Complement and autoantibody levels under anifrolumab therapy in SLE: implications for clinical practice
Jan-Gerd Rademacher, Björn Tampe, Peter Korsten

TL;DR
Anifrolumab improves SLE patients' clinical outcomes without affecting traditional blood markers like complement and autoantibodies.
Contribution
This study shows that anifrolumab improves SLE without altering key serological markers, suggesting clinical monitoring is more relevant than lab tests.
Findings
76.9% of patients showed clinical improvement with an average SLEDAI-2K reduction of 3.77 points.
Complement levels (C3c, C4) and anti-dsDNA antibodies remained largely unchanged during treatment.
No correlation was found between clinical improvement and changes in serological markers.
Abstract
Anifrolumab (ANI), a type I interferon receptor antagonist, has demonstrated clinical efficacy in systemic lupus erythematosus (SLE). However, its effects on serological markers commonly used to assess disease activity in clinical practice remain uncertain. This study evaluated changes in complement and autoantibody levels in SLE patients treated with ANI under routine care conditions. We performed a single-center retrospective analysis of SLE patients receiving ≥3 ANI infusions over a 12-month period. Clinical and serological data, including complement (C3c, C4), anti-double-stranded DNA (anti-dsDNA) antibodies, prednisone dose, and SLE Disease Activity Index 2000 (SLEDAI-2K) scores, were analyzed using mixed-effects modeling (REML). Correlations between changes in clinical SLEDAI-2K (excluding serological components) and serological markers were assessed. Thirteen patients (84.6%…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
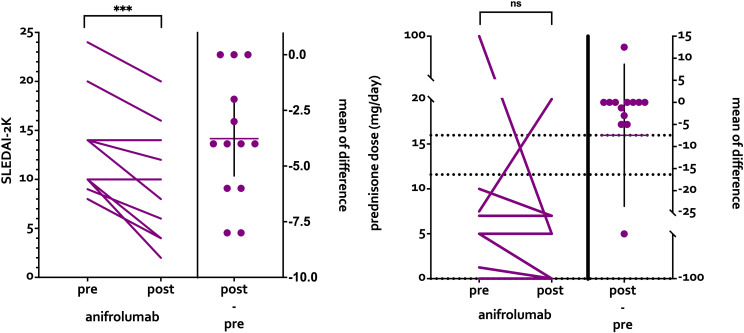 Figure 1
Figure 1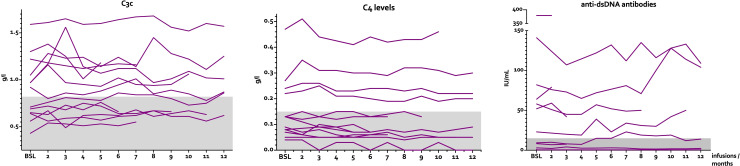 Figure 2
Figure 2| No. | Age | Sex | Dis. Dur. (y) | anti-dsDNA | Other Ab | Conc. Rx | ANI Inf. | Prednisolon (mg/d) | SLEDAI BSL | ΔSLEDAI (last follow up) |
|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 34 | M | 3 | + | Sm, SSA, U1RNP | – | 11 | 7.5 → 20 | 20 | -4 |
| 2 | 31 | F | 15 | + | Sm, SSA, U1RNP, Histone | HCQ, AZA | 12 | 5 → 0 | 10 | -6 |
| 3 | 78 | M | – | – | Sm, U1RNP | HCQ | 12 | 0 → 0 | 10 | -8 |
| 4 | 63 | F | 2 | + | SSA, SSB, Ro52, KU, CCP, RF | HCQ, AZA | 3 | 0 → 0 | 8 | -4 |
| 5 | 33 | F | 11 | – | – | HCQ, MMF | 12 | 10 → 7 | 24 | -4 |
| 6 | 58 | F | 2 | + | – | HCQ, AZA | 3 | 1.25 → 0 | 10 | -8 |
| 7 | 41 | F | 7 | + | RibP | HCQ | 3 | 5 → 0 | 12 | -4 |
| 8 | 53 | F | 5 | + | – | HCQ, MTX | 7 | 5 → 0 | 14 | -6 |
| 9 | 61 | F | 18 | + | Mi-Alpha | – | 9 | 0 → 0 | 10 | 0 |
| 10 | 38 | F | 18 | + | SSA, SSB | HCQ | 3 | 5 → 0 | 14 | -2 |
| 11 | 65 | F | 11 | + | SSA, SSB | AZA | 12 | 5 → 5 | 9 | -3 |
| 12 | 38 | F | 10 | – | SSA, U1RNP | AZA, MMF | 3 | 7 → 0 | 14 | 0 |
| 13 | 62 | F | – | + | Histone | HCQ, AZA | 12 | 5 → 7.5 | 8 | -4 |
| Δ cSLEDAI | C3c | C4 | dsDNA |
|---|---|---|---|
| Spearman r | -0.40 (CI -0.79 – 0.21) | 0.22 (CI -0.39 – 0.70) | -0.27 (CI -0.7 – 0.34) |
| p-value | 0.17 | 0.46 | 0.36 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsSystemic Lupus Erythematosus Research · Multiple Sclerosis Research Studies · Liver Diseases and Immunity
Introduction
1
Anifrolumab (ANI) is a monoclonal antibody approved for systemic lupus erythematosus (SLE) based on its clinical benefits shown in the TULIP trials (1, 2). However, its influence on serological markers, commonly used in clinical practice to guide the therapeutic response, remains uncertain. Since validated disease activity indices, such as the Systemic Lupus erythematosus Disease Activity Index (SLEDAI) (3), are not widely used outside trials (4), we aimed to clarify how ANI affects key serological parameters in routine care. We, therefore, retrospectively analyzed changes in serological markers among SLE patients treated with ANI since January 2022 at a single center.
Methods
2
Patient cohort and data collection
2.1
This was a single-center retrospective analysis conducted at the Department of Nephrology and Rheumatology, University Medical Center Göttingen, Germany. We only included patients who had received ≥3 infusions during an observation period of up to 12 months.
Eligible patients were adults (≥18 years) with a confirmed diagnosis of SLE according to the 2019 EULAR/ACR classification criteria or the 1997 ACR revised criteria. Inclusion required treatment with ANI (300 mg intravenously every 4 weeks) with a minimum of three infusions administered. Patients who discontinued therapy before the third infusion were excluded. There was no restriction on concomitant immunomodulatory therapy. Patients were identified through the institutional pharmacy records for ANI dispensing between January 2022 and March 2024.
We collected demographic and clinical data, along with complement factors (C3c, C4), anti-dsDNA antibody levels, disease activity using the SLEDAI-2K, and daily prednisone dose. Demographic variables included age, sex, and disease duration. Clinical data encompassed SLE manifestations classified by SLEDAI-2K organ domains, concomitant and prior immunomodulatory therapies (hydroxychloroquine, azathioprine, mycophenolate mofetil, methotrexate, cyclophosphamide, belimumab, and rituximab), and the number of ANI infusions received. C3c and C4 were determined by nephelometry, and anti-dsDNA antibodies by ELISA. Serological parameters and clinical assessments were obtained at each routine clinical visit every 4 weeks. Accordingly, data were collected at baseline (prior to the first infusion) and at infusion visits 2 – 12, as applicable. Of note, not every patient had complete serological data at each visit.
Statistical analysis
2.2
We analyzed changes in the SLEDAI-2K and prednisone doses before and after the use of ANI. Data with repeated measures were analyzed using a mixed-effects model (restricted maximum likelihood, REML). This method accounts for repeated measures and can handle missing values without the need for imputation.
Further, we performed a correlation analysis to assess the correlation of the clinical SLEDAI-2K with serological parameters. For this analysis, we recorded the clinical SLEDAI-2K (SLEDAI-2K without complement and anti-dsDNA levels) at baseline and at last follow-up. Spearman rank correlation coefficients were calculated to assess the association between the change in clinical SLEDAI-2K (ΔcSLEDAI-2K) and the change in each serological parameter (ΔC3c, ΔC4, Δanti-dsDNA) from baseline to last follow-up. 95% confidence intervals for the correlation coefficients were computed.
All analyses were performed with GraphPad Prism version 10.4.2 for Mac, GraphPad Software, Boston, Massachusetts USA, www.graphpad.com. A two-sided p-value < 0.05 was considered statistically significant.
Results
3
Baseline characteristics
3.1
In our cohort, there were 13 (11 female, 84.6%) patients with sufficient clinical data. Baseline characteristics are displayed in Table 1. The median age was 53 (31–78) years, the median disease duration was 10 (2–18) years. All patients were positive for antinuclear antibodies (ANA). Ten of 13 patients (76.9%) were positive for anti-dsDNA antibodies at any time during their disease course. Additional autoantibody specificities included anti-Sm (n = 3), anti-SSA (n = 5), anti-SSB (n = 3), anti-U1RNP (n = 4), anti-histone (n = 2), anti-ribosomal P (n = 1), and anti-Mi-alpha (n = 1). The most frequent concomitant immunomodulatory therapies at baseline were hydroxychloroquine (n = 9, 69.2%), azathioprine (n = 6, 46.2%), and mycophenolate mofetil (n = 3, 23.1%). Five patients (38.5%) had previously received belimumab, and three (23.1%) had previously received rituximab. At baseline, the median SLEDAI-2K score was 10 (8–24), and 10 of 13 (76.9%) patients had decreased complement levels and/or increased anti-double stranded (ds) DNA levels. The most common clinical SLEDAI-2K domains at baseline were arthritis (n = 7, 53.8%), rash (n = 6, 46.2%), neuropsychiatric SLE (NPSLE, n = 4, 30.8%), mucosal ulcers (n = 3, 23.1%), and hematuria (n = 2, 15.4%). Individual patient-level data including demographics, autoantibody profiles, concomitant therapies, and SLEDAI-2K domain involvement are presented in the Supplementary Table.
The median number of infusions in one year was 9 (range 3–12), the duration of follow-up was 12 months on an individual patient level.
Clinical response
3.2
During follow-up, 10/13 (76.9%) patients showed clinical improvement, the SLEDAI-2K decreased by 3.77 ± 2.78 points (p<0.001). A prednisone reduction was achieved in 5/13 (38.5%) patients, which was not statistically significant (Figure 1). Specifically, of the five patients with prednisone reduction, four achieved complete discontinuation (from a median of 5 mg/day to 0 mg/day). Two patients (15.4%) had an increase in prednisone dose during follow-up (patient 1: from 7.5 to 20 mg/day; patient 13: from 5 to 7.5 mg/day).
SLEDAI-2k and prednisone dose before and after anifrolumab therapy.
Serological parameters
3.3
Using a mixed-effects model for repeated measures, complement and anti-dsDNA levels remained largely unchanged during follow-up (Figure 2). There were no statistically significant changes during the course of the treatment (C3c, p=0.2502; C4, p=0.1013; anti-dsDNA, p=0.1164). At baseline, median C3c was 0.92 g/L (0.43-1.59), median C4 was 0.13 g/L (0.04-0.47), and median anti-dsDNA was 37.5 IU/mL (0.5-379]). At last follow-up, median C3c was 0.87 g/L (0.55-1.57), C4 was 0.09 g/L (0-0.46), and anti-dsDNA was 14 IU/mL (0.6-109). The mean absolute changes from baseline to last follow-up were ΔC3c = 0.06 g/L (0.01-0.2), ΔC4 = 0.02 g/L (0-0.06), and Δanti-dsDNA = 1.8 IU/mL (0-32).
Levels of C3c, C4, and double-stranded DNA antibodies over time.
Correlation between clinical and serological changes
3.4
Further, we analyzed whether the observed differences of the clinical SLEDAI-2K before and after treatment (ΔcSLEDAI-2K) correlated with changes of the complement or anti-dsDNA levels. Here, we observed no correlation between changes in cSLEDAI-2K scores and serological parameters (Table 2). The Spearman correlation coefficients were as follows: ΔcSLEDAI-2K vs. C3c: r = −0.40 (95% CI −0.79 to 0.21, p = 0.17), ΔcSLEDAI-2K vs. C4: r = 0.22 (95% CI −0.39 to 0.70, p = 0.46), and ΔcSLEDAI-2K vs. anti-dsDNA: r = −0.27 (95% CI −0.70 to 0.34, p = 0.36). These findings indicate that clinical improvement under ANI therapy occurs independently of changes in anti-dsDNA and complement levels.
Discussion
4
Our results reaffirm ANI’s effectiveness in clinical practice but show that relying solely on serological parameters may be insufficient for monitoring response. The dissociation between clinical and serological outcomes suggests that clinicians should prioritize clinical domains, especially since SLEDAI-2K may not reflect improvement under ANI. Thus, assessment should emphasize clinical findings rather than complement or antibody levels alone. The observed discordance between clinical improvement and serological stability can be understood through the mechanism of action of anifrolumab. By blocking IFNAR1, ANI suppresses type I IFN-driven inflammation, which manifests clinically through improvements in skin disease, arthritis, and other organ involvement (1, 2). However, autoantibody production and complement consumption in SLE are driven primarily by B-cell hyperactivation and immune complex formation, pathways that are only partially dependent on type I IFN signaling (5). While type I IFN can promote B-cell differentiation and BAFF expression, the established pool of long-lived plasma cells producing anti-dsDNA antibodies may be relatively resistant to IFN blockade alone (6). Similarly, complement activation through the classical pathway is driven by circulating immune complexes and may persist even when clinical disease activity improves through IFN-independent mechanisms.
Our findings are consistent with the TULIP trial data. In the TULIP-2 trial, ANI achieved significantly higher BICLA response rates compared to placebo (47.8% vs. 31.5%), yet changes in complement and anti-dsDNA levels were modest (1). Post-hoc analyses of pooled TULIP data demonstrated that patients with low complement and/or elevated anti-dsDNA at baseline showed numerically greater clinical responses (7). However, only a minority of patients with elevated anti-dsDNA achieved seronegativity during the trial (8). These trial data support our real-world observation that ANI’s clinical efficacy is not primarily mediated through serological normalization which stands in marked contrast to other biologic therapies used in SLE. Belimumab (BEL), which directly inhibits BAFF and thereby reduces B-cell survival and autoantibody production, has been shown to reduce anti-dsDNA levels by approximately 41% and to normalize complement (C3 and C4) over 52 weeks (9). Similarly, the CD20-mediated B-cell depleting monoclonal antibody rituximab (RTX) achieves significant reductions in anti-dsDNA antibodies and normalization of complement levels in the majority of treated patients (10). These differences underscore the mechanistic heterogenicity of biologic therapies in SLE and highlight that serological response depends on the therapeutic target: agents directly targeting B cells (BEL, RTX) normalize serological markers, whereas ANI, targeting upstream innate immunity through IFN blockade, achieves clinical improvement predominantly through IFN-dependent pathways.
Given the dissociation between clinical and serological outcomes, alternative pharmacodynamic biomarkers should be considered for monitoring ANI therapy. The type I IFN gene signature (IFNGS) provides more objective evidence of IFNAR1 blockade (11, 12). However, IFNGS measurement is not routinely available in clinical practice. Other potential biomarkers under investigation include downstream transcriptomic changes, plasma proteomic markers (e.g., CXCL10/IP-10, TRAIL, MCP-1), and changes in B-cell subsets, particularly follicular helper T cells (13). Future studies should evaluate the clinical utility and feasibility of these biomarkers for monitoring ANI therapy.
Although limited by a small sample size and retrospective design, our findings provide insights for interpreting serological markers during ANI therapy. Clinical assessment should guide disease activity evaluation, as serological markers may lack relevance depending on the mechanism of action. This is important when using composite indices, like SLEDAI-2K, which incorporate serological parameters. In clinical practice, physicians often rely on changes of serological responses to judge the efficacy of any treatment in SLE. However, our data demonstrates that this assumption is incorrect with ANI, which can be explained by its mechanism of action.
Conclusions
5
In conclusion, the assessment of ANI’s therapeutic efficacy should rely on validated disease indices, such as the clinical SLEDAI-2K, rather than changes of serological parameters alone. In addition, the SLEDAI-2K incorporating immunological parameters may be misleading. To our knowledge, this is the first specific analysis of serological parameters and clinical responses in a cohort of SLE patients treated with ANI.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Morand EF Furie R Tanaka Y Bruce IN Askanase AD Richez C . Trial of anifrolumab in active systemic lupus erythematosus. N Engl J Med. (2020) 382:211–21. doi: 10.1056/NEJ Moa 1912196, PMID: 31851795 · doi ↗ · pubmed ↗
- 2Furie RA Morand EF Bruce IN Manzi S Kalunian KC Vital EM . Type I interferon inhibitor anifrolumab in active systemic lupus erythematosus (TULIP-1): a randomised, controlled, phase 3 trial. Lancet Rheumatol. (2019) 1:e 208–19. doi: 10.1016/S 2665-9913(19)30076-1, PMID: 38229377 · doi ↗ · pubmed ↗
- 3Gladman DD Ibañez D Urowitz MB . Systemic lupus erythematosus disease activity index 2000. J Rheumatol. (2002) 29:288–91. 11838846 · pubmed ↗
- 4Albrecht K Thiele K Alexander T Aringer M Detert J Eidner T . Annual report 2025 from the National Database of the Regional Collaborative Rheumatology Centers in Germany. Z Rheumatol. (2025) 84(9):761–71. doi: 10.1007/s 00393-025-01646-8, PMID: 40323420 PMC 12605611 · doi ↗ · pubmed ↗
- 5Crow MK . Type I interferon in the pathogenesis of lupus. J Immunol. (2014) 192:5459–68. doi: 10.4049/jimmunol.1002795, PMID: 24907379 PMC 4083591 · doi ↗ · pubmed ↗
- 6Rönnblom L Leonard D . Interferon pathway in SLE: one key to unlocking the mystery of the disease. Lupus Sci Med. (2019) 6:e 000270. doi: 10.1136/lupus-2018-000270, PMID: 31497305 PMC 6703304 · doi ↗ · pubmed ↗
- 7Vital EM Merrill JT Morand EF Furie RA Bruce IN Tanaka Y . Anifrolumab efficacy and safety by type I interferon gene signature and clinical subgroups in patients with SLE: post hoc analysis of pooled data from two phase III trials. Ann Rheumatic Dis. (2022) 81:951–61. doi: 10.1136/annrheumdis-2021-221425, PMID: 35338035 PMC 9213795 · doi ↗ · pubmed ↗
- 8Tanaka Y Atsumi T Okada M Miyamura T Ishii T Nishiyama S . Efficacy of anifrolumab in systemic lupus erythematosus patients with serological manifestations: A post hoc analysis of the Japan subgroup of the TULIP-2 trial. Modern Rheumatol. (2025) 35:458–69. doi: 10.1093/mr/roae 111, PMID: 39821415 · doi ↗ · pubmed ↗