Cemented implantation of a dual mobility cup in an existing acetabular cup to prevent recurrent dislocation after total hip replacement
E. Saleh, S. Yacoub, C. Pempe, A. Roth, M. Ghanem

TL;DR
This study evaluates a technique for preventing hip dislocation after hip replacement surgery using a dual mobility cup implanted in an existing acetabular cup.
Contribution
The study introduces cementing a dual mobility cup in a pre-existing acetabular cup as an alternative to direct bone implantation.
Findings
Cementing a dual mobility cup in a fixed acetabular cup showed similar outcomes to direct implantation into bone.
The technique was effective in reducing dislocation rates in older patients undergoing revision hip replacement.
No significant differences were found between the two implantation techniques in clinical outcomes.
Abstract
Recurrent hip dislocation is a common complication following total hip arthroplasty (THA). The dual mobility cup (DMC) technique was introduced to reduce the risk of dislocation. Cementing DMC in a fixed acetabular cup may be a good alternative to the usual approach of implanting it directly into bone. We aimed to evaluate the outcome of DMC in preventing recurrent THA dislocation. In addition, we examined differences in clinical outcomes between the two techniques: cementation into a pre-existing acetabular cup versus direct implantation into bone. The sample comprised 20 patients who underwent surgery using the DMC technique between 2014 and 2023. The primary endpoint was time to the occurrence of postoperative revision operation for any reason, assessed by the Kaplan-Meier survival analysis with a significance threshold of p < 0.05. This retrospective comparative study included a…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
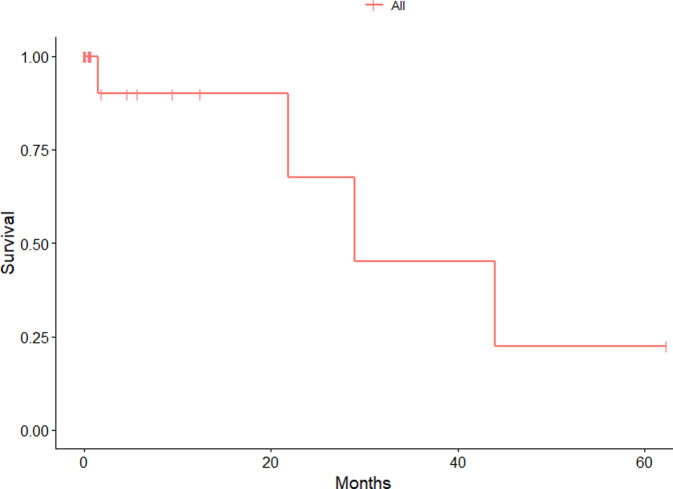 Figure 1
Figure 1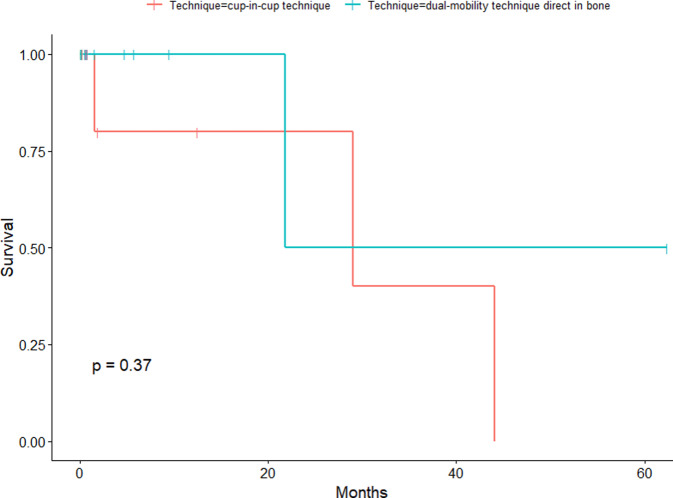 Figure 2
Figure 2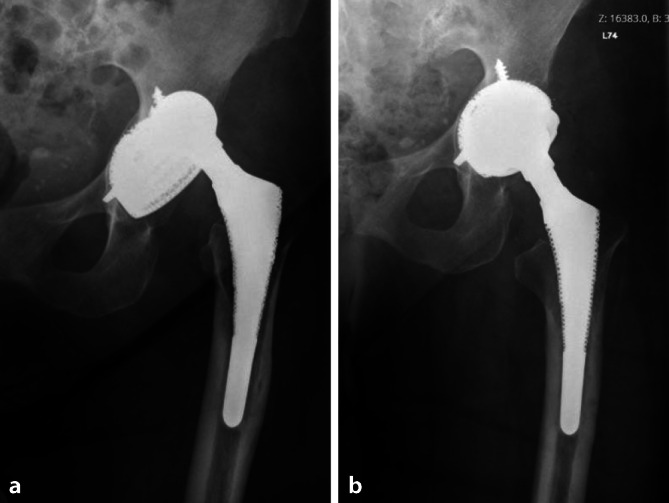 Figure 3
Figure 3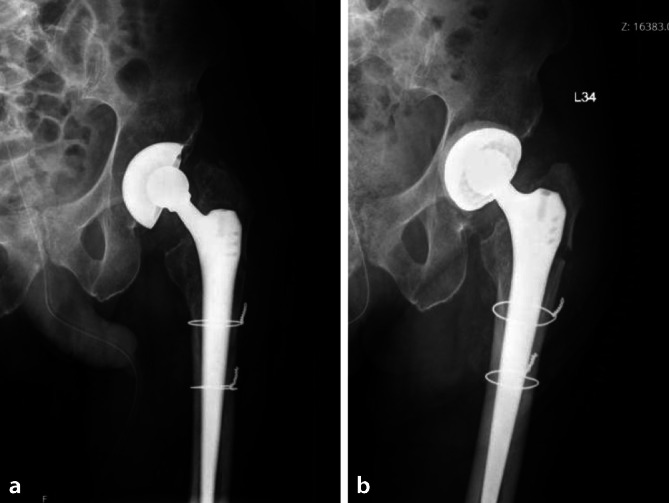 Figure 4
Figure 4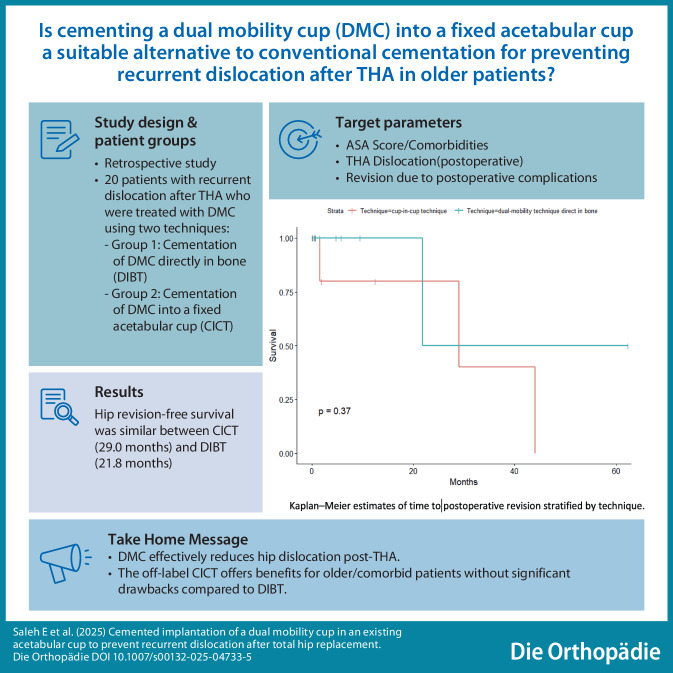 Figure 5
Figure 5 Figure 6
Figure 6- —Universitätsklinikum Leipzig (8929)
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsOrthopaedic implants and arthroplasty · Hip disorders and treatments · Hip and Femur Fractures
Introduction
Total hip arthroplasty (THA) is one of the most commonly used and successful surgical procedures, significantly improving the quality of life in the aging population. It is particularly beneficial for those suffering from coxarthrosis or a fractured neck of the femur [1]. Hip dislocation is a frequent postoperative complication [2] and a cause of higher morbidity, especially among revision THA operations [3, 4]. Other complications include fractures (18.2%) and surgical site infections (17.2%) [5]. The hip dislocation rate after revision THA is higher in comparison to primary THA and is considered the main cause for further revision THA [6, 7]. The number of THA revision operations is expected to increase by 137% by 2030 [8]. A study by de Cano et al. reported a 35% dislocation rate after THA revision due to instability [9]. In a meta-analysis of 125 studies Kunutsor et al. reported that the incidence rate of instability of the primary THA was 7% and it was 25% higher after revision THA [10].
The main risk factors for THA dislocation can be patient-related or implant-related in addition to the surgeon’s experience. Patient-related factors include previous hip operations, advanced age and lack of abductor muscular support [11–13]. Furthermore, Kunutsor et al. reported that white race, high American Society of Anesthesiologists (ASA) score, high body mass index (BMI) > 30 kg/m^2^, low social level, drug use as well as psychiatric and neurological disorders increase the risk of dislocation [10]. Implant-associated factors include the size of the femoral head, the size of the acetabular cup and the degree of femoral neck offset [14]. For example, Jameson et al. reviewed 247,546 procedures and reported a decline in postoperative dislocation incidence with the use of larger femoral heads [15].
The dual mobility cup (DMC) was pioneered in the 1970s by Bousquet and Rambert [16]. The DMC features a bipolar component that moves inside a fixed large diameter metal shell and it provides a better range of motion (ROM) before impingement. Therefore, it is expected to provide better stability with a lower rate of dislocation [17, 18]. Civinini et al., Jakobsen et al. and Van Heumen et al. reported successful clinical results for treating recurrent THA dislocation using DMC [19–21]. In a study with a 22-year follow-up of 240 hips using DMC, recurrent THA dislocations occurred only in 7 cases (0.2%), which was nonsignificant [22]. Hamadouche et al. also showed successful restoration of hip stability in 96% of 51 patients using DMC during revision THA [23]. The removal of well-fixed components, especially cemented acetabular shells, during revision THA can be highly challenging. This is mainly due to an increased risk of complications such as longer operation times, bone damage, greater blood loss and a higher incidence of infections [24]. One of the DMC approaches was described as “off-label cementation of DMC into a fixed metal shell” [25, 26], which we refer to in our work as the cup-in-cup technique (CICT). This approach was initially used to revise failed THA, particularly in older patients with comorbidities and higher ASA scores, with the aim of reducing complications [26, 27].
Herein we present two approaches for using DMC in THA revision surgery, the previously mentioned CICT versus the implantation directly into bone, which we referred to as direct-in-bone technique (DIBT). We aimed to assess the difference using DMC between both techniques in terms of stability and rate of dislocation.
Patients and methods
Between September 2014 and December 2023, we retrospectively reviewed 20 patients who suffered from recurrent postoperative hip dislocation after primary or revision THA. We included patients who were surgically treated with cementing CICT or DIBT at our center. Patient-related factors for choosing CICT were: (1) recurrent dislocation in which removal of the acetabular component may cause bone loss and/or bleeding, (2) failure of prior surgical hip stabilization operations, or (3) multimorbid situations requiring shorter operation duration to avoid complications. Whenever CICT was not possible due to instability of the pre-existing acetabular cup, we used DIBT. We preferred using DMC rather than constrained liners in those patients because of the increased failure rate and loosening with constrained implants [26, 28, 29].
Baseline characteristics including age, sex, BMI, ASA, date of the primary hip implantation, operation site, previous operations at the same hip joint, number of hip dislocation occurrences before surgery and onset of hip dislocation following the operation were derived from the patients’ electronic records. We also reviewed the digital operative records for information on the duration of surgery, type of implant and complications during the surgery to evaluate the invasiveness of the intervention.
Our main outcome was time (months) to postoperative revision operation following DMC, which was mainly due to postoperative hip dislocation. Secondary outcomes included surgery duration, postoperative complications, capability of mobility using the modified Harris Hip Score (mHHS) [30] as well as the Barthel Index (BI) [31].
Intraoperatively, histological and microbiological samples were taken. All patients were initially investigated with X‑rays in which we planned the expected implant size before the operations.
The patients were examined preoperatively, postoperatively and at discharge and 19 patients were alive at the final follow-up.
The patients were classified into 2 groups based on the surgical technique. Group 1 (10 patients) underwent CICT involving either “cementation of DMC into a preexisting acetabular cup” (7 patients) or in Burch Schneider reinforcement ring (BSR, 3 patients). Group 2 (10 patients) received DIBT for the treatment of hip dislocation. Contrary to De Cano and Trias [9], we considered BSR to fall under CICT to differentiate easily between the groups of interest and to highlight the practical impact on the patients with each technique.
Surgery
The operation was performed with the patient under general anesthesia for all the patients. The anterior lateral approach was used in all patients, following previous THA operations. After hip exposure, the femoral head and polyethylene (PE) liner were removed. The acetabular cup as well as the femoral shaft were tested for stability. The surgeon checked whether the acetabular cup was loose or not and chose the appropriate technique (either CICT or DIBT). For DMC implantation as CICT, the screws (if present) were removed and the acetabular cup direction was assessed to determine the better direction for the DMC. The DMC components were determined according to the previous planning on X‑ray imaging. Then, the DMC was placed and cemented with the desired inclination. The cement hardened in 8–10 min and was then irrigated and trial components were used to verify its size and stability. The definite metal head and liner were inserted and checked for impingement or dislocation. Vancomycin powder was applied before closure of the wound in 30% of patients [32] and the wound was closed layer by layer.
The hip instability or subluxation after the operation was considered as a form of dislocation. In this research, instability and/or subluxation was defined by detecting any abnormal movement of the hip joint coupled with pain or any audible clunk, or any sign of instability in X‑ray images.
Statistical analysis
Continuous variables were presented as mean and standard deviation (SD) while categorical variables as frequencies and percentages. Statistical significance was evaluated using the independent t‑test for continuous variables when assumptions of normality were met, or nonparametric tests otherwise. The χ^2^-test was used for categorical variables as appropriate. Survival analysis was performed via the Kaplan-Meier method. A p-value of ≤ 0.05 was considered statistically significant. We conducted statistical analyses via the Statistical Package for the Social Sciences (SPSS) software (version 26.0) (IBM, Armonk, NY, USA).
Results
Baseline characteristics
A total of 20 patients participated in this study. Half of the patients underwent CICT and the other half underwent DIBT for the treatment of recurrent hip dislocation after THA. The study included 15 women and 5 men with a mean age at the time of the operation of 77.65 ± 13.10 years (range 34–95 years) and 1 patient died shortly after the operation as she had multiple comorbidities. The mean follow-up duration was 9.91 ± 17.01 months. The mean BMI was 26.36 kg/m^2^ (range 19.2–41.4 kg/m^2^). Regarding ASA scores, the mean was 2.6, with 8 patients (40%) having ASA II and 12 patients (60%) having ASA III.
All revision operations were performed for THA dislocation. Among the patients, 16 patients (80%) had recurrent dislocation, 2 patients (10%) had dislocation with femoral loosening, 1 patient (5%) had a dislocation with periprosthetic fracture, and 1 patient (5%) had a dislocation with acetabular fracture. The mean number of preoperative dislocations was 2.90 ± 1.97. The most common secondary diagnoses at the time of surgery were osteoporosis (12 patients) and hypertension (11 patients). At the time of the revision hip operation, all patients had a history of at least 1 previous hip operation, with a mean of 2.30 ± 1.95 (range 1–7). The mean duration of hospitalization was 15.75 ± 8.06 days, 12 surgeries (60%) were performed on the right hip, while the remaining surgeries (40%) were performed on the left hip (Table 1).Table 1. Baseline characteristicsBaseline*Age at surgery (years) **±**SD (range)*77.65 ± 13.10 (34–95)ASA score2.6 ± 0.5ASA 28/20 (40.0%)ASA 312/20 (60.0%)DiagnosisDislocation with acetabular fracture1 (5.0%)Dislocation with acetabular loosening2 (10.0%)Dislocation with periprosthetic femoral fracture1 (5.0%)Recurrent dislocation16 (80.0%)Surgery duration (min)96.55 ± 45.90Site of operationLeft8 (40.0%)Right12 (60.0%)Technique typeCup-in-cup10 (50.0%)Dual-mobility cup directly in bone10 (50.0%)Follow-up duration (months)9.91 ± 17.01Hospital stay (days)15.75 ± 8.06Patient mobility before the operationAble to walk only using 2 forearm crutches (limping)2 (10.0%)Impaired ability to walk and stand due to pain1 (5.0%)Mobile using a wheelchair2 (10.0%)Not mobile due to hip dislocation13 (65.0%)Not mobile due to periprosthetic femoral fracture1 (5.0%)Not mobile in ICU1 (5.0%)SexFemale15 (75.0%)Male5 (25.0%)ASA American Society of Anesthesiologists, ICU intensive care unit
The distribution of the number of revision operations was as follows: 2 revision surgeries among 9 patients, 3 among 4 patients, 4 among 3 patients, 5 among 3 patients and 8 surgeries in 1 patient. One patient had a preoperative infection that was successfully treated at the time of surgery. The revision operation was performed at an average of 8 years (range 1 month–25 years) after the primary THA operation.
The mean number of previous revision operations in the same hip joint was 2.30 ± 1.55. After the operation, the mean number of hip joint dislocations was 0.40 ± 0.97. The size of the cups used in the surgeries had a mean of 51.25 ± 4.64 mm. All patients did not require wearing an antidislocation brace or bandage after the operation (Table 2). Intraoperative complications, including fractures, cardiovascular events, pulmonary embolism and death did not occur in any of the patients.Table 2. Output table illustrates the comparative analysis of CICT and DIBVariableLevelsCICT (n = 10)DIBT (n = 10)P-valueAge of the patient at the time of the operation (years mean ± SD)–79.10 ± 7.7176.2 ± 19.19–ASA score at the time of the operation (%)ASA 250%30%–ASA 350%70%Previous operations in the same hip joint (%)Yes10 (100.0%)10 (100.0%)NANumber of previous operations in the same hip joint (mean ± SD)–2.30 ± 1.952.30 ± 1.161Number of previous revision operations in the same hip joint (%)1 operation5 (50.0%)3 (30.0%)0.6692 operations2 (20.0%)3 (30.0%)–3 operations1 (10.0%)2 (20.0%)–4 operations1 (10.0%)2 (20.0%)–7 operations1 (10.0%)0 (0.0%)–Patients had hip dislocations before the operation (%)Yes10 (100.0%)10 (100.0%)NANumber of hip dislocations before the operation (mean ± SD)–2.40 ± 2.173.40 ± 1.780.274Number of hip dislocations before the operation (%)0 operation1 (10.0%)0 (0.0%)0.0771 operation4 (40.0%)1 (10.0%)–2 operations2 (20.0%)2 (20.0%)–3 operations0 (0.0%)4 (40.0%)–4 operations1 (10.0%)0 (0.0%)–5 operations0 (0.0%)2 (20.0%)–6 operations2 (20.0%)0 (0.0%)–7 operations0 (0.0%)1 (10.0%)–Patients had hip dislocation after the operation (%)No8 (80.0%)8 (80.0%)1Yes2 (20.0%)2 (20.0%)–Number of hip dislocations after the operation (mean ± SD)–0.40 ± 0.97 0.30 ± 0.670.791Number of hip dislocations after the operation (%)0 operation8 (80.0%)8 (80.0%)0.5721 operation1 (10.0%)1 (10.0%)–2 operations0 (0.0%)1 (10.0%)–3 operations1 (10.0%)0 (0.0%)–Wearing an antidislocation brace (%)No10 (100.0%)10 (100.0%)NAWearing an antidislocation bandage (%)No10 (100.0%)10 (100.0%)NAIntraoperative complicationsFracture (%)No10 (100.0%)10 (100.0%)NACardiovascular event (%)No10 (100.0%)10 (100.0%)NAPulmonary embolism (%)No10 (100.0%)10 (100.0%)NADeath (%)No10 (100.0%)10 (100.0%) NAPostoperative complicationsRenewed dislocation (%)No8 (80.0%)8 (80.0%)1Yes2 (20.0%)2 (20.0%)–Loosening (%)No9 (90.0%)9 (90.0%)1Yes1 (10.0%)1 (10.0%)–Liner wear (%)No9 (90.0%)10 (100.0%)1Yes1 (10.0%)0 (0.0%)–Had postoperative revision operations (%)No7 (70.0%)9 (90.0%)0.576Yes3 (30.0%)1 (10.0%)–Postoperative revision operations (mean ± SD)–0.40 ± 0.70 0.20 ± 0.630.511Postoperative revision operations (%)0 operation7 (70.0%)9 (90.0%)0.3251 operation2 (20.0%)0 (0.0%)–2 operations1 (10.0%)1 (10.0%)–Postoperative complication: hip infection (%)No8 (80.0%)8 (80.0%)1Yes2 (20.0%)2 (20.0%)–Postoperative complication: wound infection (%)No9 (90.0%)10 (100.0%)1Yes1 (10.0%)0 (0.0%)–Internal in-hospital postoperative complication: pulmonary embolism (%)No9 (90.0%)10 (100.0%)1Yes1 (10.0%)0 (0.0%)–Internal in-hospital complication: pneumonia (%)No10 (100.0%)9 (90.0%)1Yes0 (0.0%)1 (10.0%)–Internal in-hospital complication: urinary infection (%)No8 (80.0%)8 (80.0%)1Yes 2 (20.0%)2 (20.0%)–Internal in-hospital complication: cardiovascular (%)No 9 (90.0%)9 (90.0%)1Yes1 (10.0%)1 (10.0%)–Internal in-hospital complication: death (%)No10 (100.0%)9 (90.0%)1Yes0 (0.0%)1 (10.0%)–Ability to walk at discharge (%)Mobile using 2 forearm crutches under pain-adapted full load4 (40.0%)3 (30.0%)0.214Mobile using 2 forearm crutches with 20 kg partial load3 (30.0%)2 (20.0%)–Mobile using rollator0 (0.0%) 3 (30.0%)–Patient at the walking bench with pain-adapted full weight bearing with support for a few steps in the room mobile2 (20.0%) 0 (0.0%)–To the edge of the bed and to the walking bench 2–3 steps1 (10.0%)0 (0.0%)–Mobile using wheelchair0 (0.0%)1 (10.0%)–Not mobile in ICU0 (0.0%)1 (10.0%)–Barthel index postoperatively (mean ± SD)–81.00 ± 17.2971.11 ± 25.950.337Modified Harris hip score mHHS after the operation (mean ± SD)–60.89 ± 14.6548.67 ± 23.070.198*ASA *American Society of Anesthesiologists, CICT cup in cup technique, DIBT direkt in bone technique, ICU intensive care unit, SD standard deviationData are presented as mean ± SD or number (percentage). Categorical variables were analyzed via the χ^2^ test or Fisher’s exact test, and the independent t‑test test was used for continuous variables. P-values ≤ 0.05 were considered statistically significant.
Outcome
A comparison of the two surgical techniques revealed that the mean operation duration for CICT was 102.80 ± 57.51 min, whereas that for DIBT was 91.42 ± 31.31 min (p = 0.657). The mean follow-up duration for CICT was 9.10 ± 15.33 months and for DIBT it was 11.74 ± 20.23 months (p = 0.75). Assessing the mHHS at the last follow-up after the operation revealed a mean score of 60.89 for the CICT group and 48.67 for the DIBT group (p = 0.198) (Table 2). In terms of postoperative walking ability, both groups had improved outcomes compared to the preoperative conditions. Following the operation, all patients who underwent CICT were mobile, whereas 80% of those who received DIBT were mobile. In practice, there was no significant difference in mobility outcomes between the CICT and DIBT groups (p = 0.214) (Table 2).
We found that two patients in each group experienced postoperative dislocation once. There was no difference in the incidence of postoperative dislocations between the two techniques (p = 1). Postoperative complications, including renewed dislocation or cup loosening, were not significantly different between the two techniques. Postoperative assessment of the Barthel index at discharge revealed a mean score of 81.00 for the CICT group and 71.11 for the DIBT group (p = 0.337) (Table 2).
In conclusion, this study encompassed 20 patients and compared the CICT with the usual DIBT for the treatment of hip dislocation. The results demonstrated no significant differences in patient demographics, operative outcomes, postoperative complications, or functional outcomes between the two surgical techniques in this patient population.
The endpoint of the study was time to postoperative revision of the hip due to any cause after implantation of DMC. All patients with an available final follow-up were included in the survival analysis (Fig. 1). A comparison of the cup survival time between the 2 groups via the Kaplan-Meier method revealed a median survival time of 29.0 months for CICT patients and 21.8 months for DIBT patients. The log-rank test revealed no significant difference in the time to postoperative revision between the two techniques (P = 0.37) (Fig. 2).Fig. 1. Kaplan-Meier estimates of the time to postoperative revision for all techniquesFig. 2Kaplan-Meier estimates of time to postoperative revision stratified by technique
Discussion
This study examined 20 patients who underwent revision THA using cemented DMC in our center from 2014 to 2023. These patients suffered from recurrent dislocation after THA. We focused on the results of DMC in reducing postoperative recurrent hip dislocation and determined whether there was a difference between the 2 implantation techniques (CICT or DIBT).
The type of technique differed according to the indications for the operation, the acetabular bone condition and the state of the pre-existing acetabular cup. If the pre-existing implant was stable and of sufficient size (48 mm or more), the surgeon opted for CICT to minimize bone damage and blood loss (Fig. 3). If the implant was loose, it was removed and DIBT was chosen (Fig. 4).Fig. 3. Case of a 79-year-old man with septic loosening and dislocation after total hip arthroplasty (a). Placement of cemented DMC into the existing well-fixed metal shell “CICT” (b)Fig. 4. Case of a 75-year-old man operated on for multiple recurrent THA dislocations (a), with replacement of prosthetic components and placement of cemented DMC directly to the bone “DIBT” (b)
Our overall goal was to compare the outcomes between CICT and DIBT based on the technique (Table 2). Secondly, we compared the clinical outcomes in our study after the use of DMC in reducing the dislocation rate after revision THA with the findings of previous studies (Table 3). Finally, we compared the outcomes of 10 patients who underwent DMC as CICT (group 1) with those in previous related studies (Table 4).Table 3. Comparison of several clinical studies on the DMC (regardless of the technique used) [33]AuthorYearNumber of patients (only cemented DMC)Surgical approachMean follow up; months, (range), <SD>Aseptic looseningDislocationInfectionRevisionCup survivorship (%)Stambough [34]20178Posterior/posterolateral34.8 (24–63.6)021285Hipfl [35]201815–47 (25–84)012–89Assi [36]201916Posterior/posterolateral72.9 <± 40.5>000098.8Wheelton [37]201954–22.8 (6–60)001195.8Schmidt [38]202059Posterior/posterolateral24 (12–141.6)–4–1395.6Bozon [39]202123Posterior/posterolateral108 <± 12>213287Saleh^1^202320Anterolateral approach9.91 <± 17.01>243490^1^Identifying details have been anonymized for peer reviewTable 4Comparison of clinical studies on the DMC only with CICTStudyNumber of PatientsMean age of patients in years (range)Follow-up (months)ComorbiditiesHip-function preoperative (range)Hip-function postoperative (range)Dislocation postoperative (%)Loosening postoperative (%)Infection postoperative (%)Revisions postoperative (%)Cup Survivorship (%)Mean operation time (min)Stambough [34]860.6 (51–71)34.8–––2/8(25)01/8 (12.5)2/8 (25)85–Evangelista [42]1862 (30–86)36–46 (40–79)65 (41–97)001/16(6.25)1/16 (6.25)100–Chalmers [41]1864 (37–81)36–HHS 47 (37–60)HHS 81 (62–98)3/18 (17)002/18 (11.1)92.3–Wegrzyn [40]2882 (74–93)4256/44%ASA 3/2HHS 71 (69–74)HHS 88 (82–95)000 0–107Moreta [43]1079.2 (71–87)42CCI 4.3HHS 49.3(33–62)HHS 71.3 (22–91)1/10 (10)001/10 (10)92.2–Bellova [26]3378.6 (63–93)30ASA 2.72CCI 5.1–HHS 59.4 (29–91), WOMAC 602/26 (7.7)0102/33 (6)86.8124Saleh^1^1079.1 (66–93)9.1ASA 2.5–mHHS 60.892/10 (20)1/10 (10)2/10 (20)3/10 (30)90102.80ASA American Society of Anesthesiologists (score), CCI Charlson Comorbidity Index; HHS Harris Hip Score, mHHS modified Harris Hip Score; min minutes; n number; WOMAC Western Ontario and McMasters University Osteoarthritis (Index)^1^Identifying details have been anonymized for peer review
We compared our results (regardless of which technique we used) with other studies, including only revision THA in those studies. Our findings revealed 4 patients with post-DMC operation hip dislocation, 2 of whom received a revision surgery. Additionally, post-DMC revision surgery was performed in 1 patient who developed an infection and another 1 who developed femoral stem loosening, amounting to a total of 4 revision surgeries (Table 2). The resulting cup survivorship post-DMC among the 20 patients was 90%. Table 3 illustrates a significant reduction in postoperative dislocation rates following THA, incorporating both our findings and data reported in several previous studies. These findings imply the advantages of using DMC as implants in revision THA.
The comparison between the two techniques (CICT and DIBT) revealed no significant difference in the outcome, as mentioned previously in Table 2. In our work with CICT (group 1), a slightly longer operation time than with the usual technique (group 2) was noticed. On the other hand, it has a shorter operation time than that reported by Wegrzyn et al. and Bellova et al. [26, 40]. We also noted a better outcome in terms of reducing the rate of postoperative dislocation in comparison to preoperative (Table 2). Out of the 10 patients 3 had postoperative revision due to either dislocation, infection or both.
In line with the findings of previous studies, we found favorable outcomes with the use of DMC as CICT technique in group 1 (Table 4). For example, postoperative dislocation proportion after CICT in our study was 20% similar to the findings of Stambough et al. (25%) [34] and Chalmers et al. (17 %) [41]. The cup survivorship in our study was 90%, which falls within the previously reported range (85–100%) [26, 34, 40–43]. It is worth noting that our sample included mostly nonelective revision THA among geriatric patients with multiple comorbidities.
In 2014 De Martino et al. examined the results of different studies on the use of DMC in primary and revision THA. The 5‑year survivorship of DMC was 94.5–98% with a dislocation rate of 1.1–5.5% [6].
After 3 years De Martino et al. published a systematic review of 59 articles evaluating the dislocation rate following THA after implantation of DMC. They divided a total of 17,908 THA into 2 categories: primary THA and revision THA. They reported a dislocation rate of 0.9% in the primary THA patients compared to 3.0% in the revision THA patients. The mean rate of hip dislocation was 0.7% in primary THA patients and 1.3% in revision THA patients [5]. Plummer et al. reported an improved HHS among patients who received revision THA following postoperative dislocation; 45 points preoperatively vs. 90 points postoperatively [44].
Jonker et al. compared the rate of dislocation between DMC and traditional unipolar cups in a systematic review in 2019. The study reported lower rates of hip dislocation and revision after implantation of DMC [45].
Another systematic review by Ciolli et al. including 3426 patients showed the results of cementation of DMC in primary (25.5% of the cases) as well as revision THA (74.5%). The estimated prevalence of overall postoperative dislocation was around 3%, with a cup survivorship of 93.5% [33].
A recent study on DMC by de Cano and Trias in 2023 examined the outcomes of THA revision via a cemented DMC. They divided the patients into 3 groups based on the technique: CICT in pre-existing acetabular cup, DMC in BSR or DIBT. The results revealed an improvement according to the modified disability (MD) scale from 8.34 preoperatively to 15.55 postoperatively [9]. It is worth noting the results of a systematic review highlighting the favorable outcomes of DMC compared to constrained cups. Among 5617 THAs the proportions of dislocation and loosening were lower in DMC (2.6% vs. 11.0%, and 1.0% vs. 2.0%, respectively). Additionally, the cup survival rate was higher in patients who underwent DMC [8]. In summary, all the mentioned studies demonstrated the positive effect of DMC in reducing the dislocation rate, not only in primary cases but also in revision cases.
Recently, some operators have introduced the cementation of DMC in a fixed acetabular cup as an off-label technique (CICT), especially in the management of recurrent hip dislocation. The aim was mainly to reduce intraoperative complications such as blood loss and bone defects as well as operation time. This is particularly useful for frail patients with high surgical risk [26]. We found 6 published studies discussing this technique as an alternative to the usual DMC implantation approach (Table 4). Wegrzyn et al. published a study that included 28 patients, who underwent only elective operations via CICT. They reported no cases of postoperative dislocation or dissociation with HHS 88 at a mean follow-up of 3.5 years [40]. Chalmers et al. and Moreta et al. also demonstrated better postoperative outcomes using CICT. Chalmers et al. reported only 3 cases of dislocation and no dissociation in a study that included 18 patients with HHS of 82 with a mean follow-up of 3 years [41]. Moreta et al. reported only 1 case of dislocation and no dissociation in a study that included 10 patients with HHS of 71 with a mean follow-up of 3.5 years [43].
A study by Bellova et al. in 2021 involving 33 patients, but unlike the other studies included also nonelective cases that amounted to nearly 40%. Bellova et al. reported only 2 patients with dislocation and 1 with dissociation with a mean surgery duration of 124 min [26]. Wegrzyn et al. reported CICT failure because of loosening between the cement and the pre-existing cup, and not between DMC and the cement layer. This was due to the lack of surface roughness or incorrect cementation between DMC and the fixed cup. Consequently, they recommended a cement layer with a thickness of 2–3 mm between the 2 cups and a size difference of 10 mm between the DMC and the outer diameter of the fixed acetabular cup [46]. In accordance with the recommendations of Wegrzyn et al. CICT is not suitable if the fixed acetabular cup is smaller than 54 mm [46]; however, Bellova et al. reported a thinner cement layer in approximately 65% of the cases, as the size of the fixed acetabular cup was smaller than 54 mm. This allows the usage of CICT technique with smaller fixed cup sizes (up to size 48 mm) [26]. Based on our observed results with DMC via CICT, we can consider it as a successful intervention on the short-term follow-up (Tables 2 and 4).
This study had various limitations: it was retrospective, included a small sample size, had short-term follow-up in some cases and involved different implant types; however, one strength of our study was that we included nonelective surgeries in multimorbid patients, unlike previous studies which focused on elective surgeries.
Conclusion
Hip dislocation remains a challenging complication after primary or revision THA. The use of DMC improved the postoperative dislocation rate. The off-label implantation approach (CICT) can provide positive results, particularly in older and comorbid patients, by reducing bone injury, bleeding and in some cases, operative time during short-term follow-up. We did not observe any significant drawbacks when comparing both techniques (CICT and DIBT) in our study; however, we recommend further research with a bigger sample size and a longer follow-up time.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1De Martino I, D’apolito R, Soranoglou VG et al (2017) Dislocation following total hip arthroplasty using dual mobility acetabular components: a systematic review. Bone Joint J 99: 18–2410.1302/0301-620X.99B 1.BJJ-2016-0398.R 128042114 · doi ↗ · pubmed ↗
- 2de Cano JJM, Trias E (2023) The cemented double mobility cup in hip revision: different possibilities of use. Acta Ortopédica Brasileira, 31: e 256913.10.1590/1413-785220233101 e 256913 PMC 1011235137082167 · doi ↗ · pubmed ↗
- 3Kunutsor, S. K., Barrett, M. C., Beswick, A. D., Judge, A., Blom, A. W., Wylde, V., & Whitehouse, M. R. (2019). Risk factors for dislocation after primary total hip replacement: A systematic review and meta-analysis of 125 studies involving approximately five million hip replacements. Lancet Rheumatology 1(2): e 111–e 12110.1016/S 2665-9913(19)30045-138229338 · doi ↗ · pubmed ↗
- 4Guo, L., Yang, Y., An, B., Yang, Y., Shi, L., Han, X., & Gao, S. (2017). Risk factors for dislocation after revision total hip arthroplasty: A systematic review and meta-analysis. International Journal of Surgery 38: 123–12910.1016/j.ijsu.2016.12.12228043927 · doi ↗ · pubmed ↗
- 5Bellova P, Koch F, Stiehler M et al (2021) Cementation of a dual mobility cup in a well-fixed acetabular component—a reliable option in revision total hip arthroplasty? BMC Musculoskeletal Disorders, 22, 98210.1186/s 12891-021-04835-z PMC 861395834819056 · doi ↗ · pubmed ↗
- 6Guyen, O., Lewallen, D. G., & Cabanela, M. E. (2008). Modes of failure of Osteonics constrained tripolar implants: A retrospective analysis of forty-three failed implants. The Journal of Bone and Joint Surgery, 90(7), 1553–1560.10.2106/JBJS.G.0031718594105 · doi ↗ · pubmed ↗
- 7Ciolli, G., Mesnard, G., Deroche, E., Gunst, S., Batailler, C., Servien, E., & Lustig, S. (2023). Is cemented dual-mobility cup a reliable option in primary and revision total hip arthroplasty: A systematic review. Journal of Personalized Medicine, 13(1), 81.10.3390/jpm 13010081 PMC 986715436675742 · doi ↗ · pubmed ↗