The German Cancer Consortium (DKTK) multi-center prospective phase 1/2 68Ga-PSMA-11 PET-imaging trial in newly-diagnosed high-risk prostate cancer: Safety and diagnostic accuracy compared to histopathology and their impact on patient management
Frederik L. Giesel, Stefan A. Koerber, Boris Hadaschik, Selina Kiefer, Sarah Schwarzenboeck, Kambiz Rahbar, Thorsten Derlin, Christoph A. Grott, Matthias Heck, Cordula Jilg, Philipp T. Meyer, Juri Ruf, Karl Schmidt, Joerg Kotzerke, Christian la Fougère, Gerald Reischl

TL;DR
This study shows that 68Ga-PSMA-11 PET/CT imaging is safe and effective for detecting prostate cancer metastases, influencing treatment decisions in high-risk patients.
Contribution
The study provides new evidence on the diagnostic accuracy and clinical impact of 68Ga-PSMA-11 PET/CT in high-risk prostate cancer staging.
Findings
68Ga-PSMA-11 PET/CT had high sensitivity for local disease detection (97.1%) and moderate sensitivity for lymph node metastases (40%).
Imaging led to changes in surgical and radiation therapy plans in 13.2% and 20.9% of patients, respectively.
PSMA uptake correlated with Gleason score, with higher SUVpeak values for higher-grade tumors.
Abstract
Clinically accurate detection of prostate cancer (PCa) metastases is crucial for management of high-risk PCa patients scheduled for radical prostatectomy. We determine the safety and diagnostic accuracy of pre-operative 68Ga-PSMA-11 PET/CT imaging in newly diagnosed high-risk PCa and assess its impact on patient management. Investigator-initiated prospective multi-center multinational single-arm open-label phase 1/2 imaging trial (EuRadCT 2016–001815-19). Patients with high-risk PCa scheduled for prostatectomy were enrolled at 9 institutions in Germany, Austria, and Switzerland to undergo 68Ga-PSMA-11 PET/CT for primary staging. The primary objectives were the evaluation of 68Ga-PSMA-11 PET/CT imaging to detect the primary tumor and lymph node disease and safety assessment. Secondary objectives included detection of distant metastases, correlation of 68Ga-PSMA-11 uptake with Gleason…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
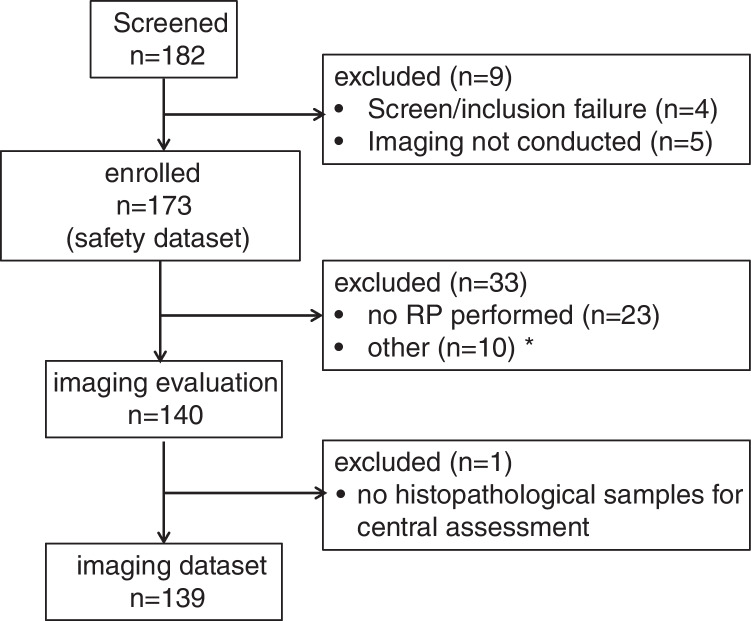 Figure 1
Figure 1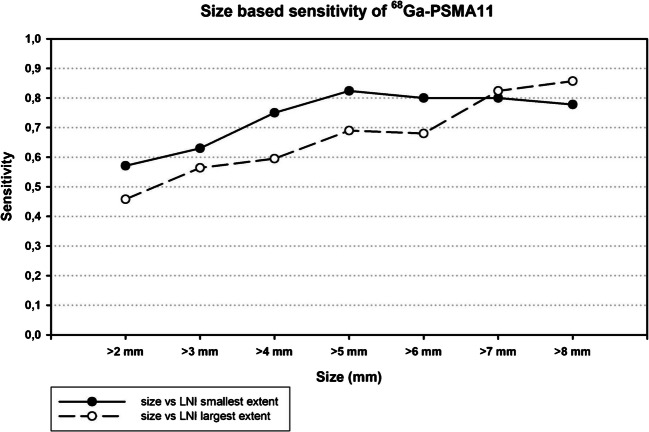 Figure 2
Figure 2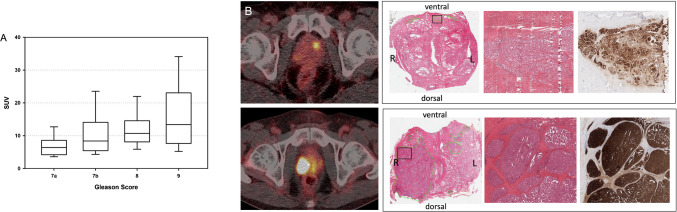 Figure 3
Figure 3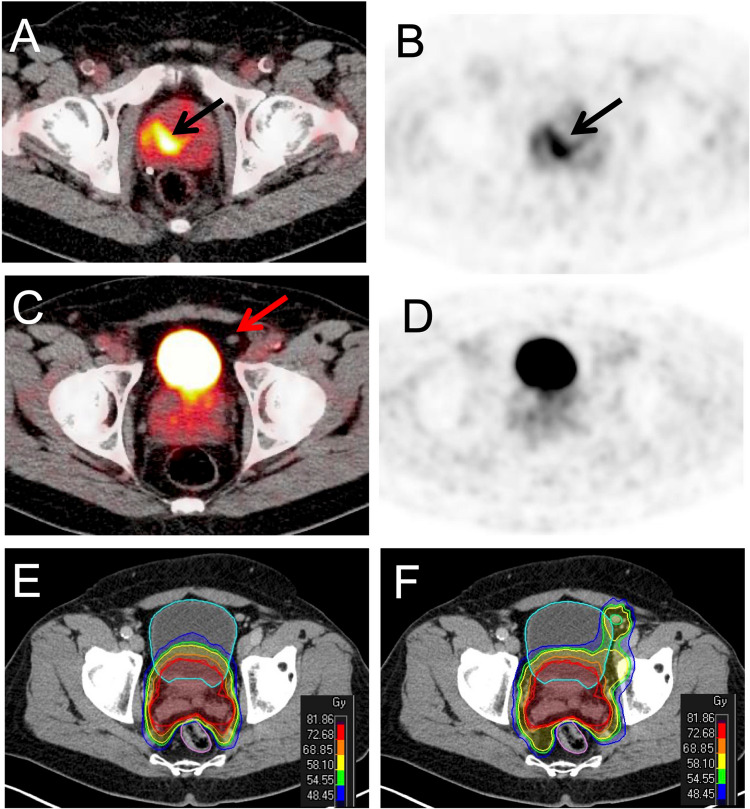 Figure 4
Figure 4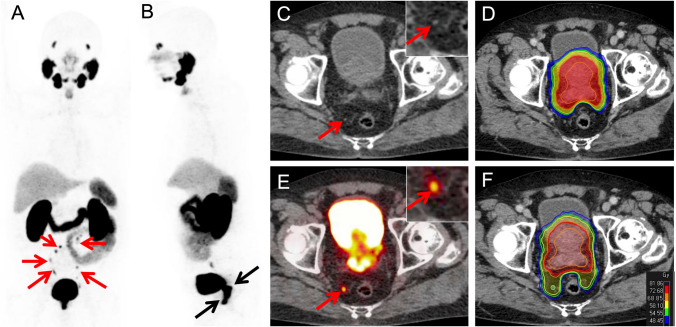 Figure 5
Figure 5- —Technische Universität München (1025)
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsProstate Cancer Treatment and Research · Prostate Cancer Diagnosis and Treatment · Radiopharmaceutical Chemistry and Applications
Introduction
Prostate cancer (PCa) is the second most common malignancy in men worldwide [1]. Staging of newly diagnosed PCa aims to detect both regional nodal involvement (N1) and distant metastatic disease (M1), the presence of which dramatically alters management and prognosis. Until recently, bone scintigraphy and abdominal/pelvic computed tomography (CT) or magnetic resonance imaging (MRI) were the mainstay imaging methods for initial staging of newly diagnosed high-risk prostate cancer [2]. However, cross-sectional imaging by CT or MRI for N-staging proved to have limited diagnostic performance: In a meta-analysis conducted by Hövels et al., cross-sectional imaging modalities yielded low sensitivities for lymph node metastases (pooled sensitivity of 0.42 for CT and 0.39 for MRI) [3]. Notably, in a subsequent prospective trial, Briganti et al. reported an even lower overall sensitivity of 0.13 for CT scans [4]. Conventional cross-sectional imaging modalities such as CT have often been paired with bone scans to improve detection of bone metastases.
The advent of prostate-specific membrane antigen (PSMA)-ligand PET/CT imaging has substantially improved prostate cancer staging [5–7]. Both initial retrospective results and prospective trials have demonstrated the ability of ^68^Ga-PSMA-11 to detect the sites of biochemical recurrence and improve the staging of regional and distant disease in intermediate and high risk primary PCa [8–10]. ^68^Ga-PSMA-11 (gallium Ga-68 gozetotide) has gained US Food and Drug Administration (FDA) approval and its success has led to the incorporation of PSMA-ligand imaging in a variety of national and international practice guidelines [2, 11–14]. These ligands, in addition to the aforementioned ^68^Ga-PSMA-11, include ^68^ Ga-PSMA-I&T, ^18^F-DCPyL, ^18^F-rhPSMA-7.3 and ^18^F-PSMA-1007 [13, 15, 16].
^68^ Ga-PMSA-11 PET/CT outperforms other targeted molecular imaging agents, such as ^18^F choline or fluciclovine, providing improved diagnostic accuracy and resulting in profound changes in patient management [8–10, 17, 18]. Findings from the proPSMA trial demonstrate a clear superiority of ^68^Ga-PSMA-11 compared to cross-sectional imaging and bone scan for the staging of high-risk primary PCa [19].
The German Cancer Consortium (DKTK) started an initiative to evaluate this new imaging agent in a prospective multi-national, multi-center phase 1/2 to evaluate safety and diagnostic efficacy in primary high risk prostate cancer. Within this prospective multicenter study, we aimed to assess the diagnostic accuracy of PSMA-PET/CT including patients with newly diagnosed prostate cancer at high risk for metastases who were scheduled for radical prostatectomy (RP) with extended pelvic lymph node dissection (EPLND). Primary objectives were i. the assessment of ^68^Ga-PSMA-11 PET/CT imaging to detect prostate cancer tissue within the prostate gland and pelvic lymph nodes and ii. to assess the clinical safety of ^68^Ga-PSMA-11.
Secondary objectives included i. the ability of ^68^Ga-PSMA-11 PET imaging to detect bone metastases in comparison to ^99m^Tc bone scintigraphy, ii. to correlate ^68^Ga-PSMA-11 uptake in primary tumours with Gleason Score in post-surgical specimens, iii. to determine the percentage of patients in which pre-operative ^68^Ga-PSMA-11 PET/CT imaging would result in a change in clinical management and iv. to evaluate the impact of pre-operative ^68^Ga-PSMA-11 PET/CT imaging on target volume definition for radiation therapy.
Material and methods
Study design and participants
A prospective open-label, single-arm, rater-blinded, multinational multi-center, diagnostic phase 1/2 study to assess safety and diagnostic performance of ^68^Ga-PSMA-11 PET/CT imaging to detect sites of prostate cancer in patients with newly diagnosed high-risk PCa (NCT03362359) was performed at 9 academic sites in Germany, Austria and Switzerland.
The study protocol was created in accordance with the Declaration of Helsinki and Good Clinical Practice, and all patients gave written informed consent before study entry. The trial was approved by the local institutional review boards, the Federal Office for Radiation Protection (Bundesamt fuer Strahlenschutz) and the Federal Institute for Drugs and Medical Devices (Bundesinstitut für Arzneimittel und Medizinprodukte, BfArM). The study drug, ^68^Ga-PSMA-11, was produced under locally established manufacturing allowances (Herstellungserlaubnis) harmonized between all centers and approved by the respective local governments. The trial was funded by the German Cancer Consortium (DKTK) and the protocol is provided in the appendix 1. Study and data management was conducted by ABX-CRO, Dresden, Germany.
Eligibility criteria included patients with histologically confirmed adenocarcinoma of the prostate, high risk for metastasis (stage cT3, Gleason Score > 7, or PSA > 20 ng/ml), who were scheduled for surgery (radical prostatectomy and extended lymph node dissection). Patients were excluded if they demonstrated hypersensitivity to ^68^Ga-PSMA-11 or its components, had known lymph node metastases outside the surgical field, > 5 bone metastases (based on ^99m^Tc bone scintigraphy), and any previous prostate cancer therapy. Prior to study inclusion a ^99m^Tc-bone scan and cross-sectional (CE-CT or CE-MRI) imaging of abdomen and pelvis were obtained consistent with EAU guidelines [12].
Procedures
Each patient received a single intravenous injection of 150 (± 50) MBq ^68^Ga-PSMA-11 on day 1 followed by PET/CT imaging at 1 h ± 10 min p.i. A low-dose CT was performed for attenuation correction followed by a diagnostic contrast-enhanced CT. PET acquisition time for each bed position was 3–4 min. Details on image acquisition and reconstruction are provided in the subject imaging manual in appendix 2 and supplementary materials*.* Please note that both conventional and digital scanners with and without time-of-flight have been used at the different trial sites. Scanners were EARL certified.
Image interpretation and radiotherapeutic planning
Three independent readers performed a central reading. Each patient scan was evaluated by two independent readers (Reader 1: SS and Reader 2: KR). If the reading results were concordant (i.e. in agreement), this was considered the final reading result. In case of disagreement between the two independent readers, an adjudication reading by a third reader (adjudicator: TD) was performed and became the final reading result (majority vote). All raters were blinded to the results of any histological investigations and preceding imaging (e.g., bone scan, MRI). All readers were experienced on clinical ^68^Ga-PSMA-11 reading and were required to complete training on 12 cases (not part of the present study population). Each reader had to re-assess 10% of the cases for quality assurance purposes.
The following qualitative analyses were performed based on the recently introduced molecular imaging TNM system (miTNM, version 1.0) as a standardized reporting framework for PSMA PET [20]. Tumour involvement of the prostate gland was assessed based on quadrants (right/left, upper/lower part) on the PET/CT image data and was reported on a 3-point scale (positive, equivocal, negative). All pelvic lymph nodes, in eight pre-defined sub-regions, (appendix 2) visible on the PET/CT and diagnostic CT scan were evaluated using a 3-point scale (positive, equivocal, negative). The short axis diameter of each representative lymph node was measured. Quantitative measurement of ^68^Ga-PSMA-11 uptake was performed in the hottest foci of the primary tumor (dominant lesion) using the maximum SUVpeak. Qualitative and quantitative analyses were performed using Mind Lesion (Mind Medical GmbH, Heidelberg).
Fictitious radiotherapy planning delineating target volumes independently based on conventional imaging and ^68^Ga-PSMA-11 PET was performed by experienced radiation oncologists blinded to the histopathological findings (CAG, SAK). Differences in target volume definitions from conventional imaging and PET were determined. SUV-parameters in PSMA-PET imaging for lesion based radiotherapeutic planning and management SUV-parameters were used as recently published [21].
Safety
Physical examination, vital signs, 12-lead ECG, pulse oximetry and laboratory tests (haematology, serum chemistry, urine analysis) were performed before dosing and 1.5 h ± 30 min, 24 h ± 4 h and 7 d after dosing. All adverse events and concomitant medications were recorded until 7 days after dosing. For details, see study flow chart (appendix 1).
Surgery, follow-up, and histopathological correlation
Surgery (radical prostatectomy and extended lymph adenectomy) and analysis of tissue specimens was performed as part of the standard care between day 7 (after EOS visit) and day 60. Only information about PSMA-positive lymph nodes outside the extended pelvic node dissection and any additional bone lesions detected by the local nuclear medicine investigator were conveyed to the surgeon to aid in their treatment planning. EPLND was conducted according to the EAU guideline 2015 with 8 sub-regions (supplementary materials). Tissue from each subregion was separately collected. Tissue specimens obtained from RP with EPLND were analyzed blinded to the results of PET imaging, first by the local pathologists and then transferred for a further second central pathology reading.
Outcomes and variables
Primary endpoints of the study were sensitivity, specificity, positive predictive value (PPV), negative predictive value (NPV), and accuracy of ^68^Ga-PSMA-11 PET to identify tumor tissue in the prostate gland and pelvic lymph nodes using histopathology as the standard of truth. Analyses were performed on a per-patient and per-quadrant basis for lesions in the prostate gland and on a per-patient, per-gross region (pelvic right vs. left) and per-subregion basis for lymph nodes. Safety and tolerability of ^68^Ga-PSMA-11 was assessed in terms of frequency of occurrence and severity of abnormal findings during safety evaluations. Secondary endpoints included detection of bone metastases, quantitative standard uptake values (SUV) stratified by Gleason Score, fraction of patients with change in clinical management and the impact on target volume definition for radiation therapy. In exploratory post-hoc analyses the sensitivity of ^68^Ga-PSMA-11 PET to identify lymph node metastases was stratified by lesion size on histopathology and interobserver variability for ^68^Ga-PSMA-11 PET reporting was investigated.
Histopathological workup
The lymph node specimens were processed by each of the participating pathology departments according to their corresponding routine protocol. A central pathology core unit was established where slices from all participating centers were collected and evaluated. Histological results from the prostate and all lymph node specimens were assessed by the central pathologist (SK) using light microscopy (Leica DM2500®, Wetzlar, Germany) with 2.5x, 10 × and 40 × objectives. The size and extent of metastatic infiltration in each lymph node metastasis were determined and measured manually in two dimensions with an ocular micrometer. The total number of resected lymph nodes, number of metastatic lymph nodes and size of the lymph nodes and metastases were documented for each resected region.
Statistical analysis
Sample size calculation for the study was based on prior experience with patients undergoing primary staging prior to RP [22]. A sensitivity of 75% and a specificity of 96% to detect PCA tissue are expected for ^68^Ga-PSMA-11 imaging. For a sample size of *N = *30 LN positive subjects, a 95% confidence interval (CI) of 0.3 (i.e. 60–90%) can be specified for an expected sensitivity of 75%. To recruit *N = *30 LN positive patients a total sample size of *N = *150 subjects will be needed assuming a prevalence of 20% for lymph node metastases in high risk primary PCa [23]. The resulting 120 subjects without lymph node metastases will allow confirmation of a specificity of about 96%, with a 95% CI of < 0.08 (91–99%).
Outcome parameters were assessed descriptively, separately for primary tumours, and lymph nodes. Regions judged as equivocal on imaging were counted as negative for statistical analysis. Data reported included frequency distribution, mean and 95% CI. CI were calculated using the Wilson score interval method. For the dominant intraprostatic lesion the maximum SUVpeak was compared with the highest Gleason Score. The Kruskal–Wallis test was performed to assess differences across Gleason Scores. In an exploratory post-hoc analysis defined cutoffs between 3 and 5 mm based on tumor diameter on histopathology were used to measure sensitivity of ^68^Ga-PSMA-11 PET/CT to detect lymph node metastases on a per-patient basis. Inter-observer agreement was determined using Brennan/Prediger Kappa (supplementary materials).
Results
A total of 182 patients were screened at 9 centers and 173 patients received the study drug (Supplementary Table 1) between 2017 and 2020. All 173 patients were eligible for assessment of safety and tolerability (safety dataset). 140 patients were eligible for image evaluation but one patient lacked histological samples for central assessment. A total number of 139 datasets were eligible for final analysis of the primary imaging endpoints (imaging dataset). The study CONSORT diagram is presented in Fig. 1. The baseline patient characteristics are provided in Table 1*.*Fig. 1CONSORT diagram. *: start of ADT prior RPE, no DICOM files for bone scan available, otherTable 1Characteristics of all patients who received ^68^Ga-PSMA-11 (safety dataset) and subset of patients with correlation of imaging data to histopathology (imaging dataset)Safety dataset(*N = *173)Imaging dataset(N = 139)Age, years Median Range6645–826645–81Time since prostate biopsy, months Median Range10–810–8Gleason Score biopsy, n (%) 6 7 8 9 103 (1.7%)34 (19.7%)69 (39.9%)63 (36.4%)4 (2.3%)2 (1.4%)25 (18.0%)57 (41.0%)53 (38.1%)2 (1.4%)iPSA, ng/mL Median Range12.20.7–204.311.31.7–204.3^68^Ga-PSMA-11 PET/CT Administered activity, - median (range), MBq152.6 (89.5–226.0)153.9 (89.5–226.0)CT, computed tomography; PET, positron emission tomography; PSA, prostate specific antigen^^ all of these patients were classified as high-risk based on PSA > 20 ng/ml
Primary endpoints
68Ga-PSMA-11 PET imaging to detect prostate cancer tissue within the prostate gland
On a per-patient basis ^68^Ga-PSMA-11 PET/CT was positive by consensus read in 135 patients, resulting in a sensitivity of 0.971 (95% CI, 0.928–0.992). On per-quadrant basis, sensitivity, specificity, PPV, NPV, and accuracy were 0.710 (95% CI 0.670–0.750), 0.600 (95% CI 0.485–0.715), 0.925 (95% CI 0.896–0.952), 0.230 (95% CI 0.196–0.290) and 0.696 (95% CI 0.658–0.734), respectively.
68Ga-PSMA-11 PET imaging to detect pelvic lymph node metastases
Lymph node metastases were present at histology in 55 patients (39.6%) from 103 regions. A total of 268 lymph node metastases were identified pathologically, and 28 metastases were outside the standard EPLND field.
On a per-patient basis sensitivity, specificity, PPV, NPV, and accuracy were 0.400 (95% CI 0.271–0.529), 0.988 (95%CI 0.965–1.000), 0.957 (95% CI 0.873–1.000), 0.716 (95% CI 0.633–0.798) and 0.755 (95% CI 0.684–0.827), respectively. In the exploratory post-hoc analysis, sensitivity was in the range of 0.564 (95% CI 0.396–0.722) for a 3 mm size threshold to 0.690 (95% CI 0.566–0.962) for a 5 mm size threshold of lymph node infiltration (LNI) (Fig. 2). Details on size-stratified PET-diagnostic performance are presented in Supplementary Table 2.Fig. 2. Correlation between lymph node infiltration (LNI) and sensitivity of ^68^Ga-PSMA-11 PET
On a per region hemiplevic (right vs. left pelvis), basis sensitivity, specificity, PPV, NPV, and accuracy were 0.345 (95% CI 0.244–0.447), 0.995 (95% CI 0.985–1.000), 0.967 (95% CI 0.902–1.000), 0.778 (95% CI 0.727–0.830) and 0.799 (95% CI 0.751–0.846), respectively. On a per-region or template basis sensitivity, specificity, PPV, NPV and accuracy were 0.155 (95% CI 0.085–0.225), 0.982 (95% CI 0.973–0.990), 0.471 (95% Ci 0.303–0.638), 0.917 (95% CI 0.900–0.934) and 0.903 (95% CI 0.886–0.921), respectively.
Inter-reader agreement
In the exploratory post-hoc analysis inter-reader agreement for prostate gland evaluation was 0.90 at patient level and 0.59 at quadrant level. For lymph nodes, the agreement was 0.90 at patient level and 0.93 at sub-region level.
Safety evaluation
Overall, 20 treatment-emergent AEs were reported in 14 of 173 (8.1%) patients (Table 2). Treatment-emergent AEs were graded as grade 1 (*n = *19) and grade 2 (*n = *1) and none led to study discontinuation. These events were not considered to be related to the study drug. No severe treatment-emergent AEs were reported. Detailed characteristics of AEs are presented in Supplementary Table 3.Table 2. Summary of adverse eventsInvestigators’ interpretationTotal (*n = *173)(n [%])Total number of TEAEs20Patients with at least one TEAE14 (8.1%)TEAEs leading to death0Total number of SAEs0Treatment-related TEAEs0Patients with at least one treatment-related TEAE0TEAEs leading to discontinuation0Patients with at least one TEAE leading to discontinuation0TEAEs by toxicity grade 119 (95.0%) 21 (5.0%) 3–50
Secondary endpoints
Detection of bone metastases on 68Ga-PSMA-11 PET/CT compared to 99mTc bone scintigraphy
12 patients exhibited positive findings by ^68^Ga-PSMA-11 PET/CT and/or bone scintigraphy in 17 anatomic regions. Only in one patient, both imaging modalities were concordantly positive in the same region. Negative ^68^Ga-PSMA-11 PET/CT with positive bone scintigraphy occurred in 7 patients in 7 different regions. Negative bone scintigraphy in ^68^Ga-PSMA-11 PET/CT positive regions was noted in 4 patients with one region in two patients, two regions in one patient and five regions in one patient. Details on patients reported as having positive bone findings are provided in Supplementary Table 4.
Correlation of 68Ga-PSMA-11 signal with Gleason Score
In 135 of 139 patients, quantitative analyses of ^68^Ga-PSMA-11 uptake in the dominant intraprostatic lesion was performed. Median maximum SUVpeak was 6.4 (range 1.7–13.6), 8.4 (range 2.3–39.4), 10.7 (range 5.6–23.0) and 13.4 (range 3.8–56.9) for Gleason Score 7a, 7b, 8 and 9, respectively. Maximum SUVpeak was significantly different for Gleason Score groups (Kruskal Wallis Test: Chisquare = 21.32, p < 0.001, Fig. 3A). Two patient examples are shown in Fig. 3B.Fig. 3. Correlation between ^68^Ga-PSMA-11 uptake and Gleason Score (A). PET-imaging, gross-section and detailed histopathology H&E histopathology including PSMA-immunhistochemistry (B) of two patients with Gleason Score 7a (upper row) and Gleason Score 9 (lower row)
Fraction of patients with change in clinical management
RP and EPLND were not conducted in a total of 23 patients. Change in clinical management resulted from the presence of unknown metastases first seen on ^68^Ga-PSMA-11 PET/CT precluding the patient from surgery in 11 cases (extensive pelvic lymph node metastases *n = *3; distant lymph node metastases *n = *3; unknown bone metastases *n = *3, pulmonary lesions *n = *2). 5 (21.7%) patients refused surgery, 4 (17.4%) patients received other therapies and 3 patients were lost to follow-up.
Change of (Potential) radiotherapeutic management
Radiotherapeutic planning was conducted in all patients from the imaging dataset. ^68^Ga-PSMA-11 PET resulted in target volume changes in 29 patients out of 139 patients (20.9%): In 23 patients major changes of the radiation plan occurred. This included upstaging to N1-disease, nodes outside international target volume recommendations (RTOG) and downstaging of morphological suspicious findings. In six patients minor changes were implemented in the radiation plan by altering the number of boosts to nodes based on positive findings in ^68^Ga-PSMA-11 PET/CT (Details see Table 3). Two patient examples are presented in Fig. 4 and 5.Table 3. Change of radiotherapeutic managementMajor changes(n = 23 patients)N1 instead of N0n = 12N0 instead of N1n = 7positive node(s) outside RTOG target volume recommendationsn = 5negative node(s) outside RTOG target volume recommendationsn = 5M0 instead of M1an = 1M1a instead of M0n = 1M1b instead of M0n = 2Minor changes(n = 6 patients)additional SIBsn = 5different SIBsn = 1SIB simultaneous integrated boost (for positive nodes)^^for some patients more than one change occurredFig. 4^68^Ga-PSMA-11 PET in a 68 year old patient with a histopathological proven Gleason 8 prostate cancer (iPSA 50 ng/ml). Fused PET/CT and PET-images show intense tracer uptake in the primary tumor (A and B). A paravesical lymph node (arrow) is suspicious on morphological imaging but negative in ^68^Ga-PSMA-11 PET (C and D). CT-guided (E) vs. ^68^Ga-PSMA-11-PET guided (F) radiation therapy planning: extended irradiation due to suspected paravesical node (E) in CT; prostate irradiation only (F)Fig. 5^68^Ga-PSMA-11 PET in a 72 year old patient with a histopathological proven Gleason 7 prostate cancer (iPSA 52 ng/ml). Coronal and sagittal PET MIP-views (A and B) present intense uptake of the tracer in the primary tumor (black arrow) and multiple pelvic areas with ^68^Ga-PSMA-11 uptake indicating lymph node metastases (red arrows). A small sized pararectal lymph node (4 mm in CT, C) show intense ^68^Ga-PSMA-11 uptake (E). CT-guided (D) vs. ^68^Ga-PSMA-11 PET guided (F) radiation therapy planning: irradiation of the pararectal lymph node was not included (C) in CT compared to ^68^Ga-PSMA-11 PET based planning (F)
Discussion
In this multicenter prospective phase 1/2 imaging trial in primary high risk PCa,^68^Ga-PSMA-11 proved to be a safe agent that produced highly impactful results. Using independent central reads ^68^Ga-PSMA-11 PET/CT was positive in 97.1% of primary tumors. Sensitivity and specificity on a per-patient basis for the detection of pelvic nodal metastases validated by histopathology were 40.0% and 98.8%, respectively consistent with the findings of other studies of PSMA PET/CT in similar populations. Adjusted to a threshold of 3 and 5 mm, which is the usually physical resolution of a PET-scanner, sensitivity increased to 56.4% and 82.4%, respectively. Change of clinical management, including surgical and radiation planning was observed in a substantial number of patients. To our knowledge, this study is the largest prospective multinational multi-center study using ^68^Ga-PSMA-11 PET focusing on primary high-risk PCa and using extensive centralized histopathological review with analysis on the basis of nodal templates as well as on the basis of LN lesion size.
The predefined specificity of 96% for lymph node disease was exceeded on a per-patient basis. However, the predefined sensitivity of 75% for detection of lymph node metastases was not reached. In retrospect the sensitivity was overestimated as it was based on older data [22]. Emerging data in the literature in primary PCa suggests a sensitivity for lymph node involvement of approximately 40% against the gold standard of careful histological evaluation, which reflects the much higher sensitivity of histopathology for microscopic and even small macroscopic lymph node involvement [14, 24, 25]. Our study is in line with several retrospective and prospective studies: For instance, Hope et al. conducted a prospective phase 3 trial in patients with intermediate and high-risk prostate cancer and reported a sensitivity of 40.0% for lymph node involvement on PET similar to our results [24]. In the surgery cohort of this study, 225 of 277 patients had high-risk disease. A recent meta-analysis by Petersen et al. summarizing the experience of eighteen retrospective and prospective studies reported a weighted sensitivity of 59% (range 23–100%) [26]. Most of the early studies were characterized by small sample sizes and were conducted as single-center retrospective studies lacking blinded independent central readers with matched histopathologic correlation. Such studies will tend to overestimate performance [27].
A major reason for this lower than expected sensitivity is that lymph node metastases are often microscopic and challenge the physical detection limit of PET technology. When patients with lymph node lesions smaller than 3 mm or 5 mm were removed from the dataset, the patient-based sensitivity rose to 56.4 and 69.0%, respectively. Consequently, the “diagnostic window” to detect lymph node metastases in PET imaging begins with lesions approximately 5 mm which compares very favorably to conventional cross-sectional imaging, for which a size of at least 8–10 mm is needed to identify positive lesions [3, 4, 28]. Even then, conventional cross sectional imaging lacks specificity for lymph node metastases as hyperplastic nodes can lead to false positives. The superiority of ^68^Ga-PSMA-11 PET compared to cross-sectional imaging was also confirmed in the proPSMA trial in which a 32% higher area under the curve (AUC) for detection of lymph node metastases was observed with PET vs. conventional imaging, although histology was not used as a gold standard in that study [19].
In the current study, a limitation of this post-hoc analysis of lymph node lesion size threshold is the decreasing number of patients in each size strata. For instance, at the 5 mm threshold only 29 of 55 patients were evaluable, reducing the statistical power. This is, in part, balanced by the higher prevalence of lymph node metastases in our study compared to the literature-based estimate. The lymph node metastasis rate in this study was 39.6%, approximately double the literature estimate of 20%.
The sensitivity of ^68^Ga-PSMA-11 PET/CT for lymph node metastases is also subject to sampling bias. For instance, if the analysis is conducted on a hemi-pelvic or template-based format, sensitivity falls to 34.5% and 15.5%, respectively, as the number of subregions increases the likelihood of sub-detectable lesions within those subregions and further reducing sensitivity. In addition, especially for template-based analysis, errors can result from mismatches between the nodes labeled during surgery and the central reading. This is reflected in the higher number of false positive lesions using the template-based analysis indicated by a drop in PPV from 71.6% in the patient-based analysis to 47.1% in the template-based analysis. From a practical point of view, the patient-based analysis is most useful to the clinician as it determines N-status. However, the template-based analysis heightens awareness of the high likelihood of sub-detectable lymph node metastases even in a high-risk population. The clinical implications in terms of overall survival of sub-detectable lymph node metastases needs to be established in larger prospective studies.
While false negative lymph node findings are a recognized limitation of ^68^Ga-PSMA-11 PET/CT, false positives were relatively unusual, suggesting that a positive scan can be relied upon as an indicator of advanced disease in most cases. ^68^Ga-PSMA-11 uptake was seen in nearly all (97.1%) of primary prostate tumors. These data confirm prior retrospective evidence and indicates ^68^Ga-PSMA-11 PET/CT can be considered a non-invasive imaging biomarker similar in accuracy to immunohistochemistry [22, 29, 30]. High ^68^Ga-PSMA-11 uptake in high-risk prostate cancer is significantly correlated with Gleason Score but shows high inter-patient variability. Thus, it cannot replace Gleason scoring but may indicate the inherent biologic variability within each Gleason score stratum and suggests added potential clinical value for lesion characterization, prognostication and targeted biopsy/treatment [21, 31].
While ^68^Ga-PSMA-11 PET/CT was highly accurate on a per-patient basis, at a more granular level of analysis, mismatches between PET and histology became more clear. Potential reasons include misregistration between imaging and histopathology, small volume disease undetectable by PET, and known physiological background uptake of ^68^Ga-PSMA-11, especially in the central-zone of the prostate gland [32]. Similar to prior retrospective and prospective investigation inter-reader agreement was substantial (> 0.6) for local and nodal reads, confirming the high reproducibility of ^68^Ga-PSMA-11 PET imaging and differentiating it from prostate MRI where inter-reader agreement is substantially lower [10, 24, 33].
Although limited by sample size, the correlation of the ^68^Ga-PSMA-11 PET/CT findings with bone scintigraphy were surprisingly poor. It should be noted that patients with extensive bony metastases (> 5 lesions) were excluded from the study. Thus, in this select group of patients with a small number of bone lesions, most regions with positive signals on bone scintigraphy were negative on ^68^Ga-PSMA-11 PET/CT, while regions positive on PET/CT were often negative on bone scintigraphy. Lacking a definitive standard of reference, it is impossible to compare the accuracy of the two methods. However, retrospective data and especially prospective data from the ProPSMA trial have shown that positive findings on ^68^Ga-PSMA-11 PET/CT are reliable indicator of bone metastases whereas lesions seen only on bone scintigraphy have a high false positive rate [19, 34, 35].
The clinical impact of ^68^Ga-PSMA-11 PET/CT is clearly demonstrated in this study. Planned surgery was not performed in 23 patients (13.2%). In 11 of 23 extra-prostatic disease was depicted on PSMA PET/CT. Similarly, there was a substantial impact on radiotherapeutic management. In 29 of 139 (20.9%) of patients, changes in the radiation plan including alterations in the sites of boosts occurred. Of note, 28 metastases on ^68^Ga-PSMA-11 PET/CT were disclosed outside the standard intrapelvic lymph node templates, emphasizing the importance of pre-therapeutic imaging for both surgery and radiation therapy planning. Our results are similar to the proPSMA study in which changes in patient management were reported in 17.7% of high-risk patients [19].
Our study has a number of limitations. While sensitivity was high on a per-patient basis, mapping of intra-prostatic cancer to histologic specimens could not be reported on an octant basis as intended due to challenges of co-registering imaging and surgical specimens. Additionally, routine PSMA-immunohistochemistry was not part of the study but could provide further information on the extent to which lesional PSMA-expression contributes to the lack of detection. For similar reasons, mismatches between (mainly adjacent) histologically positive lymph nodes and their location on PET/CT are difficult to avoid. In addition, PSMA-positive nodes in other than the eight pelvic templates have been noted by the independent blinded readers but have not been part of the primary endpoint for the template-based analysis. A standard of reference for assessing bone lesions was not implemented, and that combined with study-defined exclusions of patients with bone disease, limited the interpretation of bone findings in the study. Finally, this manuscript does not report results on the analysis of molecular and clinical biomarkers (exploratory secondary endpoint) but will be the subject of future investigation.
Conclusion
^68^Ga-PSMA-11 is a safe radiopharmaceutical and, in the setting of primary staging of high-risk prostate cancer patients, leads to increased diagnostic accuracy with a high impact on clinical management. Furthermore, pre-operative ^68^Ga-PSMA-11 PET/CT will inform accurate patient counselling by identifying PSMA-positive disease outside the planned surgical or radiotherapy field which could result in better clinical outcomes.
Supplementary Information
Below is the link to the electronic supplementary material.Supplementary file1 (DOCX 26 KB)Supplementary file2 (DOCX 20.5 KB)Supplementary file3 (XLSX 10.3 KB)
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1National Comprehensive Cancer Network (NCCN). Prostate cancer (Version 3.2024). 2024. https://pubmed.ncbi.nlm.nih.gov/38626801/
- 2FDA. FDA Approves First PSMA-Targeted PET Imaging Drug for Men with Prostate Cancer. 2020. https://www.fda.gov/drugs/news-events-human-drugs/fda-approves-second-psma-targeted-pet-imaging-drug-men-prostate-cancer
- 3EAU Guidelines on Prostate Cancer. Edn. presented at the EAU Annual Congress Milan. 2023. https://pubmed.ncbi.nlm.nih.gov/38614820/