Efficacy and safety of goniotomy and gonioscopy-assisted transluminal trabeculotomy for exfoliation glaucoma: a systematic review and single-arm meta-analysis
Weijia Li, Yulei Geng, Kuitang Shi, Guangxian Tang, Xiaowei Yan, Yawen Li, Tianyu Zhang, Jiaming Lu, Shuai Wang, Hengli Zhang

TL;DR
This study reviews the effectiveness and safety of two surgical procedures for treating exfoliation glaucoma, finding that combining them with cataract surgery provides better long-term results.
Contribution
The study provides a systematic review and meta-analysis of goniotomy and GATT for exfoliation glaucoma, highlighting the benefits of combining these procedures with phacoemulsification.
Findings
GATT combined with phacoemulsification significantly reduced intraocular pressure and medication use at 1, 6, and 12 months.
Goniotomy combined with phacoemulsification also reduced intraocular pressure and medication burden, though with less pronounced effects.
Standalone GATT showed limited long-term intraocular pressure reduction, suggesting combined surgery is more effective for sustained control.
Abstract
To assess the efficacy and safety of goniotomy (GT) and gonioscopy-assisted transluminal trabeculotomy (GATT) with or without phacoemulsification (PEI) for exfoliation glaucoma (XFG). Searches were conducted in PubMed, Scopus, Embase, Ovid, and the Web of Science. Two independent reviewers performed study selection, data extraction, and quality assessment. The primary outcomes were the reduction in intraocular pressure (IOP) and the number of antiglaucoma medications (AGMs) at 1, 6, and 12 months postoperatively. Safety was assessed by the incidence of complications. Fourteen studies involving 624 eyes were included. The GATT ± PEI group showed significant IOP reductions of 1.96 mmHg (p < 0.01), 2.17 mmHg (p < 0.001), and 2.07 mmHg (p < 0.001) at 1, 6, and 12 months, respectively, with corresponding AGM reductions of 3.28 (p < 0.001), 2.87 (p = 0.003), and 2.54 (p = 0.011). The GT +…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
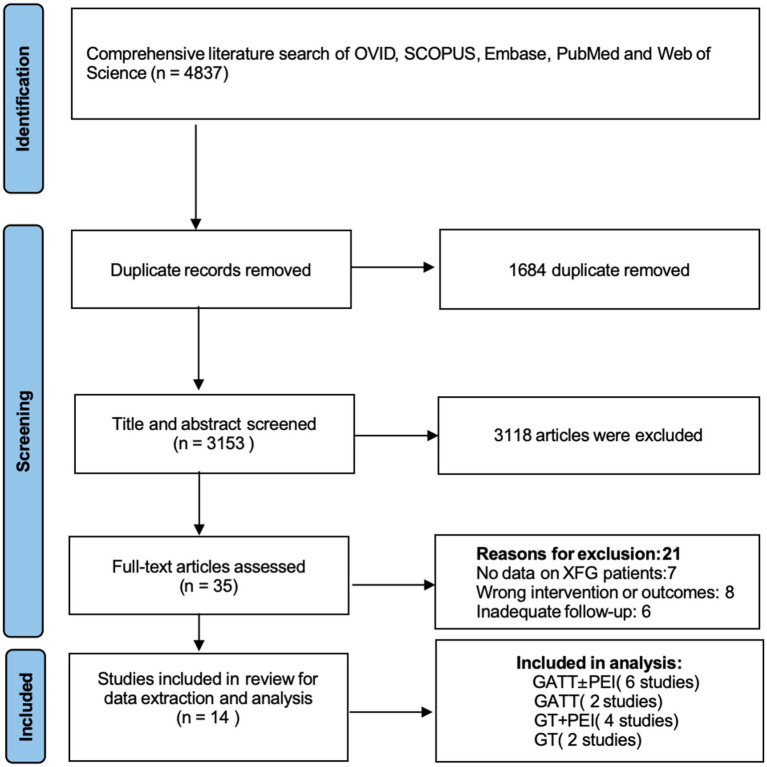 Figure 1
Figure 1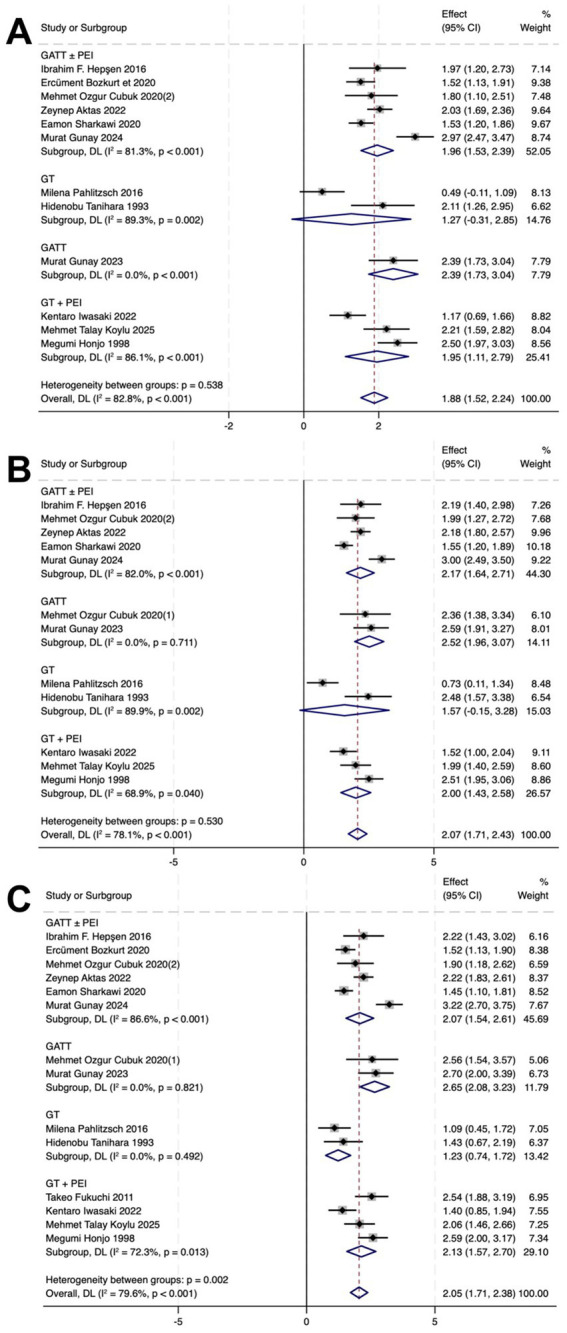 Figure 2
Figure 2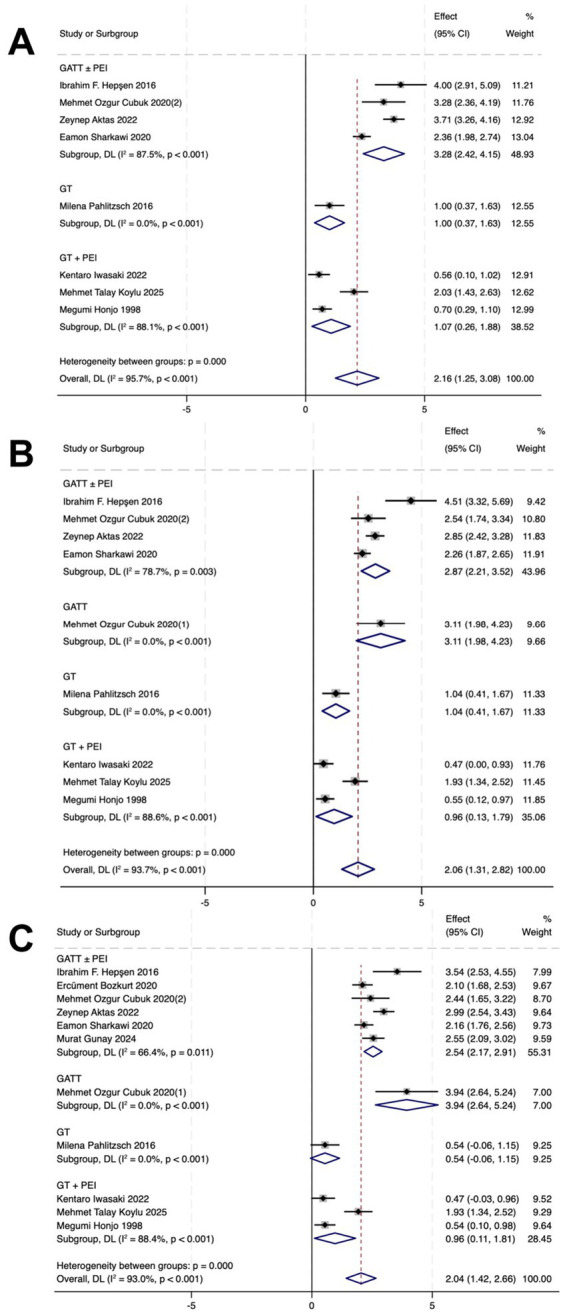 Figure 3
Figure 3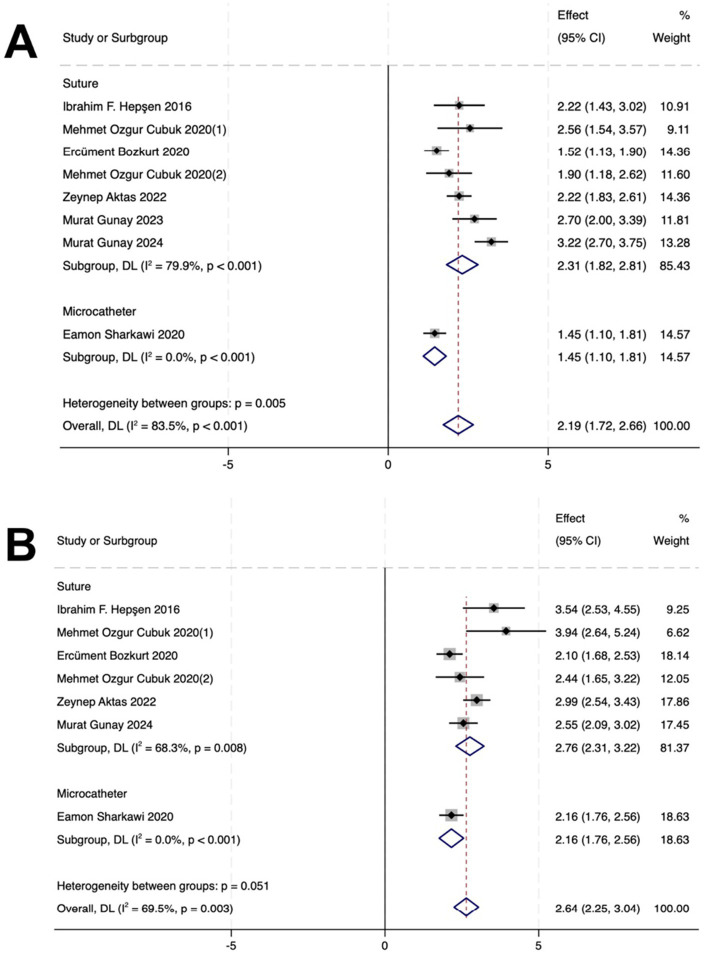 Figure 4
Figure 4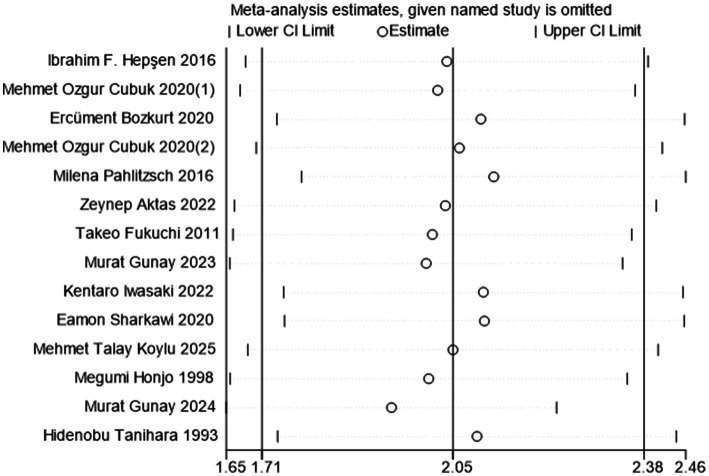 Figure 5
Figure 5| Author, Year | Country | No. of eyes | Age (years) | Preoperation medications | Baseline IOP (mmHg) | Quality evaluation |
|---|---|---|---|---|---|---|
| GATT ± PEI | ||||||
| Hepşen et al. ( | Turkey | 20 | 63.15 ± 6.78 | 3.15 ± 0.81 | 26.55 ± 8.91 | Good |
| Bozkurt et al. ( | Turkey | 66 | 68.91 ± 12.30 | 2.94 ± 1.21 | 25.35 + 8.52 | Good |
| Cubuk et al. ( | Turkey | 22 | 68.20 ± 7.00 | 3.50 ± 0.50 | 27.50 ± 10.00 | Good |
| Aktas et al. ( | Turkey | 111 | 72.00 ± 10.10 | 3.10 ± 0.80 | 26.10 ± 7.40 | Good |
| Sharkawi et al. ( | Turkey | 103 | 75.50 ± 8.90 | 2.90 ± 1.10 | 27.10 ± 11.7 | Good |
| Gunay et al. ( | Turkey | 31 | 70.70 ± 6.90 | 3.60 ± 0.60 | 29.43 ± 7.18 | Good |
| GATT | ||||||
| Cubuk et al. ( | Turkey | 14 | 65.30 ± 4.90 | 3.80 ± 0.40 | 24.60 ± 4.50 | Good |
| Gunay ( | Turkey | 31 | 68.60 ± 10.30 | 3.80 ± 0.50 | 28.00 ± 7.30 | Good |
| GT | ||||||
| Pahlitzsch et al. ( | Canada | 22 | – | 2.55 ± 0.96 | 20.86 ± 6.05 | Good |
| Tanihara et al. ( | Japan | 17 | 59.50 ± 11.80 | – | 30.80 ± 8.40 | Good |
| GT+ PEI | ||||||
| Fukuchi et al. ( | Japan | 33 | 76.20 ± 4.23 | 3.21 ± 1.58 | 22.40 ± 5.13 | Good |
| Koylu et al. ( | Turkey | 33 | 69.40 ± 5.90 | 3.70 ± 0.50 | 27.10 ± 7.90 | Good |
| Honjo et al. ( | Japan | 49 | 75.70 ± 6.00 | 1.60 ± 1.00 | 24.50 ± 4.80 | Moderate |
| Iwasaki et al. ( | Japan | 38 | 79.00 ± 6.20 | 2.70 ± 1.50 | 22.40 ± 7.40 | Good |
| Author, Year | Hyphema | IOP spike |
|---|---|---|
| Total |
|
|
| GATT ± PEI |
|
|
| Hepşen et al. ( | 20 | 1 |
| Aktas et al. ( | 36 | 15 |
| Gunay et al. ( | 65 | 21 |
| Sharkawi et al. ( | 103 | 25 |
| GATT |
|
|
| Gunay ( | 22 | 6 |
| GT |
|
|
| Tanihara et al. ( | 9 | 0 |
| GT + PEI |
|
|
| Fukuchi et al. ( | 30 | 10 |
| Koylu et al. ( | 3 | 8 |
| Honjo et al. ( | 3 | 11 |
| Iwasaki et al. ( | 6 | 9 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGlaucoma and retinal disorders · Retinal and Macular Surgery · Retinal Diseases and Treatments
Introduction
Glaucoma is the leading cause of irreversible blindness worldwide, and the number of glaucoma patients is expected to exceed 100 million by 2040 (1). Exfoliative glaucoma (XFG), a significant subtype, has a poorer prognosis than primary open-angle glaucoma (POAG), characterized by rapid progression, marked intraocular pressure (IOP) fluctuations, and more severe optic nerve damage at presentation (2, 3).
Lowering IOP remains the only effective strategy for slowing XFG progression. Medication often fails to achieve target levels, whereas traditional drainage procedures (e.g., trabeculectomy) carry high risks of complications (e.g., shallow anterior chamber, choroidal detachment) and long-term drainage-related complications (4).
In recent years, minimally invasive glaucoma surgery (MIGS) has emerged as a novel surgical approach bridging the gap between medical therapy and drainage procedures (5). MIGS offers advantages, including high safety, rapid recovery, a short operative time, and low complication rates, providing a new treatment option for glaucoma (6, 7). MIGS is typically combined with phacoemulsification. For patients with glaucoma and cataracts, combined surgery yields better visual acuity improvement and intraocular pressure reduction than cataract extraction alone.
This meta-analysis focuses on two specific MIGS procedures: goniotomy (GT) and gonioscopy-assisted transluminal trabeculotomy (GATT). GT involves a direct incision of the trabecular meshwork under gonioscopic guidance. GATT utilizes an illuminated microcatheter or a suture to circumferentially cannulate and tear through Schlemm’s canal, potentially offering a more extensive ablation of the outflow resistance (8–10).
Although GT and GATT’s efficacy in POAG is established, their effectiveness in XFG remains unclear (11, 12). Therefore, this study aimed to evaluate GT and GATT’s efficacy and safety for treating XFG through a systematic review and meta-analysis while comparing the therapeutic differences among various surgical approaches.
Methods
This meta-analysis adhered to the 2020 Preferred Reporting Items for Systematic Review and Meta-Analysis (PRISMA) guidelines and was registered in the PROSPERO database (registration number: CRD420251072295) on June 1, 2025. Two mutually blinded authors (W.L. and K.S.) independently conducted the title and abstract screenings and article assessment. The senior author (H.Z.) resolved disagreements.
Search strategy
The literature search encompassed five electronic databases: (1) PubMed; (2) Ovid; (3) Web of Science; (4) Scopus; and (5) Embase. The most recent search was conducted on June 13, 2025. The search strategy combined Medical Subject Headings (MeSH) terms and free-text terms related to the target population (e.g., “exfoliation glaucoma,” “pseudoexfoliation glaucoma”) and interventions [e.g., “goniotomy,” “trabeculotomy,” “Gonioscopy-assisted transluminal trabeculotomy (GATT)”]. Additionally, references from the retrieved articles were screened to identify further eligible studies.
Inclusion and exclusion criteria
The inclusion criteria were as follows: (1) the study subjects were diagnosed with exfoliation glaucoma; (2) the interventions included GT or GATT; and (3) the research outcomes included IOP, the number of AGMs, and complications, which can be directly obtained from the literature.
The exclusion criteria were as follows: (1) reviews, editorials, case reports, meta-analyses, letters, animal studies, guidelines, conference abstracts, and opinion articles lacking original data; (2) mixed glaucoma studies not reporting separate data for exfoliation glaucoma (XFG); (3) follow-up periods shorter than 1 year; (4) overlapping study populations; and (5) non-English-language literature.
Data collection
Two researchers independently extracted data via standardized Excel templates. The extracted data included the first author, publication year, study design, sample size, demographic characteristics (country, age, sex), follow-up duration, surgical instrument, mean ± SD of IOP, and number of AGMs. The primary outcomes were baseline and postoperative (1/6/12 months) IOP and the number of AGMs. All reported complications were documented. It is acknowledged that variations in measurement protocols (e.g., time of day for IOP assessment) exist across studies, which constitutes a source of clinical heterogeneity.
Quality assessment
The Newcastle–Ottawa Scale (NOS) was used to evaluate the quality of the included cohort studies, specifically for assessing participant selection, group comparability, and outcome measurement. Studies scoring between 7 and 9 were categorized as “High,” those scoring between 4 and 6 were deemed “fair,” and studies with scores below 3 were labelled “poor” (11).
Statistical analysis
STATA 18.0 was used for the meta-analysis. The mean differences and 95% confidence intervals (CIs) for preoperative versus postoperative IOP and the number of AGMs were calculated. Complications not explicitly reported were considered absent. Subgroup analyses were performed to compare surgical approaches and devices. Heterogeneity was assessed using the I^2^ statistic and Cochran’s Q test. A random-effects model was used if significant heterogeneity was present (I^2^ > 50% and Q-test p < 0.10); otherwise, a fixed-effects model was applied. Sensitivity analyses employed sequential exclusion methods, and publication bias was assessed via Egger’s test.
Results
Search characteristics
Initially, 4,837 potentially eligible studies were identified, and articles not meeting the specified eligibility criteria were excluded. Following the screening process, 14 articles involving a combined total of 624 eyes were selected for the final analysis.
Among these, 6 studies reported outcomes for GATT ± PEI, 2 for standalone GATT, 2 for standalone GT, and 4 for GT + PEI (Figure 1). The baseline characteristics of the included studies are shown in Table 1.
Flow chart of study selection. GT, goniotomy; GATT, gonioscopy-assisted transluminal trabeculotomy; XFG, exfoliation glaucoma; PEI, phacoemulsification with intraocular lens implantation.
Reduction of IOP and AGM
In the GATT ± PEI group, IOP decreased by 1.96 (p < 0.01), 2.17 (p < 0.001), and 2.07 (p < 0.001) at 1, 6, and 12 months post-operatively, respectively. The number of AGMs decreased by 3.28 (p < 0.001), 2.87 (p = 0.003), and 2.54 (p = 0.011) at 1, 6, and 12 months post-operatively, respectively.
In the GATT group, IOP decreased by 2.39 (p < 0.001), 2.52 (p = 0.711), and 2.65 (p = 0.821) at 1, 6, and 12 months post-operatively, respectively. The number of AGMs decreased by 3.11 (p < 0.001) and 3.94 (p < 0.001) at 6 and 12 months post-operatively, respectively.
In the GT group, the IOP decreased by 1.27 (p = 0.002), 1.57 (p = 0.002), and 1.23 (p = 0.492), respectively. AGM counts reduced by 1.00 (p < 0.001), 1.04 (p < 0.001), and 0.54 (p < 0.001) at 1, 6, and 12 months post-operatively, respectively.
In the GT + PEI group, the IOP decreased by 1.95 (p < 0.001), 2.00 (p = 0.040), and 2.13 (p = 0.013), respectively. AGM counts reduced by 1.07 (p < 0.001), 0.96 (p < 0.001), and 0.96 (p < 0.001) at 1, 6, and 12 months post-operatively, respectively (Figures 2, 3).
Forest plots showing postoperative and preoperative IOP at 1 (A), 6 (B), and 12 (C) months. CI, confidence interval.
Forest plots showing postoperative and preoperative the numbers of AGMs at 1 (A), 6 (B), and 12 (C) months. CI = confidence interval.
Influence of surgical device in the GATT ± PEI cohort
In the suture-based GATT subgroup, IOP decreased by 2.31 mmHg (p < 0.001) at 12 months postoperatively. AGM counts reduced by 2.76 (p = 0.008) at 12 months postoperatively.
In the microcatheter-based GATT subgroup, IOP decreased by 1.45 mmHg (p < 0.001) at 12 months postoperatively. AGM counts reduced by 2.16 (p < 0.001) at 12 months postoperatively (Figure 4).
Forest plots of subgroup analyses comparing surgical devices (suture vs. microcatheter) for GATT procedures within the GATT ± PEI cohort. (A) Mean difference in intraocular pressure (IOP) reduction from baseline at 12 months postoperatively. (B) Mean difference in the number of antiglaucoma medications (AGMs) reduced from baseline at 12 months postoperatively.
Safety
Table 2 shows the most common complications. Among the 624 eyes, 297 (47.6%) developed anterior chamber hemorrhage, and 106 (17.0%) experienced an IOP spike. The GATT± PEI group had a higher incidence of anterior chamber hemorrhage (35.8% of total eyes) and a higher incidence of IOP spike (9.9% of total eyes).
Publication bias and sensitivity analysis
Given the significant heterogeneity in the IOP and AGM analyses, postoperative 12-month IOP outcomes were used as a sensitivity analysis indicator. According to Egger’s test, no publication bias existed in the studies that were reported (p = 0.310). Sensitivity analysis showed that deleting any one study would not change the significance of the results, which indicates the stability of the meta-analysis (Figure 5).
The sensitivity analysis result.
Discussion
MIGS for treating exfoliation glaucoma has gained increasing attention (5, 12–24). This study comprehensively evaluated the efficacy and safety of goniotomy (GT) and gonioscopy-assisted transluminal trabeculotomy (GATT) in treating exfoliation glaucoma (XFG) through a systematic review and meta-analysis. The pooled analyses demonstrated significant reductions in both IOP and medication use across the studied procedures.
Subgroup analysis compared the efficacy of different surgical methods. The results indicate that procedures combined with phacoemulsification (GATT ± PEI and GT + PEI) demonstrated significant and sustained IOP reduction throughout the 12-month follow-up. While the standalone procedures (GATT and GT) significantly reduced the number of medications, the evidence for long-term IOP reduction was less consistent. Specifically, for standalone GATT, while a significant IOP reduction was observed at 1 month, the reductions at 6 and 12 months did not reach statistical significance in our model (p > 0.05). This suggests that the long-term IOP-lowering efficacy of standalone GATT in XFG remains uncertain based on current evidence and requires further investigation. The more consistent results observed in the combined surgery groups suggest that coupling GATT or GT with phacoemulsification may provide more stable IOP control for XFG patients with concurrent cataract.
Although GATT covers a wider range than GT, our subgroup analysis showed that in the combined surgery group, the magnitude of IOP reduction was not significantly different between GATT ± PEI and GT + PEI at 12 months. Previous studies comparing the efficacy of trabeculotomy with or without PEI for POAG across different incision angles reported similar IOP control outcomes for 120°, 240°, and 360° incisions, which is consistent with the present findings (25, 26).
When comparing the two primary devices used for GATT within the GATT ± PEI cohort, suture-based procedures were associated with a statistically greater reduction in IOP at 12 months compared to microcatheter-based procedures (between-subgroup p = 0.005). This suggests that the mechanical properties of the suture may facilitate a more complete or consistent trabeculotomy, potentially leading to enhanced aqueous outflow in eyes with XFG. However, this interpretation must be treated with considerable caution. The microcatheter subgroup contained only a single study, and the suture subgroup exhibited considerable heterogeneity, indicating other unmeasured factors (e.g., surgeon experience) are also influential. Therefore, while this finding highlights surgical device as a potentially critical variable for optimization, it remains hypothesis-generating. Future prospective studies or randomized trials designed to directly compare these devices are warranted to confirm this observed difference and guide surgical technique selection.
In the results on complications, the overall incidence of anterior chamber hemorrhage was 47.6%, which is similar with previous studies of MIGS for primary angle-closure glaucoma (PACG) (27). Notably, the GATT± PEI group presented a greater incidence of anterior chamber hemorrhage, possibly due to increased exposure of the collection duct and scleral venous connections during this procedure (28). This group also presented a greater incidence of IOP spike than did the other group. This could be caused by corticosteroid-induced IOP spike, postoperative opening of the trabecular meshwork and Schlemm’s canal walls, and a greater contact area between corticosteroids and target cells, leading to resistance in aqueous outflow in steroid-sensitive patients (29–31).
This study has several limitations. First, the majority of the included studies were observational cohort designs rather than randomized controlled trials (RCTs). This predominance of lower-level evidence limits the strength of our conclusions, as non-random assignment in these studies is prone to selection bias and confounding. Therefore, the findings should be interpreted as representing effectiveness in real-world settings, with the need for confirmation from future high-quality RCTs. Second, Over 60% of the included eyes were from studies conducted in Turkey. Given the known geographic variation in the epidemiology and phenotypic expression of exfoliation syndrome, the findings from this predominantly Turkish cohort may not be fully generalizable to other populations with potentially different risk profiles and disease courses. This limits the external validity of our pooled results. Third, surgical technique heterogeneity (e.g., resection extent, combined cataract surgery) could not be fully explained by subgroup analysis. Fourth, significant variation in follow-up durations across studies limited the assessment of long-term efficacy. Finally, Variations in the timing of IOP measurements (which typically ignored diurnal variation) may introduce measurement bias and affect the precision and comparability of the pooled estimates.
Conclusion
This systematic review and meta-analysis demonstrated that angle-based MIGS (GT and GATT), particularly when combined with phacoemulsification, can safely and effectively reduce IOP and medication use in XFG. However, the evidence for sustained IOP lowering with standalone GATT is limited, highlighting the need for further research and careful patient selection.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Barkana Y Dorairaj S. Re: Tham et al.: global prevalence of glaucoma and projections of glaucoma burden through 2040: a systematic review and meta-analysis (ophthalmology 2014;121:2081-90). Ophthalmology. (2015) 122:e 40–1. doi: 10.1016/j.ophtha.2014.11.03024974815 · doi ↗ · pubmed ↗
- 2Plateroti P Plateroti AM Abdolrahimzadeh S Scuderi G. Pseudoexfoliation syndrome and Pseudoexfoliation Glaucoma: a review of the literature with updates on surgical management. J Ophthalmol. (2015) 2015:370371. doi: 10.1155/2015/370371, 26605078 PMC 4641922 · doi ↗ · pubmed ↗
- 3Ritch R Schlötzer-Schrehardt U. Exfoliation syndrome. Surv Ophthalmol. (2001) 45:265–315. doi: 10.1016/s 0039-6257(00)00196-x 11166342 · doi ↗ · pubmed ↗
- 4Gedde SJ Schiffman JC Feuer WJ Herndon LW Brandt JD Budenz DL. Treatment outcomes in the tube versus trabeculectomy (TVT) study after five years of follow-up. Am J Ophthalmol. (2012) 153:789–803.e 2. doi: 10.1016/j.ajo.2011.10.02622245458 PMC 4460598 · doi ↗ · pubmed ↗
- 5Aktas Z Ozdemir Zeydanli E Uysal BS Yigiter A. Outcomes of prolene gonioscopy assisted transluminal trabeculotomy in primary open angle Glaucoma and pseudoexfoliation Glaucoma: a comparative study. J Glaucoma. (2022) 31:751–6. doi: 10.1097/ijg.000000000000206335696703 · doi ↗ · pubmed ↗
- 6Seibold LK Soohoo JR Ammar DA Kahook MY. Preclinical investigation of ab interno trabeculectomy using a novel dual-blade device. Am J Ophthalmol. (2013) 155:524–9.e 2. doi: 10.1016/j.ajo.2012.09.02323218696 · doi ↗ · pubmed ↗
- 7Tanito M Matsuo M. Ab-interno trabeculotomy-related glaucoma surgeries. Taiwan J Ophthalmol. (2019) 9:67–71. doi: 10.4103/tjo.tjo_38_19, 31198665 PMC 6557068 · doi ↗ · pubmed ↗
- 8Richter GM Coleman AL. Minimally invasive glaucoma surgery: current status and future prospects. Clin Ophthalmol. (2016) 10:189–206. doi: 10.2147/opth.S 8049026869753 PMC 4734795 · doi ↗ · pubmed ↗