Telehealth utilization during the COVID-19 pandemic: comparing breast cancer survivors to non-cancer patients and implications for current practice
Lashez A. Hawkins, Ruvarashe P. Rumano, Sharnell S. Smith, Chloe M. Beverly-Hery, James L. Fisher, Akia Clark, Victoria Champion, Bridget A. Oppong, Electra D. Paskett

TL;DR
Breast cancer survivors used telehealth less during the pandemic compared to non-cancer patients, despite its benefits, suggesting a need to address barriers to adoption.
Contribution
This study identifies demographic and clinical factors influencing telehealth use among breast cancer survivors during the pandemic.
Findings
Breast cancer survivors had significantly lower telehealth use (41.5%) compared to non-cancer patients (63.9%).
Higher education and being married were associated with increased telehealth use.
Among breast cancer patients, higher education and recent surgery were linked to decreased telehealth participation.
Abstract
During the 2019 coronavirus (COVID-19) pandemic, in-person medical visits changed due to social distancing guidelines. Breast cancer (BC) patients, needing ongoing treatment or surveillance, faced increased challenges in accessing care. Telehealth became essential for providing convenient and cost-effective care while minimizing COVID-19 transmission. BC survivors, however, often value in-person visits for clinical exams. This study aimed to compare telehealth participation between patients with a history of BC and women without cancer history. Adults aged 18 and older, including cancer patients, survivors, caregivers, and healthy volunteers, primarily from Ohio, were recruited with attention and inclusion of underserved and minority populations to complete a survey about COVID-19-related beliefs, practices, and knowledge. Recruitment involved (1) re-contacting participants from…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
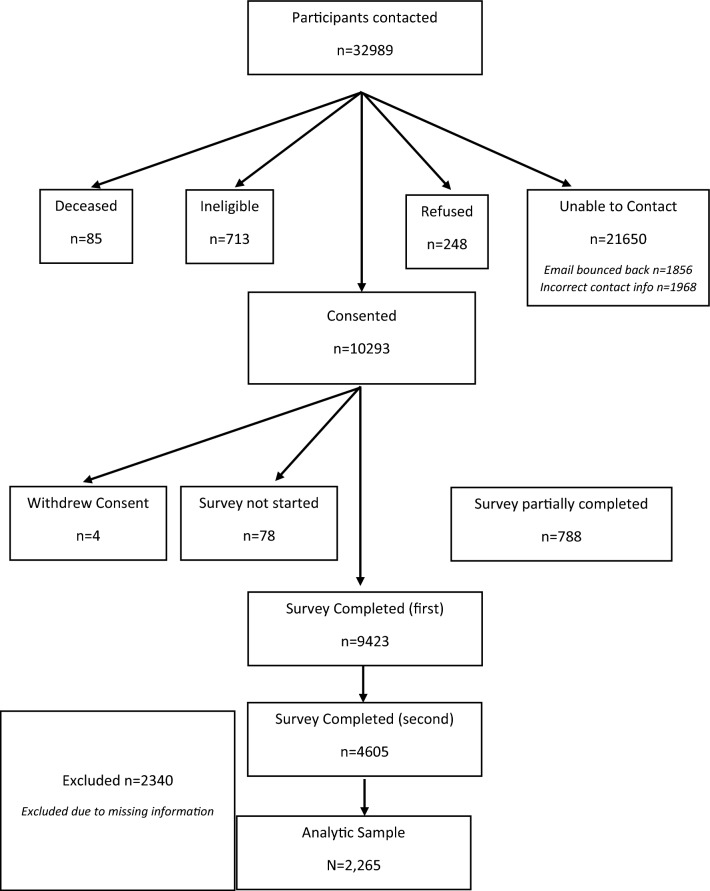 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsTelemedicine and Telehealth Implementation · COVID-19 and healthcare impacts · Cancer survivorship and care
Introduction
In the United States, breast cancer (BC) is the most commonly diagnosed cancer in women, with an estimated 310,720 new invasive cases and 42,250 deaths in 2024, corresponding to an incidence of about 131 and a mortality of 19 per 100,000 women [1]. In Ohio, approximately 10,071 new breast cancer cases and 1698 deaths occur annually [1]. The coronavirus (COVID-19) pandemic prompted a paradigm shift in healthcare delivery, aiming to maintain essential care while minimizing viral transmission. Since 2020, the United States has reported over 100 million COVID-19 cases and more than 1.1 million deaths, including roughly 3.7 million cases and 43,896 deaths in Ohio [1]. Early in the pandemic, declines were observed across the breast cancer care continuum—including screening, diagnosis, treatment, and surveillance—disrupting control efforts and potentially impacting breast cancer-related mortality [2]. To mitigate transmission risks, healthcare systems rapidly transitioned from in-person visits to widespread telehealth adoption—embraced by diverse patient populations across both oncology and non-cancer outpatient care. [3–5] Telehealth, delivered via phone or Internet-based platforms, encompasses a broad range of clinical and non-clinical services, including consultations, diagnosis, health education, remote monitoring, and administrative functions [6]. These services are enabled by information and communication technologies (ICT), such as video conferencing, mobile applications, and secure messaging [6]. Although telemedicine existed prior to the pandemic, its use and scholarly evaluation remained limited until COVID-19 accelerated both [7]. The expansion of telehealth aimed to enhance patient and provider safety, reduce travel and wait times, improve convenience, and support continuity of care, benefits that remain relevant in the post-pandemic landscape. Telehealth may also mitigate time toxicity, the cumulative burden of time spent on in-person visits, travel, and care coordination, which is increasingly recognized as a critical factor in patient-centered cancer care [8–10].
Concerns have been raised about telehealth acceptance among patients with a history of BC. Several studies found that many patients preferred in-person visits focused on BC treatment (including surgical management and preparation as well as broader treatment options such as radiation, chemotherapy, targeted therapy, and immunotherapy), valuing face-to-face interactions—particularly for important discussions and breast exams—which offered greater comfort and a stronger personal connection with their providers [3]. Numerous studies have explored the efficacy of telehealth and the satisfaction levels of patients with a history of BC amidst the COVID-19 pandemic [3, 4]. While active treatments such as surgery, chemotherapy, and radiation therapy required in-person visits, survivorship follow-ups and supportive care programs emerged as ideal candidates for virtual delivery. A retrospective study examined the utilization of BC survivorship services during the pandemic [11, 12]. The survivorship programs (SPs) were virtual and provided clinical and non-clinical programming such as physical rehabilitation, emotional and psychosocial support, nutrition, and exercise programming. The most significant shift in participation rates among non-clinical SPs during the pandemic was observed in the utilization of exercise content, which surged by 220% from 2019 to 2020 [11, 12]. Another descriptive study of breast cancer survivors (stage 0–III) found high satisfaction and strong information recall after nurse practitioner led telehealth SCP visits, indicating the potential of telehealth to support survivorship care delivery [13].
The current study aims to enhance comprehension regarding the sociodemographic and clinical factors related to utilization of telehealth services among female BC survivors, compared to those without a history of cancer, during the COVID-19 pandemic.
Methods
Overview
This study was part of an NCI-funded initiative conducted in conjunction with 16 other NCI-designated Cancer Centers, the IC-4 (Impact of COVID-19 on the Cancer Continuum Consortium) [14]. The initiative was funded to work collectively to develop core survey items and implement population surveys in the respective catchment areas. The overall goal of the IC-4 was to assess how differences in demographics (rural/urban residence, age, gender, race, educational attainment) impact engagement in cancer preventive behaviors (e.g., tobacco cessation, screening, diet) and cancer management/survivorship behaviors (e.g., adherence to treatment, adherence to surveillance, access to health services) in the context of COVID-19 environmental constraints (e.g., social distancing, employment, mental health). Each site had its own theoretical framework and survey methods. Our site used the IC-4 core set of common data elements, augmented with questions of interest to the local team, with remote data collection methods to include many unique and diverse populations. This study was approved by the OSU Institutional Review Board in June 2020.
Theoretical framework
This study was grounded in the Health Belief Model (HBM). According to the HBM, individuals’ change in health behaviors depends on a series of health beliefs, include individuals’: (1) perceived susceptibility to COVID-19 exposure, (2) perceived severity of the consequences of contracting COVID-19 (e.g., hospitalization or death), (3) perceived benefits of the effectiveness of the proposed COVID-19 prevention measures, (4) perceived barriers to executing the proposed prevention measures, (5) cue to the proposed prevention actions, and (6) self-efficacy in the person's ability successfully perform COVID-19 prevention measures [15].
Survey development
The survey elements (See Online Appendix 1) were finalized in conjunction with other members of the IC-4. The survey included individual behaviors related to mitigation of COVID-19 transmission, the challenges related to social distancing, self/family isolation, stress, and health behaviors that are highly relevant to cancer and other chronic diseases (i.e., type, duration and location of physical activity, tobacco/marijuana or alcohol use, vaping/e-cigarette use, exposure to second hand smoke, nutrition/diet, health information-seeking and participation in clinical trials, and access to health services). Questions also assessed perceived stigma related to COVID-19 with respect to different population groups and variables, such as health literacy and mental health, suspected of moderating these influences. Moreover, we assessed the impact of children being out of school and employment challenges (i.e., remote working and unemployment etc.), as well as the influence of social media on information, knowledge, behaviors, and attitudes (See Fig. 1).Fig. 1COVID-19 Survey recruitment flow chart
Sample selection
Participants who agreed to be re-contacted from previous studies were asked to participate in this study with a wide variety of populations, including patients with and without a history of cancer. Eligible participants were adults aged 18 years or older who consented to take part in the study. To ensure the inclusion of the most vulnerable, underserved, and minority populations, we sought to recruit healthy adult volunteers, cancer patients, cancer survivors, and cancer patients and caregivers, mainly from Ohio, with some from Indiana and other states. This was achieved by employing two recruitment strategies. First, we identified and contacted individuals who previously participated in studies conducted at OSU and consented to being contacted for future research projects. In addition, we invited cancer patients and survivors to nominate their primary caregivers to participate in the study. The list of previous research projects conducted at OSU included the Rural Interventions for Screening Effectiveness (RISE) study (R01 CA196243), the Community Initiative Towards Improving Equity and Health Status (CITIES) cohort (Supplement to P30CA016058), the Ohio State University Center of Excellence in Regulatory Tobacco Science (CERTS) cohort (P50CA180908), and members of the Total Cancer Care (TCC) cohort (P30CA016058). Second, to further enhance the representative of our study sample and ensure the inclusion of minority and underserved communities, we utilized our community partners and listservs to send tailored email invitations. Although our recruitment pool included adults with and without a history of cancer, the analysis focuses specifically on female BC survivors and a comparison group without a cancer history, consistent with the study aim.
Interview/data collection
We utilized several data collection methods, including Web, phone, and mailed surveys. Respondents with valid emails received an initial survey invitation via email along with three reminders seven days apart. The first survey was completed from June to November 2020, then the second from March to July 2020. All participants were initially screened using an eligibility form to confirm their current Ohio or Indiana residence before conducting the survey. Participants were able to save the Web survey and resume it at a later time. Those who partially completed the Web survey received an email reminder one week after they last accessed the survey. A trained interviewer contacted participants without an email address and those with invalid emails on file by phone. Participants who were initially reached by phone were offered the option to complete the survey over the phone or online. We mailed a cover letter and a paper survey with a self-addressed, stamped return envelope to participants who requested a mailed survey. For non-English-speaking participants, a bilingual staff member administered the survey in the appropriate language (e.g., Spanish). Participants were offered a $10 gift card upon completion of the survey. All data were collected and managed using the Research Electronic Data Capture (REDCap) secure Web-based application hosted at OSU.
Measures
To evaluate the impact of BC survivorship on health beliefs, behaviors, and telehealth utilization, we evaluated the following variables: age, race, education, income level, marital status, health insurance type, geographic residence (rural vs. urban), health and medical care, cancer history, BC history, and telehealth usage. Race was categorized as follows: “White,” “Black or African American,” “American Indian or Alaskan Native,” “Asian or Asian American,” “Native Hawaiian or Pacific Islander,” and “other.” Education level was listed as follows: “High School or Less,” “Some College/Associate,” “BS/BA,” “MS/MA or More,” and “Missing/Refused/Don’t Know,” based on original responses such as “Less than high school,” “Some high school, no diploma,” “GED,” “High school graduate,” “Some college but no degree,” various associate degrees, bachelor’s degrees, master’s degrees, professional degrees, and doctorates. Income-level amounts were “ < 35 K–50 K–75 K + .” Marital status was determined by the following selections: “Single, never been married,” “Married,” “Not married but living together,” “Separated,” “Divorced,” “Widowed,” or “Other.” Health insurance types were “Medicaid,” “Private health insurance,” “Medicare,” “Medicare plus a supplemental policy,” and “Military/ VA.” Responses were grouped into “no insurance,” “private,” “private and public,” and “public insurance.”
Health and medical care data were assessed by asking participants if they had postponed or skipped a healthcare visit, and status of various health related visits (for example, screening, chronic illness, new/changing health concern, urgent care, or other) due to COVID-19.
Data related to the pandemic was recorded using several questions. Participants were asked if a doctor had ever diagnosed them with cancer. Those who indicated “yes” to a history of cancer were asked additional questions about their active cancer-related treatment during COVID-19 (i.e., surgery and radiation status). Further information was gathered on their diagnosis from medical record review. BC-related variables that are included in this analysis consisted of the following: years since BC diagnosis, SEER stage, and treatment related variables (surgery and radiation).
Telehealth usage was measured by asking the participants if they had completed a telehealth visit since the pandemic. If they answered “yes,” participants were asked to specify if it was by phone or video. Additional variables related to telehealth usage were also included, such as access to Internet, confidence while using devices, and participation in telehealth before the COVID-19 pandemic.
Data analysis
Demographic and clinical factors were summarized according to utilization of telehealth services using descriptive statistics, with frequencies and percentages for categorical variables (e.g., race) and means and standard errors for continuous variables (e.g., age). Differences between those who utilized telehealth services and those who did not were calculated using Chi square tests (Fisher’s exact test, when appropriate). Univariable logistic regressions were used to calculate odds ratios reflecting differences in odds of telehealth utilization among BC survivors (compared to those not previously diagnosed with any cancer) and for categories of potentially confounding factors. Multivariable logistic regression was used to develop a model identifying factors which were at least marginally significantly associated with telehealth utilization, after adjustment for confounding by additional factors in the model. These factors, identified from responses to the COVID-19 survey due to their potential impact on telehealth utilization, were included in the multivariable model (Table 1) to assess their independent associations with telehealth use. Factors with at least marginally statistically significant (p < 0.15) associations in univariate analyses were initially included in the multivariable model. Factors were removed individually, first with the weakest factor, until all factors remaining in the model were significantly associated with telehealth utilization or were important to the model in such a way as to substantively alter association(s) between additional factor(s) in the model and telehealth utilization by 15% or more. Therefore, the final model contained factors that were independently associated with telehealth utilization or important confounders of associations with additional model factors. A subgroup analysis of only those reporting a history of BC was conducted with univariable and multivariable logistic regression for factors associated with telehealth participation. All statistical analyses were conducted using IBM SPSS Statistics version 29.0.1.0 (IBM Corp, Armonk, NY). A two-sided p-value of less than 0.05 was considered statistically significant.Table 1. Odds ratios and 95% confidence intervals from a multivariable logistic regression reflecting associations between odds of having ever participated in a telehealth visit since the COVID-19 pandemic and selected factorsOdds ratio95% CIp-valueRace White (referent)/// Black/African American1.901.04–3.470.036 Asian0.550.24–1.270.162 Other/multiple0.680.36–1.310.251 Missing/refused/don’t know1.210.28–5.300.803Education High school or less (referent)/// Some college/associate1.501.03–2.170.034 BS/BA1.250.86–1.800.247 MS/MA or more1.310.90–1.900.166 Missing/refused/don’t know7.500.17–333.30.299Marital status Single/never married (referent)/// Married/living as married1.611.13–2.310.009 Div/Wid/Sep/Other1.400.91–2.130.129 Missing/refused/don’t know0.880.05–14.50.929Breast cancer diagnosis No (referent)/// Yes0.720.55–0.960.023Vehicle access No (referent)/// Yes0.940.02–0.41.002 Missing/refused/don’t knowNot estimableCurrently working? No (referent)/// Yes1.251.00–1.560.050 Missing/refused/don’t know0.750.20–2.880.679Postponed/skipped any healthcare in past year due to COVID No (referent)/// Yes2.341.84–2.99 < .001 Missing/refused/don’t know0.170.01–2.840.219Confidence level using computers,smartphones, devices Not at all (referent)/// Only a little0.180.05–0.740.017 Somewhat0.290.06–1.090.067 Very0.430.12–1.590.206 Missing/refused/don’t knowNot estimablePre-COVID Telehealth Visit? No (referent)/// By phone only0.530.35–0.800.003 By video only0.710.44–1.140.152 By phone and video0.490.29–0.820.007 Missing/refused/don’t know0.250.01–6.930.416
Results
Demographic characteristics of our sample (N = 2265) according to BC diagnosis versus no diagnosis of cancer at any site are described in Table 2. Of the 2265 participants, 989 (43.7%) had a previous BC diagnosis and 1276 (56.3%) did not have a history of any cancer. Age, education, marital status, and insurance status differed significantly between the groups. Participants with BC were more likely to be among ages 50–59 years old compared to those without a cancer diagnosis (31.6% vs. 26.4%, p < 0.0001). Also, participants with BC were more likely to have a higher level of education compared to those without cancer (BS/BA: 32.0% vs. 27.1%, p = 0.001). Additionally, participants with BC compared to those with no cancer diagnosis were significantly more likely to be divorced/widowed/separated/other (19.3% vs. 15.6%, p = 0.037). Participants with BC were also more likely to have private insurance (67.2% vs. 56.8%, p = 0.001) compared to those with no cancer diagnosis.Table 2a Participant demographics according to breast cancer diagnosis. b Telehealth visit since pandemic according to breast cancer diagnosisBreast cancer diagnosis (N = 989, 43.7%)No cancer diagnosis (N = 1276, 56.3%)p-valueaAge mean (standard error)55.58 (0.40)57.90 (0.35) < 0.001Age group < 40122 (12.3%)127 (10.0%) 40–49142 (14.4%)169 (13.2%) 50–59313 (31.6%)337 (26.4%) 60–69300 (30.3%)414 (32.4%) 70 + 112 (11.3%)229 (17.9%)Race.262 White890 (90.0%)1151 (90.2%) Black/African American42 (4.2%)68 (5.3%) Asian16 (1.6%)22 (1.7%) Other/multiple31 (3.1%)29 (2.3%) Missing/refused/don’t know10 (1.0%)6 (0.5%)Hispanic Ethnicity.065 No957 (96.8%)1251 (98.0%) Yes22 (2.2%)21 (1.6%) Missing/refused/don’t know10 (1.0%)4 (0.3%)Education < .001 High school or less78 (7.9%)161 (12.6%) Some college/associate279 (28.2%)424 (33.2%) BS/BA316 (32.0%)346 (27.1%) MS/MA or more309 (31.2%)343 (26.9%) Missing/refused/don’t know7 (0.7%)2 (0.2%)Income group.235 < 35 K-50 K-75 K + 536 (54.2%)646 (50.6%) Missing/refused/don’t know123 (12.4%)190 (14.9%)Marital status.037 Single/never married94 (9.5%)120 (9.4%) Married/living as married700 (70.8%)956 (74.9%) Div/Wid/Sep/Other191 (19.3%)199 (15.6%) Missing/refused/don’t know4 (0.4%)1 (0.1%)Insurance status < .001No insurance24 (2.4%)21 (1.6%)Public only83 (8.4%)130 (10.2%)Private only665 (67.2%)725 (56.8%)Public and private208 (21.0%)385 (30.2%)Missing/refused/don’t know9 (0.9%)15 (1.2%)Rural urban continuum code.137Non-metro352 (35.6%)501 (39.3%)Metro635 (64.2%)770 (60.3%)Missing2 (0.2%)5 (0.4%)bTelehealth visit since pandemic < .001 No579 (58.5%)460 (36.1%) Yes410 (41.5%)816 (63.9%) By Phone229 (23.2%)463 (36.3%) By Video299 (30.2%)622 (48.7%)^*^Overlapping counts
BC status with regard to any telehealth participation during the COVID-19 pandemic is described in Table 2B. Of these participants with BC, 410 (41.5%) participated in a telehealth visit since the pandemic and 579 (58.5%) did not. Of those BC participants who did participate in telehealth, 229 (55.9%) participants accessed their telehealth visit by phone and 299 (72.9%) accessed by video. In addition, having a telehealth visit since the pandemic was lower among BC survivors compared to those without any cancer diagnosis (41.5% vs. 63.9%, p < 0.001).
Characteristics of our sample according to participation in telehealth visits since the COVID-19 pandemic are described in Table 3. Of these participants, 1226 (54.1%) participated in a telehealth visit since the pandemic and 1039 (45.9%) did not. There was a significant difference in age, with a mean of 55.90 years for those who participated in a telehealth visit, compared to mean of 57.72 years for those who did not (p < 0.001). The groups also differed between self-reported racial categories. Those who participated in telehealth compared to those who did not use telehealth were more likely to be Black/African American (5.8% vs. 3.8%, p = 0.02). Additionally, when analyzing the entire sample (Table 3), a higher percentage of those who used telehealth compared to no telehealth did not have a cancer diagnosis (66.6% vs. 44.3%, p < 0.001).Table 3. Participant demographics according to having ever participated in a telehealth visit since the COVID-19 pandemicParticipated in a telehealth visit since pandemic (N = 1226, 54.1%)Not participated in a telehealth visit since pandemic (N = 1039, 45.9%)p-valueAge mean (standard error)55.90 (0.40)57.72 (0.35) < 0.001Age group.010 < 40120 (9.8%)129 (12.4%) 40–49152 (12.4%)159 (15.3%) 50–59352 (28.7%)298 (28.7%) 60–69395 (32.2%)319 (30.7%) 70 + 207 (16.9%)134 (12.9%)Race.020 White1107 (90.3%)934 (89.9%) Black/African American71 (5.8%)39 (3.8%) Asian15 (1.2%)23 (2.2%) Other/multiple26 (2.1%)34 (3.3%) Missing/refused/don’t know7 (0.6%)9 (0.9%)Hispanic ethnicity.099 No1203 (98.1%)1005 (96.7%) Yes18 (1.5%)25 (2.4%) Missing/refused/don’t know5 (0.4%)9 (0.9%)Education.315 High school or less137 (11.2%)102 (9.8%) Some college/associate396 (32.3%)307 (29.5%) BS/BA345 (28.1%)317 (30.5%) MS/MA or more342 (27.9%)310 (29.8%) Missing/refused/don’t know6 (0.5%)3 (0.3%) Income group.142 < 35 K-50 K-75 K + 630 (51.4%)552 (53.1%) Missing/refused/don’t know174 (14.2%)139 (13.4%)Marital status.473 Single/never married115 (9.4%)99 (9.5%) Married/living as married883 (72.0%)773 (74.4%) Div/Wid/Sep/Other225 (18.4%)165 (15.9%) Missing/refused/don’t know3 (0.2%)2 (0.2%)Insurance status.293 No insurance23 (1.9%)22 (2.1%) Public only129 (10.5%)84 (8.1%) Private only734 (59.9%)656 (63.1%) Public and private327 (26.7%)266 (25.6%) Missing/refused/don’t know13 (1.1%)11 (1.1%)Rural urban continuum code.760 Non-Metro467 (38.1%)386 (37.2%) Metro756 (61.7%)649 (62.5%) Missing3 (0.2%)4 (0.4%)Breast cancer diagnosis < .001 No816 (66.6%)460 (44.3%) Yes410 (33.4%)579 (55.7%)
Results from univariable logistic regression analysis are presented in Table 4. Women with a BC diagnosis were less likely to use telehealth compared to those without a history of cancer (OR: 0.40, 95% CI: 0.34–0.47, p < 0.001). Women aged 70 and older had higher odds of a telehealth visit compared to those under 40 years (OR:1.67, 95% CI: 1.19–2.31, p = 0.003). Compared with white women, odds of a telehealth visit were significantly higher among Black women (OR: 1.54, 95% CI: 1.03–2.29, p = 0.036). There was no significant difference in the use of telehealth by ethnicity. Compared to individuals earning < 50,000–74,999 (OR: 0.65, 95% CI: 0.47–0.92, p = 0.014) and 35 K (referent)/// 49,9990.730.49–1.090.120 74,9990.650.47–0.920.014 $75 K + 0.710.53–0.960.024 Missing/refused/don’t know0.780.55–1.110.170Marital status Single/never married (referent)/// Married/living as married0.980.74–1.310.908 Div/Wid/Sep/Other1.170.84–1.640.349 Missing/refused/don’t know1.290.21–7.890.782Insurance status No insurance (referent)/// Public only1.470.77–2.800.243 Private only1.070.59–1.940.823 Public and private1.180.64–2.160.601 Missing/refused/don’t know1.130.42–3.050.809Rural urban continuum code Non-metro (referent)/// Metro0.960.81–1.140.664 Missing0.620.14–2.790.533Vehicle access No (referent)/// Yes0.130.03–0.54.005 Missing/refused/don’t know.001.000-.006 < .001Days typically left home for work in past 3 weeks No/// Yes0.920.77–1.100.351 Missing/refused/don’t know0.720.22–2.360.584Postponed/skipped any healthcare in past year due to COVID No (referent)/// Yes0.590.49-.0.71 < .00.1 Missing/refused/don’t know1.190.93–1.530.174Internet access at home No (referent)/// Yes0.770.39–1.540.461 Missing/refused/don’t know1.190.58–2.430.640Reliable telephone connection at home No (referent)/// Yes0.510.27–0.950.033 Missing/refused/don’t know0.810.42–1.550.524Confidence level using computers, smartphones, devices Not at All (referent)/// Only a little0.410.12–1.360.144 Somewhat0.560.78–1.740.313 Very0.310.99–0.950.041 Missing/refused/don’t know0.580.18–1.820.347Pre-COVID telehealth visit? No (referent)/// By phone only1.300.90–1.890.168 By video only1.641.07–2.540.024 By phone and video1.250.78–2.020.353 Missing/refused/don’t know1.611.27–2.04 < .001
The factors of interest included race, age, marital status, breast cancer diagnosis, current employment status, whether the participant postponed or skipped any healthcare in the past year due to COVID-19, confidence in using computers, smartphones, and other devices, and whether the participant had a telehealth visit prior to the COVID-19 pandemic. History of BC was associated with reduced odds of telehealth use (OR: 0.72, 95% CI: 0.55–0.96, p = 0.023). Other factors that were significantly associated with increased utilization of telehealth were Black race (OR: 1.90, 95% CI: 1.04–3.47, p = 0.036), having some college education (OR: 1.50, 95% CI:1.03–2.17, p = 0.034), being married (OR: 1.61, 95% CI: 1.13–2.31, p = 0.009), and being currently employed (OR: 1.25, 95% CI:1.00–1.56, p = 0.050). Also, those who postponed or skipped any healthcare visits due to the pandemic had an increased odds of participating in telehealth (OR: 2.34, 95% CI: 1.84–2.99, p < 0.001). Other factors that lowered odds of having a telehealth visit include having a vehicle, having “only a little” confidence with technology, or ever using telehealth prior to the COVID-19 pandemic.
Of the 989 patients with a history of BC, 645 patients had complete data on clinical factors (including SEER stage, surgery status, and radiation status) for the subgroup analysis. More than half of these patients used telehealth during the pandemic, with video visits slightly more common than phone visits. Specifically, 410 patients (64%) participated in at least one telehealth visit, and 73% of those used video. Age greater than 70 years (OR: 2.39, 95% CI: 1.13–5.08) increased telehealth participation. Higher educational attainment (OR: 0.37, 95% CI: 0.19–0.71) and surgical intervention (OR: 0.26, 95% CI: 0.07–0.91) were associated with decreased telehealth participation (Table 5).Table 5. Frequencies, odds ratios, and 95% confidence intervals from univariable and multivariable logistic regressions reflecting associations between odds of having ever participated in a telehealth visit since the COVID-19 pandemic and selected factors among 645 female breast cancer participants of the ‘Impact of COVID-19’ StudyFrequencyUnivariableMultivariableOR (95% CI)OR (95% CI)Age group < 40 (referent)71// 40–49990.78 (0.42–1.45)0.72 (0.38–1.32) 50–591941.01 (0.58–1.76)0.97 (0.54–1.76) 60–692041.25 (0.71–2.18)1.29 (0.72–2.33) 70 + 772.48 (1.20–5.14)2.39 (1.13–5.08)Race White (referent)584/ Black/African American301.38 (0.62–3.07) Asian and other/multiple241.18 (0.50–2.81)Hispanic ethnicity Non-hispanic (referent)629 Hispanic100.57 (0.16–1.99)Education High school or less (referent)57// Some college/associate1861.12 (0.58–2.18)1.07 (0.55–2.11) BS/BA2020.63 (0.33–1.21)0.61 (0.32–1.19) MS/MA or more1960.42 (0.22–0.81)0.37 (0.19–0.71)Income group < 35 K-50 K-75 K + 3440.53 (0.27–1.02)Marital status Single/never married (referent)63/ Married/living as married4411.43 (0.84–2.43) Divorced/widowed/separated/other1382.02 (1.09–3.73)Insurance status No Insurance (referent)14/ Public only590.84 (0.23–3.03) Private only4280.60 (0.18–1.93) Public and private1371.08 (0.32–3.66)Rural urban continuum code Non-metro (referent)238// Metro4071.10 (0.80–1.53)1.43 (0.98–2.09)Currently working No (referent)235/ Yes2680.84 (0.58–1.21)SEER summary stage at diagnosis In situ (referent)61/ Localized2491.21 (0.68–2.49) Regional1311.12 (0.60–2.10) Distant123.24 (0.65–16.11)Had surgery? No (referent)21// Yes6200.28 (0.08–0.96)0.26 (0.07–0.91)Had radiation? No (referent)245/ Yes3951.13 (0.82–1.58)^^ Frequencies may not total to 645 due to missing values
Discussion
The aim of this study was to understand the factors associated with telehealth usage among patients with a history of BC. We compared the usage of telehealth among BC survivors compared to those without cancer during the COVID-19 pandemic. We found that Black race, having some college education, being married, and being currently employed were characteristics significantly associated with increased participation. We subsequently evaluated the differences in telehealth participation among patients with a history of BC showing no differences in telehealth usage based on race, ethnicity, or income. Additionally, an important unique finding was the increased telehealth adoption among individuals over age 70, a demographic typically among the least likely to use the Internet. This trend may reflect the heightened awareness of COVID-19 risks for older adults, who were widely recognized as being at highest risk for severe outcomes, and the widespread public messaging encouraging them to limit in-person visits. Our findings are notable in terms of race, as many studies have demonstrated a lack of telehealth usage from vulnerable patient populations such as African Americans and Hispanics [16–19]. Similarly, a 2023 study reported factors that impact telehealth usage included age, gender, race, education, employment status, and income [17]. Their findings showed that while low-income, racial, and ethnic minority communities were at greater risk for health inequities, Hispanic communities were more likely to use telehealth than other ethnic groups in this study [17]. While our study primarily focused on Black/African American participants, we observed that Hispanic and Asian participants also demonstrated higher telehealth utilization compared to non-Hispanic White participants.
Our data also indicated that patients with a history of BC that had some college education were more likely to have utilized telehealth services. A supporting study with a subgroup analysis revealed that education levels were significantly associated with knowledge and prior experience with telehealth [20]. In our study, marital status was identified as a factor in telehealth usage among BC survivors, as well. This is consistent with previous research that has examined the benefits of marriage and healthcare [21, 22]. Marital status often serves as an indirect indicator of social support. A spouse can play a crucial role in encouraging patients to attend appointments and adhere to their care plans, including supporting the use of telehealth by helping set up technology, reminding patients of virtual visits, or providing assistance during the appointment itself [22]. Lastly, we found that being employed was associated with increased participation. Similarly, another study compared telehealth utilization between employed and non-employed patients, revealing that full-time employed patients were 15% more likely to use telehealth compared to unemployed patients [19].
Although there was not a statistically significant difference in telehealth usage based on home Internet access in this study, other research has shown that lack of reliable Internet is an important socioeconomic barrier to telehealth use. [23, 24] For instance, approximately 21 to 42 million Americans lack high-speed Internet access, which impacts their ability to utilize telehealth services. [24] These issues play a crucial role in delivering adequate telehealth care and decrease satisfaction among medically underserved communities [23–25]. In addition, low digital literacy creates significant barriers for many groups in accessing remote healthcare. While telehealth offers advantages, several studies have highlighted that many BC survivors were resistant to the idea and favored in-person visits. They valued face-to-face interactions, especially for crucial discussions and breast examinations, as these visits provided a sense of comfort and a stronger personal connection with their healthcare providers. [13, 26–28] The physical presence during appointments was perceived as more reassuring and conducive to building trust and understanding between patients and doctors, which they found lacking in virtual consultations. ^13^ While our study did not examine this directly, it is possible that patients without a prior trusting relationship with their provider may feel this effect more strongly, which they sometimes found lacking in virtual consultations. In our subgroup analysis of patients with a history of BC, surgical treatment was associated with reduced telehealth utilization. This may reflect that BC survivors experienced health issues requiring in-person visits, either due to new symptoms or ongoing aspects of their treatment, reducing the need or feasibility of virtual visits. However, because the survey did not capture whether participants were undergoing active treatment, it is possible that some BC survivors required in-person visits due to ongoing treatment or emerging health issues, which may partly explain their lower telehealth use. This phase of care often necessitates in-person encounters—for procedures such as drain removal—or reflects patient preferences for discussing results face-to-face.
Strengths
This study had several strengths including a large sample size that allowed for the capture of data from a broad patient population. Since this study was part of the NCI-funded IC-4 initiative, it benefited from a collaborative approach with 16 other NCI-designated Cancer Centers in developing a comprehensive survey instrument. The study utilized multiple recruitment strategies to include underserved, vulnerable, and minority populations. The use of several remote data collection methods allowed for the inclusion of more patients. We had an option for non-English speaking participants to complete the survey in their preferred language. We also included primary caregivers, recognizing that their involvement in care coordination and technological support provides insight into factors influence telehealth uptake that may not be fully captured through patient responses alone. By capturing unique, timely, and relevant data, the study provided insights into BC patient preferences during the COVID-19 pandemic. These findings can lead to a comprehensive understanding of how the pandemic influenced healthcare choices and behaviors.
Limitations
Several limitations were identified in our study. Firstly, the lack of diversity within our sample, primarily comprising White respondents, restricts the generalizability of our findings to more diverse demographic groups. Secondly, reliance on survey data introduces the potential for response bias, where participants may have responded in ways influenced by societal expectations or the context of the COVID-19 pandemic. Specifically, the preference for telehealth appointments during COVID-19, driven by the need for social distancing, may have skewed our results toward an overrepresentation of positive attitudes toward telehealth. Third, due to the survey-based nature of this study, we were unable to collect detailed clinical information regarding cancer treatment type or phase of care. Importantly, we did not distinguish between survivors receiving active systemic chemotherapy and those on long-term endocrine (hormone) therapy. This distinction is clinically meaningful, as patients undergoing chemotherapy often require more frequent in-person monitoring, management of treatment-related toxicities, and hospital-based care, whereas patients on oral endocrine therapy may be managed longitudinally in the outpatient setting over several years. Differences in treatment modality may therefore influence both the appropriateness of telehealth use and patient preferences. The absence of treatment-specific data limits our ability to contextualize telehealth utilization patterns and may partially explain the lower observed telehealth use among breast cancer survivors. Furthermore, we were not able to collect information on the reasons for telehealth visits, for example whether BC survivors were undergoing active treatment, which may have influenced their ability or need to use telehealth. This limitation may partly explain the lower observed telehealth use among BC survivors, as some aspects of BC care—particularly physical examination—cannot be adequately performed virtually. The inherent limitations of telehealth in replacing in-person clinical assessment should be considered when interpreting patient preferences (e.g., adherence improvement).
Fourth, because the survey was interviewer-administered for a small subset of the sample by a bilingual staff member, some social desirability bias may have been introduced, although the use of bilingual staff was necessary to ensure equitable participation among individuals with limited English proficiency. Lastly, the composition of our sample may not fully reflect real-world BC populations. Our recruitment strategy—rely on Ohio-based individuals previously enrolled in OSU research cohorts, community listservs, and caregiver nominations—may have introduced selection bias, as these participants may differ from the broader BC population in engagement, access to care, and technology comfort. Additionally, caregivers were included in the sample, and although their perspectives provide valuable insight, their inclusion may influence the overall findings and should be interpreted with this context in mind. These factors collectively highlight the need for caution in generalizing our findings to broader populations or to clinical decision-making regarding telehealth use in BC care. Despite these limitations, understanding how the pandemic affected patient preferences in our catchment area remains important for informing future models of care.
Conclusion
Based on our findings, further analysis focusing on the subgroup of women with a BC diagnosis would strengthen our understanding of factors that influence utilization of telehealth. This analysis could provide valuable insights into potential barriers to telehealth adoption, particularly in scenarios where patient considerations such as immunocompromised state (from chemotherapy) or societal factors such as lockdowns during the pandemic which may restrict in-person healthcare visits. Understanding these barriers is crucial for ensuring continued engagement in healthcare among BC survivors and identifying populations that may benefit from telehealth, while recognizing that individuals undergoing active treatment may still require frequent in-person visits. By exploring these dynamics, future studies can contribute to improving healthcare delivery and enhancing access to essential services for this vulnerable population.
Supplementary Information
Below is the link to the electronic supplementary material.Supplementary file1 (DOCX 18 KB)
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1American Cancer Society. Breast Cancer Statistics | How Common Is Breast Cancer? www.cancer.org. Published January 17, 2024. https://www.cancer.org/cancer/types/breast-cancer/about/how-common-is-breast-cancer.html#:~:text=At%20this%20time%20there%20are
- 2Office USGA. Telehealth in the Pandemic—How Has It Changed Health Care Delivery in Medicaid and Medicare? www.gao.gov. Published September 29, 2022. https://www.gao.gov/blog/telehealth-pandemic-how-has-it-changed-health-care-delivery-medicaid-and-medicare#:~:text=To%20prevent%20the%20spread%20of
- 3Alyafei A, Easton-Carr R. The health belief model of behavior change. [Updated 2024 May 19]. In: Stat Pearls [Internet]. Treasure Island (FL): Stat Pearls Publishing; 2025 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK 606120/26.