Beta-blocker use and outcome after allogeneic hematopoietic stem cell transplantation in acute myeloid leukemia
Johanna Werk, David Baden, Inna Shaforostova, Jan-Henrik Mikesch, Christian Reicherts, Julia Marx, Georg Lenz, Christoph Schliemann, Matthias Stelljes, Alexander Pohlmann

TL;DR
Beta-blockers may reduce leukemia relapse after stem cell transplants in AML patients, but increase non-relapse mortality.
Contribution
First study to show beta-blocker use is linked to post-transplant outcomes in AML patients.
Findings
Beta-blockers were associated with lower relapse rates but higher non-relapse mortality.
Multivariable analysis confirmed beta-blockers independently affect relapse and non-relapse mortality.
Chronic GvHD or organ toxicity was more common in beta-blocker users as a cause of death.
Abstract
Allogeneic hematopoietic stem cell transplantation (HSCT) is curative for patients with acute myeloid leukemia (AML) through an immune-mediated graft-versus-leukemia effect, but relapse is common. Studies in solid tumors have shown that adrenergic stress impairs anti-tumor immunity, and that beta-blockade can prolong survival in mice and patients receiving immunotherapy. To this end, we investigated whether beta-blocker use impacts outcomes in AML patients undergoing HSCT. We analyzed the cumulative incidences of relapse (CIR), non-relapse mortality (NRM) and overall survival (OS) in 413 patients with AML who underwent first allogeneic HSCT. A total of 112 patients (27%) received beta-blockers after HSCT. The use of beta-blockers was associated with a lower CIR (P = 0.024), but with a higher NRM (P = 0.002); OS did not differ. In multivariable analyses, beta-blocker use emerged as an…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
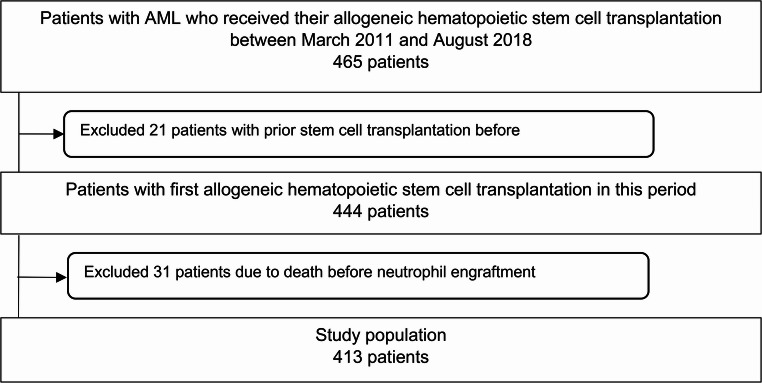 Figure 1
Figure 1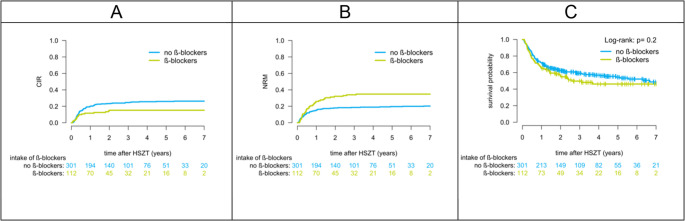 Figure 2
Figure 2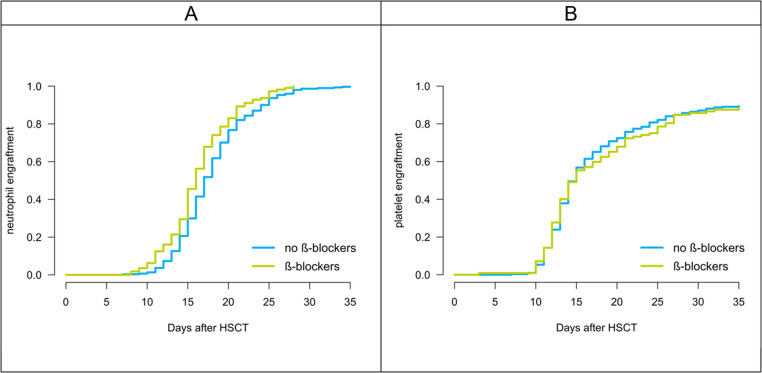 Figure 3
Figure 3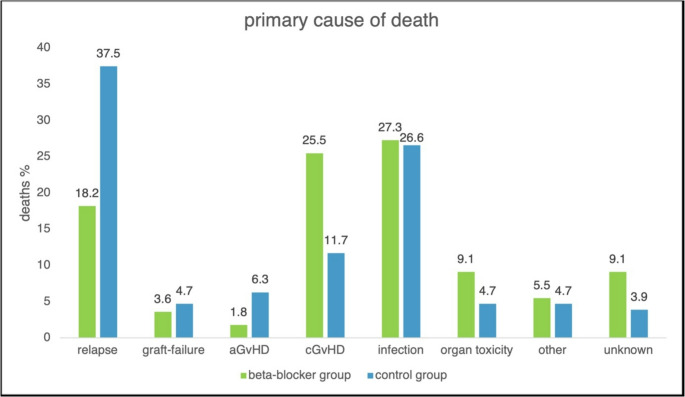 Figure 4
Figure 4- —Universitätsklinikum Münster (8918)
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCancer, Stress, Anesthesia, and Immune Response · Immune Response and Inflammation · Receptor Mechanisms and Signaling
Introduction
Allogeneic hematopoietic stem cell transplantation (HSCT) remains a curative treatment approach for patients with acute myeloid leukemia (AML). Despite improvements in supportive care and transplant procedures, long-term survival is still compromised by relapse, reported as cumulative incidence of relapse (CIR), and non-relapse mortality (NRM) [1]. Strategies to identify modifiable risk factors are therefore of major clinical interest.
Adrenergic signaling has been shown to regulate tumor biology and immune responses. Preclinical models demonstrated that stress hormones can promote tumor growth, metastasis, and immune dysregulation [2–4]. These findings provide a rationale for investigating pharmacological beta-adrenergic blockade as a potential modifier of cancer outcomes.
Clinically, evidence remains heterogeneous. Some retrospective studies suggested favorable effects of beta-blocker therapy on tumor progression and survival in solid tumors [5]. However, results across different entities and treatment settings have been inconsistent. A recent systematic review and meta-analysis, comprising 79 studies with nearly 500,000 patients, reported an association between beta-blocker use and improved progression-free survival but no consistent benefit for overall or cancer-specific survival. Importantly, substantial heterogeneity and risk of bias were noted [6].
To date, no study has investigated the potential influence of beta-blocker exposure on outcomes after HSCT in patients with AML. The present analysis therefore aimed to evaluate the association between beta-blocker use and post-transplant outcomes including cumulative incidence of relapse (CIR), non-relapse mortality (NRM), and overall survival (OS) in AML patients undergoing allogeneic HSCT.
Methods
Patient characteristics
Patients with AML who underwent first allogeneic HSCT at the Bone Marrow Transplantation Center of the University Hospital Münster, Germany, between March 2011 and August 2018 were included. Initially, 465 transplanted AML patients were screened, of whom 52 patients were excluded. Twenty-one patients were excluded because of previous HSCT (e.g. for myelodysplastic syndrome) and 31 patients were excluded because of early death after transplantation before neutrophil engraftment. Thus, a total of 413 AML patients were included in the final analysis set (Fig. 1).Fig. 1. Flow diagram showing inclusion and exclusion of patients with acute myeloid leukemia (AML) undergoing allogeneic hematopoietic stem cell transplantation (HSCT) between March 2011 and August 2018. A total of 413 patients were included in the final analysis
The intervention of interest was beta-blocker use, defined as (1) beta-blockers as part of the discharge medication after allogeneic HSCT or (2) beta-blocker medication for at least 14 consecutive days after neutrophil engraftment during the inpatient stay of HSCT. All patients taking beta-blockers at discharge had to continue taking beta-blockers for at least 60 days after HSCT. We therefore applied a landmark design including only patients who survived until neutrophil engraftment; exposure to beta-blockers was defined thereafter. Beta-blockers were prescribed for standard clinical indications at the treating physician’s discretion; no patient received beta-blockers with the intent to influence relapse or other study endpoints. Patients with short-term beta-blocker exposure not meeting the predefined criteria were classified as non-users (n = 25). Beta-blocker exposure was observed throughout the entire study period (2011–2018) without clustering in a specific time window (Supplementary Table 4). In addition, patients taking beta-blockers were further divided into high-dose and low-dose beta-blocker groups based on total daily dose. The low-dose group included those patients with a daily dose of less than or equal to 30 mg propranolol, 5 mg bisoprolol, 70 mg metoprolol, 2.5 mg nebivolol or 12.5 mg carvedilol. Any daily dose above these limits was considered high-dose. We also recorded the intake of calcium channel blockers, angiotensin-converting enzyme (ACE) inhibitors and angiotensin II receptor blockers (ARBs).
The study was approved by the Ethics Committee of Westphalia-Lippe (2021-490-f-S) and was conducted in accordance with the Declaration of Helsinki and its later amendments.
Outcomes and measurements
Patient data were collected retrospectively from medical records. Post-transplant AML relapse was defined as at least 5% leukemic blasts in a bone marrow aspirate, reappearance of blasts in peripheral blood or new extramedullary leukemia. The CIR was calculated by considering deaths from causes other than relapse as a competing risk. Deaths from any cause without prior relapse are events assigned to the NRM with relapse as a competing event. OS was defined as the time from the date of cell transplantation to death or last contact. Median follow-up time was calculated using the reverse Kaplan-Meier method.
Neutrophil engraftment was defined as the first of three consecutive days with at least 500 granulocytes/µL after transplantation. Platelet engraftment was defined as the first platelet count greater than 20,000/µL for more than three days without platelet transfusion. Diagnosis and grading of acute GvHD (aGvHD) and chronic GvHD (cGvHD) were performed according to standard criteria [7–10]. Primary cause of post-transplant death was assessed according to the criteria of Copelan et al. [11].
Statistical analysis
Patients were divided into beta-blocker users and non-users according to the definitions outlined above. Normality of continuous variables was assessed using the Shapiro–Wilk test. Two independent groups were compared using the Mann–Whitney U test for continuous variables and the χ² test (or Fisher’s exact test when appropriate) for categorical variables. OS was estimated with the Kaplan–Meier method and compared using the log-rank test. CIR and NRM were estimated using the Aalen–Johansen estimator. Survival probabilities were reported at 2 years. Univariate and multivariable effects were assessed for CIR and NRM using the Fine–Gray subdistribution hazards model, and for OS using Cox proportional hazards models. The following covariates were included a priori to control for confounding rather than selected by model-selection procedures: age, sex mismatch, donor match, donor relationship, remission status, and beta-blocker use.
The P value for interaction was obtained from likelihood-ratio tests comparing nested models with and without the interaction term. Analyses were conducted using RStudio (version 1.1.463) and SPSS (version 26). Statistical significance was defined as a two-sided P value < 0.05.
Results
Patient characteristics
A total of 413 patients with AML who underwent allogeneic HSCT met the eligibility criteria for this retrospective single-center study. At the time of the analysis, 183 (44.3%) patients had died. Patient, disease, and transplant characteristics are listed in Table 1.
Table 1. Patient, disease and transplantation characteristicsVariablesNo beta-blockerBeta-blockerP valueN, no (%)301 (72.9)112 (27.1)Age, years< 0.001* Median (range)52 (18–75)59 (20–75)Sex, no (%)0.117** Male170 (56.5)73 (65.2) Female131 (43.5)39 (34.8)AML type, no (%)0.072** de novo232 (77.1)79 (70.5) t-AML17 (5.6)3 (2.7) s-AML52 (17.3)30 (26.8)ELN 2010, no (%)0.433** Favorable52 (17.3)18 (16.1) Intermediate179 (59.5)63 (56.3) Adverse68 (22.6)31 (27.7) Unknown2 (0.7)0 (0)NPM1 status, no (%)0.792** Wild-type231 (76.7)88 (78.6) Mutated69 (22.9)24 (21.4) Unknown1 (0.3)0 (0)FLT3 status, no (%)0.453** Wild-type231 (77.0)91 (81.3) ITD61 (20.3)17 (15.2) TKD8 (2.7)4 (3.6)Remission status at HSCT, no (%)0.512** Complete remission (CR)165 (54.8)55 (49.1) CR1140 (46.5)45 (40.2) CR ≥ 225 (8.3)9 (8.0) not determinable01 (0.9) Active AML136 (45.2)57 (50.9) Refractory105 (34.9)46 (41.1) Untreated relapse31 (10.3)11 (9.8)Comorbidities, no (%) Hypertension65 (21.6)58 (51.8)< 0.001* Atrial fibrillation/flutter6 (2.0)14 (12.5)< 0.001* Coronary heart disease2 (0.7)7 (6.3)0.002Donor age, years0.227* Median (range)37 (18–73)39 (19–76)Donor type, no (%)0.163 Related Mismatched1 (0.3)1 (0.9) Related Matched89 (29.6)27 (24.1) Unrelated Matched157 (52.2)70 (62.5) Unrelated Mismatched51 (16.9)12 (10.7) Haploidentical3 (1.0)2 (1.8)Sex mismatch, no (%)0.349** Female D/male R48 (15.9)13 (11.6) Other253 (84.1)99 (88.4)Graft source, no (%)1.000** PBSC291 (96.7)108 (96.4) BM10 (3.3)4 (3.6)CMV risk, no (%)0.701** D-/R-73 (24.3)27 (24.1) D+/R-32 (10.6)12 (10.7) D-/R+68 (22.6)31 (27.7) D+/R+128 (42.5)42 (37.5)Conditioning, no (%)0.247** MAC7 (2.3)0 (0) RIC135 (44.9)44 (39.3) NMA7 (2.3)2 (1.8) SEQ152 (50.5)66 (58.9)ATG, no (%)0.677** Yes241 (80.1)92 (82.1) No60 (19.9)20 (17.9)Immunosuppression, no (%)0.050** CsA/MMF163 (54.2)66 (58.9) CsA/MTX137 (45.5)43 (38.4) Other1 (0.3)3 (2.7)Neutrophil Engraftment, days0.002* Median (range)18 (7–38)16 (8–28)Platelet Engraftment, days0.820* Median (range)18 (7–84)19 (3–83)Acute GvHD, no (%)1.000** Grade 0–1239 (79.4)89 (79.5) Grade ≥ 262 (20.6)23 (20.5)Chronic GvHD, no (%)0.101** No cGvHD184 (61.1)70 (62.5) Mild29 (9.6)11 (9.8) Moderate34 (11.3)20 (17.9) Severe54 (17.9)11 (9.8)Primary Cause of Death, no (%)0.041** Relapse48 (37.5)10 (18.2) Graft failure6 (4.7)2 (3.6) aGvHD8 (6.3)1 (1.8) cGvHD15 (11.7)14 (25.5) Infection34 (26.6)15 (27.3) Organ Toxicity6 (4.7)5 (9.1) Other6 (4.7)3 (5.5) Unknown5 (3.9)5 (9.1)AML acute myeloid leukemia, ELN European Leukemia Net, CR complete remission, PBSC peripheral blood stem cells, BM bone marrow, D donor, R recipient, CMV cytomegalovirus, MAC myeloablative conditioning, RIC reduced intensity conditioning, NMA non-myeloablative conditioning, SEQ sequential conditioning, ATG antithymocyte globulin, CsA cyclosporine A, MMF mycophenolate mofetil, MTX methotrexate, GvHD graft-versus-host diseaseStatistical analysis: * Mann-Whitney U; ** χ² (Fisher’s exact test when appropriate)
The beta-blocker group included 112 patients (27.1%). The control group consisted of 301 patients (72.9%) who were not taking beta-blockers according to the definitions as outlined above. The median (range) age of the entire study population was 54 (18–75) years. Beta-blocker users were older than patients in the control group (median 59 vs. 52 years, P < 0.01) and more frequently had pre-existing cardiovascular comorbidities, including hypertension, atrial fibrillation, and coronary heart disease (Table 1). Two hundred and eighteen patients (52.8%) received a sequential conditioning regimen (SEQ) and 179 patients (43.3%) received fludarabine and total body irradiation (4 × 2 Gy) or a combination of melphalan and fludarabine with treosulfan or busulfan (RIC). In addition, 9 patients (2.2%) received non-myeloablative conditioning regimens (NMA), mostly consisting of fludarabine and total body irradiation with 2 × 2 Gy. Seven patients (1.7%) received myeloablative conditioning regimens (MAC). A total of 399 patients (96.6%) received peripheral blood stem cells (PBSC) and 14 patients (3.4%) received a bone marrow (BM) graft. Of the 413 patients, 220 patients (53.3%) were in complete remission (CR) prior to transplantation and 193 patients (46.7%) had active disease. Cyclosporine A in combination with methotrexate for GvHD prophylaxis was used in 180 cases (43.6%). Cyclosporine A in combination with mycophenolate mofetil was given to 229 patients (55.4%), and 4 patients (1.0%) received other medications for GvHD prophylaxis.
Two hundred and twenty-four patients (54.2%) were treated with at least one of the following cardiac medications: 112 patients (27.1%) were taking beta-blockers, 138 patients (33.4%) were treated with calcium channel blockers, and 83 patients (20.1%) were taking ACE inhibitors or ARBs. The distribution of medication use is shown in Supplement 1. Use of ACE inhibitors, ARBs or calcium channel blockers was not significantly associated with outcome (all P > 0.05).
Beta-blocker use and outcome after transplantation
Median follow-up was 43.2 months (95% CI, 39.6–51.2). Median OS for the entire cohort was not reached during follow-up. At 2 years, CIR was lower in the beta-blocker group than in controls (16.0% vs. 25.4%; P = 0.024; Fig. 2a). Conversely, the cumulative incidence of NRM was higher with beta-blocker use (35.7% vs. 19.1%; P = 0.002; Fig. 2b). For OS, the estimated 2-year survival was 49.7% (95% CI, 39.8–59.6) with beta-blockers and 59.3% (95% CI, 53.5–65.0) without beta-blockers (P = 0.353; Fig. 2c).
Eighty-five patients (20.6%) experienced aGvHD ≥ grade 2 and 159 (38.5%) patients had cGvHD. The beta-blocker and control groups did not differ in the incidence of acute or chronic GvHD (P > 0.05). In the beta-blocker group, 89 patients (79.5%) had no or grade 1 aGvHD, and 23 patients (20.5%) had aGvHD grade 2 or higher. In the control group, 239 patients (79.4%) had no aGvHD or aGvHD grade 1, and 62 patients (20.6%) had aGvHD grade 2 or higher. cGvHD affected 42 patients (37.5%) in the beta-blocker group and 117 patients (38.9%) in the control group (Fig. 3).Fig. 2(A) Cumulative incidence of relapse (CIR), (B) non-relapse mortality (NRM), and (C) overall survival (OS) after HSCT in patients receiving or not receiving beta-blockers. P values were obtained using Gray’s test (A, B) and the log-rank test (C).
Fig. 3(A) Neutrophil and (B) platelet engraftment after HSCT in patients receiving or not receiving beta-blockers. P values were derived from log-rank tests.
The primary cause of death differed significantly between the beta-blocker and control groups (P = 0.041). In the beta-blocker cohort, death was attributed to infection in 15 (27.3%) patients, cGvHD in 14 (25.5%) and AML relapse in 10 (18.2%). In the control group, the main cause of death was AML relapse in 48 (37.5%) patients, followed by infection in 34 (26.6%) and cGvHD in 15 (11.7%). Differences in primary cause of death are shown in Fig. 4.Fig. 4. Distribution of primary causes of death, according to previously published definitions [11], in patients receiving beta-blockers (green) and control patients (blue). aGvHD = acute graft-versus-host disease; cGvHD = chronic graft-versus-host disease
Univariate analyses of potential risk factors for CIR, NRM, and OS are shown in Table 2. Older age and active disease at transplantation were consistently associated with inferior outcomes across endpoints. For OS, additional associations were observed with donor match, donor relation, remission status, and conditioning therapy. Beta-blocker use was associated with a lower CIR but a higher NRM, while no significant association with OS was detected. Adjusted associations are reported in Table 3 and summarized below.
Table 2. Univariate analysis for cumulative incidence of relapse, non-relapse mortality and overall survivalCovariablesCIRNRMOSFine-GrayFine-GrayCox proportional hazardsHR (95% CI) P HR (95% CI) P HR (95% CI) P Age0.99 (0.98–1.01)0.6201.02 (1.00-1.04)0.0181.14 (1.01–1.28)0.032Sex mismatch NoRefRefRef Yes0.86 (0.48–1.54)0.6201.07 (0.63–1.81)0.8000.98 (0.66–1.47)0.923Donor match MatchedRefRefRef Mismatched1.05 (0.62–1.76)0.8601.76 (1.10–2.82)0.0191.64 (1.15–2.34)0.006Donor relation RelatedRefRefRef Unrelated1.41 (0.89–2.25)0.1501.23 (0.80–1.90)0.3401.45 (1.04–2.02)0.030Remission CRRefRefRef active disease1.08 (0.73–1.62)0.6901.95 (1.31–2.91)0.0011.60 (1.20–2.15)0.001Beta-blocker Non-useRefRefRef Use0.55 (0.33–0.94)0.0281.86 (1.25–2.77)0.0021.24 (0.90–1.70)0.180Ref Reference, HR Hazard ratio, CIR cumulative incidence of relapse, NRM non-relapse mortality, OS overall survival;Age was modeled per 1-year increase for CIR and NRM, and per 10-year increase for OS
Table 3. Multivariable analysis for cumulative incidence of relapse, non-relapse mortality and overall survivalCovariablesCIRNRMOSFine-GrayFine-GrayCox proportional hazardsHR (95% CI) P HR (95% CI) P HR (95% CI) P Age (per 10 years)1.00 (0.87–1.14)0.9601.15 (0.95–1.40)0.1601.09 (0.97–1.24)0.157Sex mismatch NoRefRefRef Yes0.94 (0.52–1.70)0.8301.12 (0.65–1.93)0.6801.06 (0.70–1.60)0.786Donor match MatchedRefRefRef Mismatched0.90 (0.52–1.56)0.7101.73 (1.09–2.74)0.0201.54 (1.08–2.22)0.019Donor relation RelatedRefRefRef Unrelated1.45 (0.87–2.44)0.1601 (0.65–1.58)0.9701.27 (0.89–1.80)0.181RemissionCRRefRefRef active disease1.08 (0.72–1.63)0.7201.78 (1.19–2.67)0.0051.49 (1.11-2.00)0.009Beta-blocker Non-useRefRefRef Use0.53 (0.31–0.92)0.0241.72 (1.13–2.64)0.0121.17 (0.84–1.62)0.353Ref Reference, HR Hazard ratio, CIR cumulative incidence of relapse, NRM non-relapse mortality, OS overall survival
In multivariable analyses, adjusting for demographics, donor characteristics and transplantation-related variables, beta-blocker use was independently associated with lower CIR (hazard ratio (HR), 0.53; 95% CI, 0.31–0.92; P = 0.024) and higher NRM (HR 1.72; 95% CI, 1.13–2.64; P = 0.012), but not OS (P = 0.353). Other variables associated with NRM were donor match (P = 0.020) and remission status before transplant (P = 0.005). There were no other covariates with an independent effect on CIR in our model. The results of the multivariable regression analysis are listed in Table 3.
Beta-blocker use was associated with an earlier neutrophil engraftment (at median on day 16 vs. 18 after HSCT in the beta-blocker group vs. control group; P = 0.002; Fig. 3a). There was no significant difference in platelet engraftment between the two groups (at median on day 19 vs. 18 after HSCT in the beta-blocker group vs. control group; P > 0.05; Fig. 3b).
In the beta-blocker group, 56 patients (50%) received bisoprolol and 51 patients (45.5%) received metoprolol. Only five patients (4.5%) were treated with other agents such as propranolol or carvedilol. Fifty-one patients (45.5%) received low-dose beta-blockers and 61 patients (54.5%) high-dose beta-blockers, according to the definitions given above. Medication characteristics are listed in Supplement 2. There was no difference in CIR, NRM and OS among high- and low-dose beta-blocker users (P > 0.05 for all outcome variables, data not shown). Similarly, there was no significant difference in CIR, NRM and OS between the different beta-blocker substances (P > 0.05).
The results of the subgroup analysis are shown in the forest plot for OS (Supplement 3). Exploratory analyses suggested significant interactions of beta-blocker use with antithymocyte globulin (ATG) administration (P_interaction = 0.01) and donor relation (P_interaction = 0.01). In patients transplanted from related donors, who uniformly did not receive ATG, beta-blocker use was associated with inferior OS (HR 2.58, 95% CI 1.42–4.67).
Discussion
In our analysis, among AML patients who received a first allogeneic HSCT, the use of beta-blockers was associated with a lower risk of post-transplant AML relapse. In contrast, the risk of death without prior AML relapse was higher among beta-blocker users. As a net effect of the lower CIR but higher NRM in beta-blocker users, OS did not differ between the beta-blocker and the control groups. Since age alone does not seem to be the main driver of this observation according to the results of the multivariable analyses, it is likely that the variable “beta-blocker use” marks vulnerable patients with a higher burden of pre-existing medical conditions in our retrospective analysis. Consistent with this interpretation, patients receiving beta-blockers more frequently had pre-existing cardiovascular comorbidities, including hypertension, atrial fibrillation, and coronary heart disease. These comorbidities may at least partly explain the higher non-relapse mortality observed among beta-blocker users. In this context, the higher proportion of infection-related deaths among beta-blocker users should be interpreted with caution, as reduced physiological reserve in patients with cardiovascular comorbidities may contribute to fatal infectious complications after HSCT rather than a direct effect of beta-blockade. On the other hand, we also investigated whether the use of calcium channel blockers, ACE inhibitors or ARBs predicted post-transplant outcome and found no significant associations with CIR, NRM or OS. However, within the group of patients on cardiovascular medications, the need for beta-blockers may still label the more vulnerable fraction of patients, i.e. those with a history of angina, myocardial infarction, or atrial fibrillation, whereas calcium channel blockers, ACE inhibitors or ARBs may be used by patients with arterial hypertension only.
Nevertheless, beta-blocker users had a lower cumulative risk of AML relapse in our study after adjusting for demographic, disease- and transplantation-related confounders, which may possibly indicate improved immunologic control of residual leukemia after transplantation. However, a dose-dependent effect was not observed. While there was no difference between beta-blocker users and non-users in the incidence of acute or chronic GvHD, consistent with a potential immunomodulatory effect of beta-blockers, we found that cGvHD was a major cause of death among patients in the beta-blocker group, ranking second after infections. In contrast, patients in the control group died mostly due to AML relapse.
In exploratory subgroup analyses, beta-blocker use showed a significant association with outcome among patients who either did not receive antithymocyte globulin (ATG) or underwent transplantation from a related donor. As related donor recipients in our cohort uniformly did not receive ATG, these factors were closely intertwined. Given the exploratory nature of these findings, they should be interpreted with caution. Our study has several limitations, most of which are inherent to its retrospective nature. First, we applied an engraftment-landmark design; patients who died before neutrophil engraftment were excluded. Consequently, causes of very early mortality, including early infectious deaths, could not be assessed. This may introduce selection bias and prevents assessment of very early post-transplant mortality. In addition, although patient characteristics such as age differed between the beta-blocker and non-beta-blocker groups, we cannot rule out additional unmeasured confounders. It also remains difficult to disentangle the relative contributions of underlying cardiovascular conditions from potential immune-related mechanisms to post-transplant NRM. Second, we were not able to demonstrate a dose–response relationship between beta-blocker dose and outcome variables. Third, beta-blocker exposure beyond our predefined criteria could not be verified in individual patients. Finally, although non-selective beta-blockers such as propranolol may exert stronger immunomodulatory effects than β1-selective agents the small number of patients receiving non-selective agents precluded further analysis [12]. Despite these limitations, our study is the first to demonstrate an association between beta-blocker use and post-transplant outcome in a large cohort of AML patients undergoing allogeneic HSCT. If confirmed in independent cohorts and laboratory studies, our findings may provide a rationale to investigate the effects of carefully titrated beta-adrenergic blockade on donor cell-mediated immune responses and post-transplant outcome in a prospective trial.
Supplementary Information
Below is the link to the electronic supplementary material.
Supplementary Material 1
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Powe DG et al (2010) Beta-blocker drug therapy reduces secondary cancer formation in breast cancer and improves cancer specific survival. Oncotarget 1(7):628–638. Accessed: Oct. 14, 2025. [Online]. Available: https://www.impactjournals.com/oncotarget/www.impactjournals.com/oncotarget 628