of congenital malformation (12). The concept of a plumper was adapted in the present case, in which a patient experienced difficulty playing the saxophone after full-mouth rehabilitation with an implant-supported prosthesis. The plumper used in this patient was a plumper-type music splint, designed specifically for musical performance and worn only during instrument playing. The condition was successfully managed with this appliance, which is described in this report.
Case description
2
A 55-year-old male amateur saxophone player presented with complaints of early fatigue during instrument performance. He reported that this difficulty had developed after receiving a fixed implant-supported full-arch prosthesis in the maxilla at another clinic. The patient regularly played the alto saxophone as a member of an amateur orchestra. His embouchure was of the single-lip type, and his principal playing style also relied on single-lip technique.
Diagnostic assessment
2.1
Intraoral examination revealed a completely edentulous maxilla restored with a fixed implant-supported prosthesis (Figures 1A–C). A space was observed between the prosthetic superstructure, the residual alveolar ridge, and the buccal mucosa. To evaluate the embouchure condition during performance, a functional impression was made using silicone impression material while the patient played (13). This procedure revealed a pronounced lateral embouchure gap, particularly on the right side (Figures 1D–F).
The patient's condition at the first visit. (A) Intraoral occlusal view. (B) Intraoral frontal view. (C) Panoramic x-ray of the upper and lower jaws. (D) The embouchure while the patient was playing the clarinet. (E) Lateral dental impression on the maxillary model, occlusal view. (F) Lateral dental impression on the maxillary model, lateral view.
Based on these findings, a treatment plan was formulated to fabricate a plumper-type music splint designed to fill the existing space and provide improved support during saxophone performance. While reconstruction of the prosthetic superstructure was considered, it was deemed unnecessary, as the difficulty occurred only during saxophone playing and the existing prosthesis functioned adequately in daily activities; furthermore, remaking the superstructure would have imposed a significant financial burden.
Therapeutic intervention
2.2
A preliminary impression of the maxilla was obtained using irreversible hydrocolloid impression material (Hi-Technicol, GC, Tokyo, Japan). A frame was fabricated using a vacuum-adapted thermoforming technique with a 1.5 mm thick polyethylene terephthalate disk (Splint Clear 1.5 mm, Yamahachi Dental, Gamagori, Japan). Auto-polymerizing dental acrylic resin (Unifast III, GC, Tokyo, Japan) was added intraorally, and the device was adjusted according to the patient's perception of blowing comfort. The splint was then polished using an abrasive bur, producing a provisional music splint (Figure 2A).
The fabrication of the definitive music splint using the data from the provisional splint. (A) Provisional music splint. (B) Digitized surface data of the provisional splint. (C) Milled acrylic disk used to fabricate the definitive music splint. (D) Frontal view of the completed definitive splint. (E) Lateral view of the completed definitive splint. (F) The definitive music splint in place.
After one month of use during musical activity, the provisional splint was reported to function without any issues. It was then digitized using a model scanner (D2000 Lab Scanner, 3Shape, Copenhagen, Denmark) to acquire three-dimensional data (Figure 2B). The definitive plumper-type music splint was designed using dental computer-aided design software (3Shape Dental System, 3Shape, Copenhagen, Denmark) and general-purpose 3D modeling software (Meshmixer, Autodesk, San Francisco, CA) based on the scanned data. The splint was subsequently fabricated via computer-controlled milling using a dental milling machine (DWX-52DC, DGSHAPE, Hamamatsu, Japan) and auto-polymerizing denture base acrylic resin (Palapress vario, Kulzer, Hanau, Germany) (Figure 2C) and polished (Figures 2D,E).
The definitive splint was delivered to the patient (Figure 2F) and adjusted according to his feedback while playing the instrument. Both subjective and objective evaluations were then performed.
Follow-up and outcomes
2.3
Performance evaluation included measurement of the maximum sustained note duration. The patient was instructed to sustain an E♭3 note at mezzo-forte (mf) and mezzo-piano (mp) levels, each repeated three times. The duration was measured in seconds, and the average value was recorded.
Subjective evaluation of playing comfort was conducted using a 10-point scale for the following items: mouthpiece adaptation, blowing efficiency, instrument stability, buccal stability, tone quality, loud note production, soft note production, high note production, low note production, short note production, long note production, and endurance. This scale was adapted from those used in previous studies, with additional items included based on the patient's feedback to better capture performance-related difficulties (4, 8, 9). Additional qualitative feedback regarding the overall playing experience was also obtained. The evaluation was repeated after one year of use during the patient's regular check-up.
The plumper-type music splint fit well, and the patient was able to use it in daily practice and on stage without any problems. He reported that he could practice for a longer time when the splint was worn, and no mucosal complications were observed on the soft tissues adjacent to the splint. Figure 3A shows the questionnaire results one month after delivery. Almost all items were rated favorably when the splint was worn, and even those that had been very low, such as buccal stability and low-tone production without the splint, showed marked improvement. Regarding qualitative feedback, the patient reported that without the splint his lips became fatigued and air leaked laterally, the sound sometimes became breathy or trembled, weak tones were difficult to produce as intended, and he became fatigued easily, which made him anxious. On the other hand, when the splint was worn, he felt that airflow was stabilized, pressure did not escape laterally, and he could articulate tones as intended, which gave him confidence. He also mentioned, however, that he was still struggling with the endurance and stability of his embouchure.
(A) The results of the questionnaire after using the definitive music splint for one month. “with” indicates performance with the music splint; “without” indicates performance without the music splint. (B) The maximum blowing time with and without using the music splint. (C) The results of the questionnaire after using the definitive music splint for one year.
Figure 3B shows the results of the long-tone assessment, and Figure 3C shows the questionnaire results after one year of splint use. The maximum sound duration was longer with the splint in both mf and pp blowing. The questionnaire also indicated that, after one year of splint use, scores had improved even when the splint was not worn. In terms of qualitative feedback after adjustments, the patient reported that without the splint the tone lacked density and sometimes became breathy, whereas with the splint air leakage was prevented, intraoral pressure could be maintained, and he could concentrate on performance without unnecessary muscular effort. In addition, compared with the initial stage, he reported that he had become able to play with harder reeds, changing from 2½ to 3½, and he also felt that the facial surface remained more stable during blowing.
Discussion
3
In this case, the implant-supported prosthesis previously delivered at another clinic provided adequate function for mastication but presented difficulties during wind instrument performance. While oral functions such as speech, swallowing, and mastication are well recognized, the functional requirements for musical performance are often overlooked. Raising dentists’ awareness of other oral functions, such as singing and playing musical instruments, is desirable for future practice.
The use of a plumper-type music splint improved the patient's playing comfort compared with the non-use condition and reduced fatigue during performance, allowing the patient to participate confidently in orchestral activities. With the use of the plumper-type music splint, the patient's subjective evaluation improved to a level comparable to post-treatment conditions reported in previous case reports (4, 8, 9). Plumpers are usually used to compensate for intraoral space and to support soft tissues (11, 12). In this patient, difficulty in playing was attributed to the inability of the existing implant-supported full-arch prosthesis to fully restore the lost alveolar bone, even though the teeth were prosthetically reconstructed. Therefore, the use of a plumper-type device was well suited to address the functional issue in this case. No conclusions regarding reed hardness or facial symmetry can be drawn from a single case. Further investigation, including facial measurements during instrument performance (14), is warranted.
Several limitations should be acknowledged. Because retention of the plumper-type music splint relies on engaging the undercut by utilizing the flexibility of the material, its long-term durability with prolonged use remains uncertain. In addition, compared with the porcelain surface of the prosthetic superstructure, the material characteristics of the splint may predispose it to increased plaque accumulation, surface degradation, or discoloration over time. Nevertheless, as a removable device, a music splint poses fewer risks to performance compared with irreversible treatments, making it a suitable and low-risk option for wind instrument players (4). It is essential to design the splint according to the individual's oral conditions and to provide a device optimized for musical performance. It should also be noted that if a removable prosthesis had been selected instead of a fixed reconstruction, the prosthesis itself might have been more easily modified by adding or reducing material to accommodate musical performance (8). When planning prosthetic treatment for wind instrument players, treatment options should therefore be carefully discussed with the patient not only in terms of their general advantages and disadvantages, but also from the perspective of instrument performance.
Conclusion
4
In this case, the plumper-type music splint successfully compensated for the reduced intraoral tissue volume associated with the existing implant-supported prosthesis, resulting in improved embouchure stability and greater playing comfort. As a removable and minimally invasive approach, this appliance may serve as a practical adjunctive option for wind instrument players who develop performance-related functional difficulties after fixed full-arch implant rehabilitation.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Woldendorp K Boschma H Boonstra A Arendzen H Reneman M. Fundamentals of embouchure in brass players: towards a definition and clinical assessment. Med Probl Perform Art. (2016) 31:232–43. 10.21091/mppa.2016.403827942703 · doi ↗ · pubmed ↗
- 2Clemente M Mendes J Moreira A Bernardes G Van Twillert H Ferreira A A new classification of wind instruments: orofacial considerations. J Oral Biol Craniofac Res. (2019) 9:268–76. 10.1016/j.jobcr.2019.06.01031249774 PMC 6587030 · doi ↗ · pubmed ↗
- 3Yeo D Pham T Baker J Porter S. Specific orofacial problems experienced by musicians. Aust Dent J. (2002) 47:2–11. 10.1111/j.1834-7819.2002.tb 00296.x 12035952 · doi ↗ · pubmed ↗
- 4Tanabe G Hattori M Obata S Takahashi Y Churei H Nishiyama A Case report: psychoacoustic analysis of a clarinet performance with a custom-made soft lip shield worn to prevent mucosal erosion of lower lip. Front Psychol. (2022) 13:852866. 10.3389/fpsyg.2022.85286635529561 PMC 9069104 · doi ↗ · pubmed ↗
- 5Porter MM. Dental problems in wind instrument playing. 2. Single-reed instruments–the lip shield. Br Dent J. (1967) 123:441–3.4863318 · pubmed ↗
- 6Krivin M Conforth SG. An embouchure aid for clarinet and saxophone players. J Am Dent Assoc. (1975) 90:1277–81. 10.14219/JADA.ARCHIVE.1975.02511056395 · doi ↗ · pubmed ↗
- 7Nii M Yoda N Putra RH Aida J Sasaki K. Evaluation of the optimal hardness and thickness of music splints for wind instrument players. J Prosthet Dent. (2023) 129:754–62. 10.1016/J.PROSDENT.2021.06.04434364689 · doi ↗ · pubmed ↗
- 8Hattori M Sumita YI Taniguchi H. Sound analysis of a musical performance to evaluate prosthodontic treatment for a clarinet player. J Prosthodont. (2015) 24:71–7. 10.1111/jopr.1216624920520 · doi ↗ · pubmed ↗