Therapeutic methods and effect on keloid and hypertrophic scars: a systematic review
Yuhang Shen, Lirong Yang, Dayong Feng, Chunhui Wang, Zhiyong Bai, Xi Wang, Jingwen Wang, Yuening Feng, Ayue An

TL;DR
This paper reviews current and emerging treatments for keloids and hypertrophic scars, highlighting combination therapies as more effective than single treatments.
Contribution
The study systematically evaluates a wide range of therapies, including innovative approaches like RNA microneedles and stem cells, for fibroproliferative scar disorders.
Findings
Combination therapies show better outcomes than single-modality treatments in reducing scar recurrence and improving prognosis.
Corticosteroid injections and surgical excision remain key benchmarks despite no definitive treatment standard.
Anti-fibroblast growth strategies are essential for effective scar management.
Abstract
Keloids and hypertrophic scars are fibroproliferative disorders with high recurrence rates, lacking a definitive treatment standard. This review systematically evaluates current therapies and their effectiveness in treating keloid and hypertrophic scars. The inclusion criteria were based on the population, intervention, comparator, outcomes, and study design (PICOS) framework. Electronic searches through April 2025 across databases such as PubMed, EMBASE, Cochrane Library, and Web of Science used keywords such as ‘keloid’, ‘occlusive dressings’, and ‘imiquimod’, among others. Meanwhile, we used the keywords ‘Antigens, CD’ and ‘MicroRNAs’ to search for molecular mechanisms associated with keloid and hypertrophic scars. The Risk of Bias 2 (RoB2) and Methodological Index for Non-Randomized Studies (MINORS) checklists were used to assess the quality of the included studies and potential…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
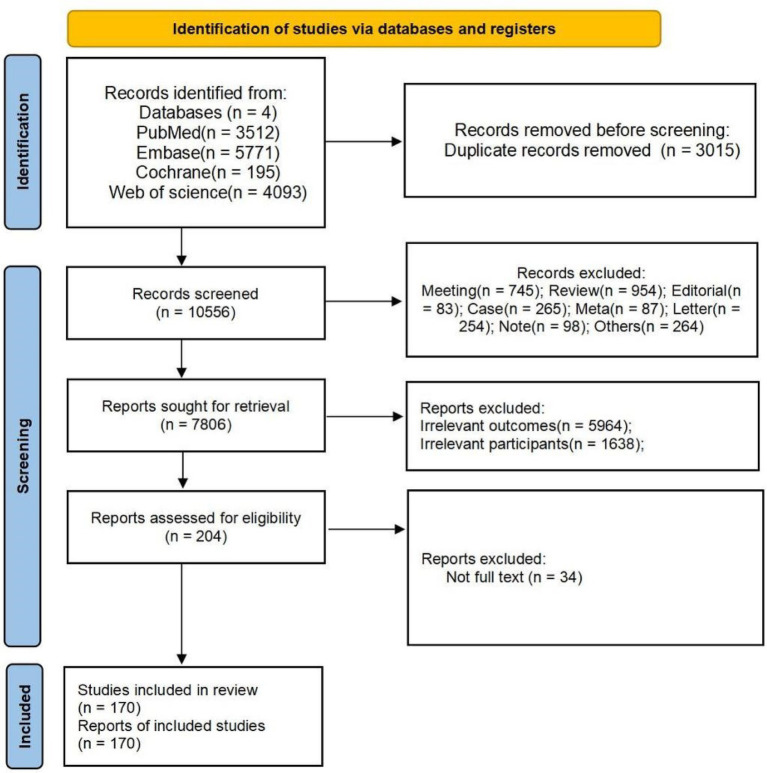 Figure 1
Figure 1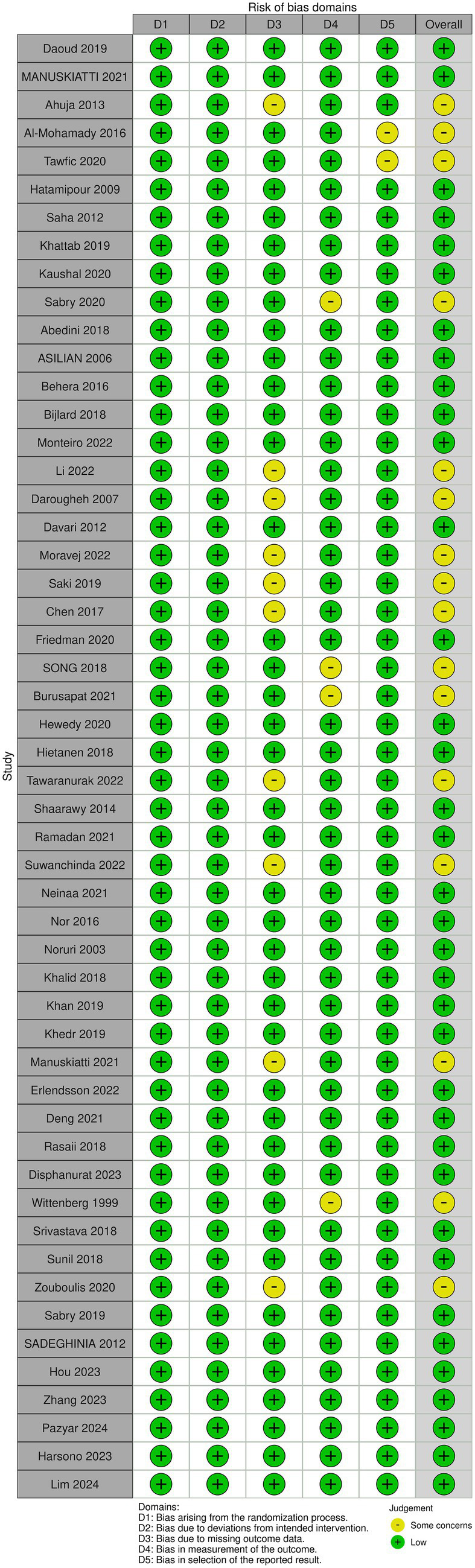 Figure 2
Figure 2| Study | Country | Study design | Patients | Sample size | Age | Intervention of the experimental group | Intervention of the controlled group | Follow up |
|---|---|---|---|---|---|---|---|---|
| Daoud 2019 ( | USA | RCT | Large (>100 cm2) hypertrophic scars | 23 s | \ | Combined Intense Pulsed Light (IPL) With Fractional CO2-Laser | Fractional CO2-Laser | 6 months |
| Manuskiatti 2021 ( | USA | RCT | Abdominal hypertrophic scars | 19 | 34 | Laser+steroid | Laser + petrolatum | 6 months |
| Son 2014 ( | Korea | Cohort study | Keloids or hypertrophic scars | 12 | 34.5 | 578 nm Copper Bromide Laser Combined with Intralesional Corticosteroid Injection | \ | 1 month |
| Lee 2015 ( | Korea | Cohort study | Keloids or hypertrophic scars | 30 | 23.9 | 6-MeV electron beam | \ | 27.4 months |
| Ahuja 2013 ( | India | RCT | Keloids or hypertrophic scars | 40 | \ | Intralesional verapamil hydrochloride (concentration 2.5 mg/mL) | Intralesional triamcinolone acetonide (concentration 40 mg/mL) | \ |
| Martin-Garcia 2005 ( | USA | Cohort study | Earlobe Keloid | 6 | 20.17 | Imiquimod 5% Cream | \ | 2 years |
| Al-Mohamady 2016 ( | Egypt | RCT | Keloids or hypertrophic scars | 20 | 22.6 | 595-nm PDL laser | Nd: YAG laser | 1 month |
| Tawfic 2020 ( | Egypt | RCT | Hypertrophic Scars and Keloids | 30 | 25.97 | Combined: Fractional and Nd YAG | Nd: YAG alone/Fractional laser alone | 1 month |
| Kant 2018 ( | Netherlands | Retrospective study | Hypertrophic and keloid scars | 58 | 28.1 | Triamcinolone and verapamil | \ | \ |
| Li 2020 ( | China | Prospective study | Hypertrophic scars and keloids | 21 | 28.43 | Intralesional 1,470 nm bare-fiber diode laser | \ | \ |
| Wen 2021 ( | China | Retrospective study | Keloids | 100 | 28 | Hypofractionated radiotherapy | \ | 4.92 years |
| Hatamipour 2009 ( | Iran | RCT | Keloids | 50 | \ | combined topical silicone and 5-Fluorouracil | Topical silicone | 1 year |
| Saha 2012 ( | India | RCT | Keloids | 44 | 33.75 | 5-FU (50 mg/mL) | Triamcinolone acetonide (40 mg/mL) | 1 year |
| Daurade 2020 ( | France | Retrospective study | Keloids | 38 | \ | Combining surgical excision and high-dose-rate brachytherapy | \ | 6 months |
| Chen 2020 ( | China | Cohort study | Keloids | 40 | 27.1 | Continuous tension reduction | \ | 2 years |
| Wang 2020 ( | China | Cohort study | Keloids | 41 | 27.4 | combined Ultrapulse Fractional Carbon Dioxide Laser and Topical Triamcinolone | \ | 2 years |
| Levenberg 2020 ( | Israel | Cohort study | Keloids | 21 | \ | Intralesional 5FU and corticosteroids | \ | 3 months |
| Khattab 2019 ( | Egypt | RCT | Keloids | 40 | 31.55 | Intralesional verapamil alone 2.5 mg/mL. | Combination of PDL and intralesional verapamil alone 2.5 mg/mL | 6 months |
| Bonnardeaux 2019 ( | Canada | Cohort study | Keloids | 21 | \ | Surgical excision combined with fully ablative carbon dioxide laser therapy and triamcinolone injections | \ | 18 months |
| Seo 2011 ( | Korea | Cohort study | Keloids and hypertrophic scars | 9 | 44.11 | Topical and intralesional mitomycin C (1 mg/mL) | \ | 6 months |
| Arnault 2009 ( | France | Cohort study | Keloids | 55 | \ | Iridium 192* brachytherapy | \ | \ |
| Yii 1996 ( | England | Cohort study | Keloids and hypertrophic scars | 41 | \ | Cynthaskin and topical steroid | \ | \ |
| Bijlard 2017 ( | Netherlands | Cohort study | Keloids | 238 | \ | High-Dose-Rate Brachytherapy | \ | \ |
| Kaushal 2020 ( | India | RCT | Keloids | 60 | 33.57 | Combined intralesional radiofrequency and intralesional triamcinolone acetonide | Intralesional triamcinolone acetonide alone | \ |
| Sabry 2020 ( | Egypt | RCT | Hypertrophic scars and keloids | 20 | 12.5 | combined laser and intralesional injection of botulinum toxin A | Intralesional injection of botulinum toxin A | \ |
| Bischof 2007 ( | Germany | Cohort study | Keloids | 47 | 36.6 | 6-MeV electron beam radiotherapy | \ | 5.8 years |
| Francisco 2013 ( | Spain | Cohort study | Keloids | 10 | 25.7 | Combination of bleomycin and triamcinolone acetonide | \ | \ |
| Cho 2010 ( | Korea | Cohort study | Keloids and hypertrophic scars | 12 | 23.8 | 1,064-nm Q-switched Nd: YAG laser with low fluence | \ | 3 months |
| Chopinaud 2014 ( | France | Retrospective study | Keloids | 10 | \ | Intralesional Cryosurgery | \ | \ |
| Clavere 1997 ( | France | Cohort study | Keloids | 39 | \ | Iridium 192 brachytherapy | \ | \ |
| Abedini 2018 ( | Iran | RCT | Keloids and hypertrophic scars | 50 | \ | Intralesional verapamil (2.5 mg/mL) | Intralesional corticosteroids (40 mg/mL) | 3 months |
| Copcu 2004 ( | Turkey | Cohort study | Keloids | 21 | 20.61 | Combination of Surgery and Intralesional Verapamil Injection | \ | 2 years |
| Careta 2013 ( | Brazil | Cohort study | Keloids | 12 | 20.08 | Shaving, Cryosurgery, and Intralesional Steroid Injection | \ | \ |
| Asilian 2006 ( | Iran | RCT | Keloids | 69 | 24.73 | Combination of Triamcinolone, 5-Fluorouracil, and Pulsed-Dye Laser | Intralesional triamcinolone acetonide (10 mg/mL)/TAC (40 mg/mL) + 5-FU (50 mg/mL) | 3 months |
| Behera 2016 ( | India | RCT | Keloids | 60 | \ | Carbon Dioxide Laser | Cryotherapy | 1 year |
| Carvalhaes 2015 ( | Brazil | Cohort study | Earlobe keloids | 46 | \ | Triamcinolone injections, surgical resection, and local pressure | \ | 2 years |
| Espana 2001 ( | Spain | Cohort study | Keloids and hypertrophic scars | 13 | 23.85 | Bleomycin | \ | \ |
| Weshahy 2012 ( | Egypt | Cohort study | Keloids and hypertrophic scars | 22 | \ | Combined intralesional cryosurgery and intralesional steroid injection | \ | 4 months |
| Manjunath 2021 ( | India | Cohort study | Keloids | 50 | \ | Surgical Excision and Adjuvant High-dose Rate Brachytherapy | \ | 6 months |
| Bijlard 2018 ( | Netherlands | RCT | Keloids | 26 | 33.78 | Intralesional cryotherapy | Excision with corticosteroid injections or brachytherapy | \ |
| Alhamzawi 2021 ( | Iraq | Cohort study | Keloids | 24 | 24.25 | Fractional Carbon Dioxide Laser with Intralesional 5-Fluorouracil (50 mg/mL) | \ | \ |
| Erol 2008 ( | Turkey | Cohort study | Keloids and hypertrophic scars | 109 | \ | Intense Pulsed Light | \ | \ |
| Monteiro 2022 ( | India | RCT | Keloids | 30 | \ | Intralesional 5 Fluorouracil (50 mg/mL) | Combination of 5 Fluorouracil (50 mg/mL) with Triamcinolone Acetonide (40 mg/mL) | 6 months |
| Escarmant 1993 ( | USA | Cohort study | Keloids | 544 | 24 | Iridium 192 interstitial irradiation after surgical excision | \ | 6 years |
| Annabathula 2017 ( | India | Cohort study | Keloids | 15 | \ | Fractional Carbon Dioxide, Long Pulse Nd: YAG and Pulsed Dye Laser | \ | \ |
| Berman 2020 ( | USA | Retrospective study | Keloids | 61 | 38.9 | Superficial Radiation Therapy | \ | 2 years |
| Li 2022 ( | China | RCT | Keloids | 60 | 29.49 | Excision followed by 5-FU and betamethasone intralesional injections | 5-FU and betamethasone intralesional injections/excision followed by radiotherapy | 8–12 months |
| Barragan 2022 ( | Spain | Cohort study | Keloids | 51 | 46 | Interstitial high-dose-rate brachytherapy | \ | 4 years |
| Jiang 2015 ( | Germany | Prospective study | Keloids | 24 | \ | Interstitial high-dose-rate brachytherapy | \ | \ |
| Jiang 2017 ( | Germany | Cohort study | Keloids | 29 | \ | Interstitial high-dose-rate brachytherapy | \ | 4.14 years |
| Guix 2001 ( | Spain | Cohort study | Keloids | 169 | \ | Interstitial high-dose-rate brachytherapy | \ | 7 years |
| Hafkamp 2017 ( | Netherlands | Prospective study | Therapy-resistant keloids | 24 | Interstitial high-dose-rate brachytherapy | \ | 2.21 years | |
| Meymandi 2014 ( | Iran | Cohort study | Keloids | 86 | \ | Intense Pulsed Light Method Along With Corticosteroid Injection | \ | \ |
| Stephanides 2011 ( | England | Cohort study | Refractory Keloids | 99 | \ | Intralesional triamcinolone (10 mg or 40 mg/dL) and pulsed dye laser | \ | \ |
| Choi 2020 ( | Korea | Cohort study | Auricular keloid | 18 | 26.5 | Triamcinolone acetonide intralesional injection | \ | 2 years |
| Darougheh 2007 ( | Iran | RCT | Keloids and hypertrophic scars | 40 | 24.3 | Intralesional triamcinolone acetonide | Combination of TAC and 5-fluorouracil | 3 months |
| Davari 2012 ( | Iran | RCT | Keloids and hypertrophic scars | 7 | 30.29 | Pulsed dye laser | 9 weeks after suture removal | \ |
| Muneuchi 2009 ( | Japan | Cohort study | Keloids | 94 | 42 | Intralesional injection of triamcinolone acetonide | \ | 5 years |
| Kim 2015 ( | Korea | Cohort study | Keloids and hypertrophic scars | 52 | \ | intense pulsed light device and intralesional corticosteroid injection | \ | \ |
| Kim 2022 ( | Korea | Retrospective study | Hypertrophic cesarean section scars | 35 | 34.91 | pulsed dye laser therapy combined with intralesional triamcinolone injection | \ | 7.74 months |
| Moravej 2022 ( | Iran | RCT | Keloids and hypertrophic scars | 60 | 33.95 | Intralesional bleomycin (1.5 mg/mL) | Intralesional triamcinolone (20 mg/mL) | \ |
| Saki 2019 ( | Iran | RCT | Keloids | 15 | \ | Intralesional Triamcinolone Acetonide | Intralesional Verapamil | 6 months |
| George 2005 ( | Greece | Cohort study | Keloids | 20 | 30.05 | Intralesional 5-fluorouracil | \ | 2 years |
| Hye 2015 ( | Korea | Cohort study | Hypertrophic Thyroidectomy Scar | 67 | 37 | Copper bromide laser and intralesional triamcinolone injection (2.5 mg/mL or 5 mg/mL) | \ | \ |
| Maemoto 2020 ( | Japan | Cohort study | Keloids | 59 | \ | Electron beam radiation therapy | \ | 10 years |
| Berman 2002 ( | USA | Cohort study | Keloids | 12 | \ | Imiquimod 5% cream | \ | 6 months |
| Chen 2017 ( | China | RCT | Keloids | 39 | 26.73 | Intralesional injection of diprospan (2 mg betamethasone disodium phosphate and 5 mg betamethasone dipropionate in 1 mL) | Intralesional injection of diprospan with a combination of 0.5 mL 5-fluorouracil (25 mg/mL)/diprospan + 5-FU + 1,064-nm Nd: YAG laser | \ |
| Ogawa 2002 ( | Japan | Retrospective study | Keloids and hypertrophic scars | 147 | \ | Electron beam radiation therapy | \ | 18 months |
| Friedman 2020 ( | Israel | RCT | Surgical scars | 11 | 47.2 | Erbium glass, 1,540 nm laser | not treated | 1 year |
| Aljodah 2021 ( | Iraq | Cohort study | Recurrent Auricular Keloid | 41 | 29 | Combination of Surgical Excision and Perioperative Corticosteroid Injection (40 mg/mL) | \ | 13.04 months |
| Park 2012 ( | Korea | Cohort study | Facial Keloids | 15 | 34 | Intralesional Steroid Injections (20 mg/mL) | \ | 18 months |
| Acosta 2016 ( | Chile | prospective study | Keloids | 21 | 12 | Intralesional Triamcinolone (40 mg/mL) | \ | 5.58 years |
| Ogawa 2014 ( | Japan | Retrospective study | Auricular Keloid | 57 | \ | Surgical excision and radiotherapy | \ | 18 months |
| Ollstein 1981 ( | USA | Cohort study | Keloids | 40 | \ | Combined surgical excision and immediate X-ray therapy | \ | 2 years |
| Reinholz 2020 ( | Germany | Cohort study | Keloids | 25 | 28.68 | Intralesional 5-fluorouracil (50 mg/mL) in combination with triamcinolone acetonide (40 mg/mL) | \ | 1 year |
| SONG 2018 ( | China | RCT | Keloids | 240 | \ | hyperbaric oxygen therapy | Surgical excision and radiotherapy | \ |
| Song 2014 ( | Korea | Cohort study | Intractable keloids | 12 | 32 | Single-fraction radiotherapy | \ | 20 months |
| Burusapat 2021 ( | Thailand | RCT | Auricular Keloid | 34 | 25.52 | Immediate Triamcinolone Acetonide Injection | Delayed Triamcinolone Acetonide Injection | 6 months |
| Shen 2015 ( | China | Cohort study | Keloids | 568 | \ | Hypofractionated electron-beam radiation | \ | 40 months |
| Ragoowansi 2002 ( | England | Cohort study | Keloids | 80 | \ | Surgical Excision and immediate single-fraction radiotherapy | \ | 5 years |
| Hewedy 2020 ( | Egypt | RCT | Keloids | 40 | 29.05 | Intralesional triamcinolone acetonide (20 mg/mL) and Platelet rich plasma | TA (20 mg/mL) alone | 3 months |
| Hietanen 2018 ( | Finland | RCT | Keloids | 43 | 42 | Intralesional triamcinolone | 6 months | |
| Weshay 2015 ( | Egypt | Cohort study | Keloids | 18 | 32.78 | Combination of Radiofrequency and Intralesional Steroids (10 mg/mL) | \ | 5 years |
| Agbenorku 2000 ( | Ghana | Cohort study | Keloids | 120 | \ | A triple therapy comprising the use of steroid injections and cream (triamcinolone acetonide), surgery, and silicone gel strip/sheet pressure application | \ | 13 months |
| Ahmad 2017 ( | Pakistan | Cohort study | Keloids | 51 | 22.82 | Iridium-192 high-dose rate surface mould brachytherapy | \ | 33 months |
| Saray 2005 ( | Turkey | Cohort study | Keloids and hypertrophic scars | 14 | 32.57 | Dermojet injections of bleomycin (1.5 IU/mL) | \ | 19 months |
| Tawaranurak 2022 ( | Thailand | RCT | Keloids | 22 | 43.7 | Treated with fractional CO2 laser + topical triamcinolone | Intralesional TA | 1 year |
| Sruthi 2017 ( | India | Cohort study | Keloids | 13 | \ | Single-fraction radiation | \ | 32.67 months |
| Son 2020 ( | USA | Cohort study | Keloids | 15 | 43.87 | A single dose of low-energy superficial X-ray radiation | \ | 6 months |
| Shaarawy 2014 ( | Egypt | RCT | Keloids | 24 | 29.29 | Intralesional botulinum toxin type A | Intralesional steroid | 7 months |
| Song 2018 ( | China | Cohort study | Keloids | 108 | \ | Intralesional triamcinolone acetonide injection | \ | \ |
| Ramadan 2021 ( | Egypt | RCT | Keloids and hypertrophic scars | 40 | \ | Pulsed Nd: YAG laser and intralesional bleomycin | Pulsed Nd: YAG laser only | \ |
| Suwanchinda 2022 ( | Thailand | RCT | keloids and hypertrophic scars | 18 | Cold atmospheric-pressure plasma | Untreated | 1 month | |
| Luo 2023 ( | China | Cohort study | Treating refractory keloids and hypertrophic scars | 86 | \ | The combined application of bleomycin and triamcinolone | \ | 2–5 years |
| Neinaa 2021 ( | Egypt | RCT | Keloids | 60 | 25 | Intralesional injection of botulinum toxin type-A (5 IU/injection point) | Intralesional injection of platelet rich plasma (0.1 mL/injection point)/intralesional injection of triamcinolone acetonide (20 mg/session) | \ |
| Nor 2016 ( | Malaysia | RCT | Keloids | 21 | 29 | Either daily topical clobetasol propionate 0.05% cream under occlusion with a silicone dressing | Monthly intralesional triamcinolone injection | 3 months |
| Noruri 2003 ( | USA | RCT | Surgical scars | 11 | 60.18 | 585-nm pulsed dye laser | Not treated | 1 month |
| Khalid 2018 ( | Pakistan | RCT | Ear keloids | 60 | 31.82 | Intralesional 5-FU/triamcinolone acetonide injections | Radiotherapy | 6 months |
| Khan 2019 ( | Pakistan | RCT | Keloids | 164 | 32.5 | Intralesional bleomycin | Intralesional triamcinolone | 6 months |
| Khedr 2019 ( | Egypt | RCT | Hypertrophic scars | 50 | 16.64 | Nd: YAG laser | combined intense pulsed light and radiofrequency | 3 months |
| Stern 1989 ( | USA | Prospective study | Earlobe Keloids | 18 | \ | Carbon dioxide laser excision | \ | \ |
| Stewart 2006 ( | USA | Retrospective study | Head and neck keloids | 10 | 21 | The combination of surgical excision with the application of topical mitomycin-C | \ | 8 months |
| Leeuwen 2014 ( | Netherlands | Prospective study | Keloids | 27 | \ | Intralesional Cryotherapy | \ | 1 year |
| Viani 2009 ( | Brazil | Retrospective study | Keloids | 612 | 25 | Strontium 90 brachytherapy | \ | 61 months |
| Manuskiatti 2021 ( | Thailand | RCT | Hypertrophic scars | 21 | 35.5 | Thermomechanical fractional injury-assisted topical corticosteroid (40 mg/mL) | Corticosteroid injection (40 mg/mL) | 6 months |
| Erlendsson 2022 ( | Denmark | RCT | Hypertrophic scars | 20 | \ | A pneumatic jet injection with 5-fluorouracil and triamcinolone acetonide | 5-FU + TAC | 1 month |
| Wang 2020 ( | China | Cohort study | Keloids | 58 | 33 | Combined surgical excision and electron external beam radiation | \ | 22 months |
| Davison 2009 ( | USA | Retrospective study | Keloids and hypertrophic scars | 102 | \ | 5-FU + steroid with excision | 5FU + steroid without excision/steroid treatment with excision | 6 years |
| Dai 2021 ( | China | Retrospective study | Keloids | 50 | 41 | Combination of ablative fractional carbon dioxide laser and platelet-rich plasma | Ablative fractional carbon dioxide laser | 6 months |
| Ang 2013 ( | Singapore | Retrospective study | Earlobe keloids | 16 | 20 | Carbon dioxide laser ablation | Cold steel debulking surgery | 2 years |
| Nishi 2022 ( | India | Cohort study | Keloids | 170 | \ | combination of cryotherapy with intralesional corticosteroid | A combination of fractional CO2 laser followed by topical corticosteroids | \ |
| Sharma 2021 ( | India | Cohort study | Small keloids | 40 | \ | Intralesional 5-FU and triamcinolone acetonide | Combination of intralesional bleomycin and triamcinolone acetonide | \ |
| Abdel-Meguid 2014 ( | Egypt | Cohort study | Keloids | 23 | 26.21 | Intralesional cryosurgery | Contact cryosurgery | \ |
| Lv 2021 ( | China | Prospective study | Hypertrophic scars | 68 | 40.76 | Ablative fractional CO2 laser surgery | Conventional surgery | \ |
| Meymandi 2016 ( | Iran | Cohort study | keloids and hypertrophic scars | 166 | 31.7 | Intense pulsed light | Cryotherapy | \ |
| Deng 2021 ( | Japan | RCT | Keloids | 31 | 24 | Intralesional triamcinolone (5 ml 1%) and 5-fluorouracil (0.6 ml 2.5%) injections and Strontium-90 brachytherapy | Intralesional triamcinolone (5 mL 1%) and 5-fluorouracil (0.6 mL 2.5%) injections | 14 months |
| Yosipovitch 2009 ( | Singapore | Cohort study | Keloids | 10 | 25.9 | Cryotherapy and steroid injection | Cryotherapy alone/Steroid injection | \ |
| Emad 2010 ( | Iran | Prospective study | Keloids | 28 | 28.85 | Surgical excision and radiotherapy | Cryotherapy and intralesional steroid | \ |
| Hoang 2016 ( | USA | Retrospective study | Keloids | 128 | \ | Interstitial high-dose rate brachytherapy | Excision alone/external beam radiotherapy | 3.5 years |
| Berman 1997 ( | USA | Cohort study | Keloids | 124 | \ | Interferon alfa-2b | Excision alone/injection with triamcinolone acetonide | \ |
| Albalat 2021 ( | Egypt | Cohort study | Keloids or hypertrophic scars | 160 | 32.25 | Intralesional triamcinolone (concentration 40 mg/mL) | Intralesional 5-fluorouracil (concentration 250 mg/5 mL)/intralesional verapamil (concentration 2.5 mg/mL)/intralesional platelet-rich plasma (2.4 mL) | \ |
| Payapvipapong 2014 ( | Thailand | Cohort study | Keloids and hypertrophic scars | 26 | 34.43 | Intralesional triamcinolone acetonide (10 mg/mL) | Intralesional bleomycin (1 mg/mL) | 3 months |
| Rasaii 2018 ( | Iran | RCT | Keloids | 20 | 23.3 | Intralesional triamcinolone (40 mg/mL) in combination with botulinium toxin A (20 mg/mL) | Intralesional triamcinolone (40 mg/mL) alone | 1 month |
| Disphanurat 2023 ( | Thailand | RCT | Keloids and hypertrophic scars | 20 | 34.25 | Triamcinolone acetonide-loaded dissolving microneedle patch | Drug-free DMN patch | 1 month |
| Dina 2021 ( | Egypt | Cohort study | Keloids | 30 | 26.4 | combined fractional ablative 2,940 nm Er: YAG laser and topical application of steroid cream | Intralesional corticosteroid injection | \ |
| Wittenberg 1999 ( | USA | RCT | Hypertrophic scars | 20 | 48.9 | 585-nm flashlamp-pumped pulsed-dye laser | Silicone gel sheeting | 4 months |
| Srivastava 2018 ( | India | RCT | Keloids | 60 | 27.93 | Intralesional triamcinolone acetonide (40 mg/mL) and 5-fluorouracil (50 mg/mL) | Intralesional triamcinolone acetonide (40 mg/mL)/intralesional 5-fluorouracil (50 mg/mL) | 6 weeks |
| Sunil 2018 ( | India | RCT | Keloids | 60 | 30.85 | Fractional CO2 laser | Intralesional triamcinolone (40 mg/mL)/intralesional verapamil (2.5 mg/ mL) | \ |
| Zouboulis 2020 ( | Germany | RCT | Small keloids | 40 | 23.5 | Combined liquid nitrogen contact cryosurgery with intralesional corticosteroids | Liquid nitrogen contact cryosurgery | 3 years |
| Stromps 2013 ( | Israel | Retrospective study | Refractory keloids | 64 | 34.68 | Intralesional cryotherapy combined with postoperative silicone gel sheeting | Intralesional cryotherapy alone | 1 year |
| Alexander 2018 ( | India | Cohort study | Keloids and hypertrophic scars | 50 | \ | Fractional CO2 laser with intralesional steroid | Intralesional steroid alone | \ |
| Sabry 2019 ( | Egypt | RCT | Keloids and hypertrophic scars | 30 | 19.75 | CO2 laser and topically applied 5-FU | CO2 laser and topically applied verapamil hydrochloride/ablative fractional CO2 laser monotherapy | \ |
| Sadeghinia 2012 ( | Iran | RCT | Keloids | 40 | \ | Intralesional triamcinolone acetonide | 5-FU tattooing | 11 months |
| Gamil 2019 ( | Egypt | Cohort study | Keloids | 50 | 28.11 | Combined intralesional triamcinolone acetonide with botulinum toxin type A | Intralesional triamcinolone acetonide/intralesional botulinum toxin type A | 1 month |
| Dogahe 2023 ( | Iran | Cohort study | Keloids | 43 | 36.09 | Intralesional triamcinolone (40 mg/mL) and verapamil (2.5 mg/mL) | Intralesional triamcinolone alone (40 mg/mL) | 3 months |
| Shin 2019 ( | Korea | Cohort study | Keloids and hypertrophic scars | 38 | 39.52 | Combination of non-ablative fractional laser and intralesional triamcinolone injection | Intralesional triamcinolone injection | \ |
| Sharma 2007 ( | India | Cohort study | Small keloids | 21 | \ | combination of liquid nitrogen and intralesional triamcinolone acetonide (5 mg/mL) | Liquid nitrogen alone | 6 months |
| Gamil 2018 ( | Egypt | Cohort study | Acne keloidalis nuchae | 30 | 36.87 | Er: YAG laser | Long-pulsed Nd: YAG laser | \ |
| Cicco 2013 ( | Italy | Cohort study | Keloids | 96 | \ | High-dose-rate interstitial brachytherapy | Low-dose-rate interstitial brachytherapy | 2.33 years |
| Chernoff 2007 ( | USA | Cohort study | Keloids and hypertrophic scars | 30 | \ | Dermatix gel | Silicone gel sheeting | \ |
| Tsai 2019 ( | Japan | Retrospective study | Hypertrophic Scars | 40 | 34.2 | Combination of 1,064-nm Neodymium-doped Yttrium Aluminum Garnet Laser and Steroid Tape | Steroid tape | 6 months |
| Tawfik 2019 ( | Egypt | Cohort study | Severe hypertrophic scars | 24 | 26 | combined 5-fluorouracil and fractional erbium YAG laser | Topical 5-fluorouracil cream | \ |
| Hou 2023 ( | China | RCT | Keloids | 72 | 28.75 | Punch excision combined with Intralesional steroid injection | Intralesional Steroid Injection alone | \ |
| Liu 2023 ( | China | Retrospective study | Keloids | 29 | 35.38 | combined Pulsed Dye Laser and triamcinolone acetonide | Triamcinolone acetonide | \ |
| Lee 2008 ( | Korea | Cohort study | Keloids | 19 | 24.6 | Triamcinolone acetonide intralesional injection + Interferon- | Triamcinolone acetonide intralesional injection | \ |
| Zawahry 2015 ( | Egypt | Cohort study | Hypertrophic burn scars | 11 | 30.8 | Fractional CO2 laser | Untreated | 3 months |
| Meseci 2019 ( | Turkey | Prospective study | Postcesarean scars | 61 | 31.28 | Topical corticosteroid ointment | Untreated | 6 months |
| Qiao 2017 ( | China | Cohort study | Earlobe Keloid | 160 | \ | Surgery combined with lucortriticod and electron irradiation group | 1 year | |
| Francesca 2010 ( | Italy | Cohort study | Facial Scars | 30 | 37 | Self-drying silicone gel | \ | |
| Zhou 2023 ( | China | Retrospective study | Hypertrophic Scars | 155 | 29.7 | Ablative fractional carbon dioxide laser +1 g triamcinolone external application | Ablative fractional carbon dioxide laser + 40 mg/mL triamcinolone intralesional injection | 1 month |
| Zhang 2023 ( | China | RCT | Hypertrophic Scars | 101 | 32 | Combined CO2 fractional laser and narrowband intense pulsed light | Intense pulsed light | 3 months |
| Li 2024 ( | China | Prospective study | Hypertrophic Scars | 118 | \ | Keloid-cross-flap surgery and radiotherapy | Keloid-cross-flap surgery and compression therapy | 3 months |
| Pazyar 2024 ( | Iran | RCT | Keloids | 22 | 35.23 | Intralesional vitamin D injection | Intralesional triamcinolone injection | 3 months |
| Khan 2025 ( | Pakistan | Retrospective study | Keloids | 17 | 41.5 | Surgical excision and radiotherapy | \ | 2 years |
| Jiang 2024 ( | China | Retrospective study | Keloids | 12 | 24.42 | fractional carbon dioxide laser + 5-aminolevulinic acid photodynamic therapy | \ | 6 months |
| Hu 2023 ( | China | Retrospective study | Keloids | 15 | \ | Surgical resection, ultra-reduced tension suture incision, and superficial radiation therapy | \ | 6 months |
| Yang 2025 ( | China | Retrospective study | Keloids | 67 | \ | Surgical resection + injection of triamcinolone and 5-fluorouracil + radiation therapy | \ | >1 year |
| Park 2024 ( | Korea | Retrospective study | Keloids | 111 | 35.18 | Intralesional triamcinolone + ND: YAG laser | Intralesional Triamcinolone | 1 year |
| Harsono 2023 ( | Indonesia | RCT | Keloids | 24 | 29.38 | Intralesional injection of umbilical cord Mesenchymal stem cells | Intralesional injection of triamcinolone acetonide | 4 months |
| Qiu 2025 ( | China | Retrospective study | Hypertrophic Scars | 42 | 26.59 | Manual fractional technology with CO2 laser combined with transdermal triamcinolone acetonide and 5-fluorouracil | \ | 6 months |
| Aristides 2024 ( | Mexico | Retrospective study | Keloids | 22 | 24.3 | combined continuous wave and repetitive fractionated CO2 laser | \ | 6 months |
| Lim 2024 ( | Singapore | RCT | Keloids | 32 | 43.6 | Small interfering RNA microneedle patches | Silicone sheets | 2 months |
| Study | Intervention of the experimental group | Intervention of the controlled group | Conclusion |
|---|---|---|---|
| Daoud 2019 ( | Combined Intense Pulsed Light (IPL) With Fractional CO2-Laser | Fractional CO2-laser | The experimental group had statistically significant improvement in both color and texture |
| Abdel-Meguid 2014 ( | Intralesional cryosurgery | Contact cryosurgery | Intralesional cryosurgery is superior to contact cryosurgery in terms of efficacy and safety |
| Abedini 2018 ( | Intralesional verapamil (2.5 mg/mL) | Intralesional corticosteroids (40 mg/mL) | Did not support verapamil’s capability in the treatment of keloid or hypertrophic scars |
| Acosta 2016 ( | Intralesional Triamcinolone (40 mg/mL) | \ | Triamcinolone acetonide is highly effective for the treatment of pediatric keloids. There is no relationship between clinical response and the factors evaluated, such as lesion location, etiology, and age of the keloid. |
| Agbenorku 2000 ( | A triple therapy comprising the use of steroid injections and cream (triamcinolone acetonide), surgery and silicone gel strip/sheet pressure application | \ | This is a tedious and time intensive procedure for both physician and patient. A quicker and more readily available method should be sought |
| Ahmad 2017 ( | Iridium-192 high-dose rate surface mould brachytherapy | \ | 10 Gy in a single fraction is therefore the most convenient and cost effective dose regimen for the management of keloid scars in developing countries like Pakistan |
| Ahuja 2013 ( | Intralesional verapamil hydrochloride (concentration 2.5 mg/mL) | Intralesional triamcinolone acetonide (concentration 40 mg/mL) | Verapamil can flatten the raised scars, with an extremely low cost and fewer adverse effects |
| Albalat 2021 ( | Intralesional triamcinolone (concentration 40 mg/mL) | Intralesional 5-fluorouracil (concentration 250 mg/5 mL)/intralesional verapamil (concentration 2.5 mg/mL)/intralesional platelet-rich plasma (2.4 mL) | Intralesional verapamil was reported to be the most effective therapy, and platelet-rich plasma was effective as intralesional triamcinolone acetonide with no serious side effects; 5-fluorouracil was less effective in treating keloids. |
| Alexander 2018 ( | Fractional CO2 laser with intralesional steroid | Intralesional steroid alone | Combination therapy with FCL and ILS was superior in efficacy when compared to ILS alone, in the treatment of keloids and HTS |
| Alhamzawi 2021 ( | Fractional Carbon Dioxide Laser with Intralesional 5-Fluorouracil (50 mg/mL) | \ | Combination therapy with an FCO2 laser and intralesional 5-FU showed a promising effect in the treatment of resistant keloids, with an acceptable safety profile and low recurrence rate. |
| Aljodah 2021 ( | Combination of Surgical Excision and Perioperative Corticosteroid Injection (40 mg/mL) | \ | Perioperative corticosteroid injections combined with surgical excision of auricular keloids are still a valid option in recurrent cases. |
| Al-Mohamady 2016 ( | 595-nm PDL laser | Nd: YAG laser | Pulsed-dye laser and long-pulsed Nd: YAG laser treatments for keloid and hypertrophic scars provide significant improvement with no significant difference between the modalities. |
| Ang 2013 ( | The carbon dioxide laser ablation | Cold steel debulking surgery | Both the CO2 laser ablation and cold steel surgery were equally useful in reducing the size of the earlobe keloids, but were not effective in preventing the regrowth of the keloids |
| Annabathula 2017 ( | Fractional Carbon Dioxide, Long Pulse Nd: YAG and Pulsed Dye Laser | \ | Lasers may have a synergistic effect when combined with other modalities of treatment, but cannot be used as monotherapy in the treatment of keloids. |
| Arnault 2009 ( | Iridium 192* brachytherapy | \ | The technique is efficient in preventing keloid recurrence and in treating the functional signs, but at the expense of an unaesthetic result |
| Asilian 2006 ( | Combination of Triamcinolone, 5-Fluorouracil, and Pulsed-Dye Laser | Intralesional triamcinolone acetonide (10 mg/mL)/TAC (40 mg/mL) + 5-FU (50 mg/mL) | The TAC + 5-FU + PDL combination appears to be the best approach for treating keloid and hypertrophic scars. |
| Barragan 2022 ( | Interstitial high-dose-rate brachytherapy | \ | The treatment of keloid scars with perioperative interstitial high-dose-rate brachytherapy achieved excellent results, with a recurrence rate of only 4.9% and excellent cosmetic outcomes |
| Behera 2016 ( | Carbon dioxide laser | Cryotherapy | Both CO2 laser and cryotherapy, when combined with ILTA, were found to be equally effective in treating keloids. |
| Berman 1997 ( | Interferon alfa-2b | excision alone/injection with triamcinolone acetonide | Postoperative TAC injections do not reduce the number of keloid recurrences. However, injection of keloid excision sites with IFN-c ~ 2b offers a therapeutic advantage over keloid excision. |
| Berman 2002 ( | Imiquimod 5% cream | \ | The recurrence rate of excised keloids treated with postoperative imiquimod 5% cream was lower than the recurrence rates previously reported in the literature. |
| Berman 2020 ( | Superficial Radiation Therapy | \ | SRT with a BED value of 30 Gy delivered to keloidectomy excision sites immediately following excision was well-tolerated and resulted in markedly fewer long-term recurrences than reported following keloidectomy alone. |
| Bijlard 2017 ( | High-Dose-Rate Brachytherapy | \ | After excision of resistant keloids, high-dose-rate brachytherapy with a biological equivalent dose of approximately 20 Gy is recommended, on the basis of low recurrence and complication rates |
| Bijlard 2018 ( | Intralesional cryotherapy | Excision with corticosteroid injections or brachytherapy | Intralesional cryotherapy is inferior to keloid excision followed by brachytherapy for resistant keloids. In primary keloids, intralesional cryotherapy reduced keloid volume |
| Bischof 2007 ( | 6-MeV electron beam radiotherapy | \ | Postoperative electron radiotherapy is well-tolerated and very effective in preventing keloid recurrence |
| Bonnardeaux 2019 ( | Surgical excision combined with fully ablative carbon dioxide laser therapy and triamcinolone injections | \ | The need for multimodal therapy with combined methods in order to achieve long-term remission |
| Burusapat 2021 ( | Immediate triamcinolone acetonide injection | Delayed triamcinolone acetonide injection | Immediate TA injection is an acceptable option for the treatment of auricular keloids. Here, it was associated with a lower recurrence rate than delayed injection and resulted in no complications. |
| Careta 2013 ( | Shaving, cryosurgery, and intralesional steroid injection | \ | Shaving associated with cryosurgery seems to be a useful treatment for large keloid scars |
| Carvalhaes 2015 ( | Triamcinolone injections, surgical resection, and local pressure | \ | The combination of infiltration TCN month to 20 mg/mL (1.2 mg to 2.0 mg per mm3 TCN injury), surgical excision, and pressure application device is effective for the treatment of keloid ear lobe. |
| Chen 2017 ( | Intralesional injection of diprospan (2 mg betamethasone disodium phosphate and 5 mg betamethasone dipropionate in 1 mL) | Intralesional injection of diprospan with a combination of 0.5 mL 5-fluorouracil (25 mg/mL)/diprospan + 5-FU + 1,064-nm Nd: YAG laser | The combination of diprospan + 5-FU + Nd: YAG was the most efficacious therapy for keloid scars. |
| Chen 2020 ( | Continuous tension reduction | \ | The technique of continuous tension reduction could be used as an alternative method to prevent keloid recurrence under the condition of without radiotherapy |
| Chernoff 2007 ( | Dermatix gel | Silicone gel sheeting | Dermatix is a useful treatment for abnormal scarring. |
| Cho 2010 ( | 1,064-nm Q-switched Nd: YAG laser with low fluence | \ | QS Nd: YAG laser with low fluence may be used for the treatment of keloids and hypertrophic scars. |
| Choi 2020 ( | Triamcinolone acetonide intralesional injection | \ | TA ILI after intralesional excision can be effective for the management of auricular keloids. A low recurrence rate, similar to that of postoperative radiation therapy, was obtained with an effective surgical procedure and minimal postoperative treatment. |
| Chopinaud 2014 ( | Intralesional Cryosurgery | \ | Intralesional cryosurgery is an effective treatment for keloids |
| Cicco 2013 ( | High-dose-rate interstitial brachytherapy | Low-dose-rate interstitial brachytherapy | Postoperative brachytherapy is an effective treatment for keloids. |
| Clavere 1997 ( | Iridium 192 brachytherapy | \ | Iridium 192 brachytherapy is an effective treatment for keloids |
| Copcu 2004 ( | Combination of Surgery and Intralesional Verapamil Injection | \ | Surgical excision with W-plasty or skin grafting and intralesional verapamil injection may be a good alternative in the treatment of keloids. |
| Dai 2021 ( | Combination of ablative fractional carbon dioxide laser and platelet-rich plasma | Ablative fractional carbon dioxide laser | PRP is an effective adjunct for AFCL in the treatment of hypertrophic burn scars and that the combination of PRP and AFCL proved to be more useful than AFCL alone. |
| Darougheh 2007 ( | Intralesional triamcinolone acetonide | Combination of TAC and 5-fluorouracil | The overall efficacy of TAC + 5-FU was comparable with TAC, but the TAC + 5-FU combination was more acceptable to patients and produced better results. |
| Daurade 2020 ( | Combining surgical excision and high-dose-rate brachytherapy | \ | Extralesional excision combined with postoperative high-dose-rate brachytherapy seems to be one of the most effective invasive protocols to treat and prevent keloids |
| Davari 2012 ( | Pulsed dye laser | Nine weeks after suture removal | The pigmentation and erythema values following early treatment were higher than those following late treatment or no treatment, and the elasticity values were lowest following late treatment. |
| Davison 2009 ( | 5-FU + steroid with excision | 5-FU + steroid without excision/steroid treatment with excision | Combination 5-FU/triamcinolone is superior to intralesional steroid therapy in the treatment of keloids. |
| Deng 2021 ( | Intralesional triamcinolone (5 mL 1%) and 5-fluorouracil (0.6 mL 2.5%) injections and Strontium-90 brachytherapy | Intralesional triamcinolone (5 mL 1%) and 5-fluorouracil (0.6 mL 2.5%) injections | Strontium-90 brachytherapy as an adjuvant radiation could effectively reduce the recurrence of small keloids after intralesional triamcinolone and 5-fluorouracil injections. |
| Dina 2021 ( | Combined fractional ablative 2,940 nm Er: YAG laser and topical application of steroid cream | Intralesional corticosteroid injection | The use of ablative fractional laser-assisted delivery of topical steroid can offer a safer and better aesthetic treatment option |
| Disphanurat 2023 ( | Triamcinolone acetonide-loaded dissolving microneedle patch | Drug-free DMN patch | DMN patches were effective in the transdermal drug delivery of TAC for the treatment of HTSs |
| Dogahe 2023 ( | Intralesional triamcinolone (40 mg/mL) and verapamil (2.5 mg/mL) | Intralesional triamcinolone alone (40 mg/mL) | The combination of verapamil and triamcinolone provides a more effective treatment for keloids, thereby highlighting the potential of verapamil in scar reduction |
| Emad 2010 ( | Surgical excision and radiotherapy | Cryotherapy and intralesional steroid | Although cryotherapy combined with intralesional steroids was associated with more side effects and higher relapse rates, it could be a good choice for small and newly formed keloids. |
| Erlendsson 2022 ( | A pneumatic jet injection with 5-fluorouracil and triamcinolone acetonide | 5-FU + TAC | A single PJI injection containing 5-FU and TAC can significantly improve the height and pliability of HTS. |
| Erol 2008 ( | Intense Pulsed Light | \ | IPL is effective not only in improving the appearance of hypertrophic scars and keloids regardless of their origin, but also in reducing the height, redness, and hardness of scars. |
| Escarmant 1993 ( | Iridium 192 interstitial irradiation after surgical excision | \ | The effectiveness of the method linking surgical excision and Iridium 192 interstitial irradiation shows the importance of the sterile conditions of the treatment. |
| Espana 2001 ( | Bleomycin | \ | Bleomycin seems to be a useful treatment for keloid scars |
| Francesca 2010 ( | Self-drying silicone gel | Compared with the base cream, self-drying silicone gel has the advantage to dry quickly and allow the subsequent application of sunscreens and other cosmetics. | |
| Francisco 2013 ( | Combination of bleomycin and triamcinolone acetonide | \ | The best results were obtained in keloids over 1 cm2 or when divided into 1 cm2 square areas. |
| Friedman 2020 ( | Erbium glass, 1,540 nm laser | Not treated | a single presurgical laser treatment of the planned incision site is a simple, safe, and painless strategy to substantially improve the final scar appearance. |
| Gamil 2018 ( | Er: YAG laser | Long-pulsed Nd: YAG laser | The Er: YAG laser proved to be a potentially effective and safe modality both in the early and late AKN lesions. |
| Gamil 2019 ( | Combined intralesional triamcinolone acetonide with botulinum toxin type A | Intralesional triamcinolone acetonide/intralesional botulinum toxin type A | Combined injection of intralesional steroids with BTX-A appears to be superior to either therapy alone and offer the best benefit of safer and more efficacious response with lesser side effects. |
| George 2005 ( | Intralesional 5-fluorouracil | \ | Intralesional 5-FU may be effective in the treatment of keloids, but recurrence is common. |
| Guix 2001 ( | Interstitial high-dose-rate brachytherapy | \ | HDR brachytherapy is an effective treatment for keloid scars. It is well tolerated and does not present significant side effects. |
| Hafkamp 2017 ( | Interstitial high-dose-rate brachytherapy | \ | Plastic surgery followed by a single dose of 13 Gy HDR brachytherapy resulted in 76% local control of keloid with a relatively good cosmetic outcome. |
| Hatamipour 2009 ( | Combined topical silicone and 5Fluorouracil | Topical silicone | The modality of combined 5-FU and topical silicone is a sound approach for the prevention of keloids |
| Hewedy 2020 ( | Intralesional triamcinolone acetonide (20 mg/mL) and Platelet rich plasma | TA (20 mg/mL) alone | Combining intralesional PRP with TA could yield cosmetically better outcomes in keloid treatment with a lower incidence of TA-induced side effects, especially atrophy and hypopigmentation. |
| Hietanen 2018 ( | Intralesional triamcinolone | TAC and 5-FU injections did not differ in their clinical effectiveness in this randomized study | |
| Hoang 2016 ( | Interstitial high dose rate brachytherapy | Excision alone/external beam radiotherapy | Post-excision RT shows a significant reduction in keloid recurrence compared to excision alone. While the recurrence control rates are not statistically different between EBRT and brachytherapy, keloids treated with EBRT recurred significantly later than those treated by HDR brachytherapy |
| Hou 2023 ( | Punch excision combined with intralesional steroid injection | Intralesional Steroid Injection alone | The combination of punch excision and intralesional steroid injection has a notable therapeutic effect on keloids, shortening the treatment course without evident adverse reactions. |
| Hye 2015 ( | Copper bromide laser and intralesional triamcinolone injection (2.5 mg/mL or 5 mg/mL) | \ | Three to four treatment sessions were required to reduce scar VSS score by 50% when using the combination treatment of CBL and TA ILI. |
| Jiang 2015 ( | Interstitial high-dose-rate brachytherapy | \ | Brachytherapy may be advantageous in the management of high-risk keloids or as salvage treatment for failure after external beam therapy. |
| Jiang 2017 ( | Interstitial high-dose-rate brachytherapy | \ | Brachytherapy may be advantageous in the management of high-risk keloids, even after failure of external beam radiotherapy and other treatment procedures |
| Kant 2018 ( | Triamcinolone and verapamil | \ | Combined therapy of triamcinolone and verapamil results in overall significant scar improvement with a long-term stable result |
| Kaushal 2020 ( | Combined intralesional radiofrequency and intralesional triamcinolone acetonide | Intralesional triamcinolone acetonide alone | Thus, both the studied modalities of treatment produced equal efficacy and safety but with less recurrence in the combined group. |
| Khalid 2018 ( | intralesional 5-FU/TAC injections | Radiotherapy | Excision and intralesional5-FU/TAC is an effective treatment for keloids on the ears |
| Khan 2019 ( | Intralesional bleomycin | Intralesional triamcinolone | Intralesional bleomycin is more efficacious than intralesional triamcinolone acetonide in the treatment of keloids |
| Khattab 2019 ( | Intralesional verapamil alone 2.5 mg/mL. | Combination of PDL and intralesional verapamil alone 2.5 mg/mL | Combination therapy with PDL + intralesional verapamil was superior in efficacy when compared to intralesional verapamil alone, in the treatment of keloids |
| Khedr 2019 ( | Nd: YAG laser | Combined intense pulsed light and radiofrequency | Both modalities were successful in the treatment of hypertrophic scars; however, a significant improvement in the clinical and histopathological findings was detected with the E-light method. |
| Kim 2015 ( | Intense pulsed light device and intralesional corticosteroid injection | \ | IPL + corticosteroid injection can improve the appearance of keloids and hypertrophic scars |
| Kim 2022 ( | Pulsed dye laser therapy combined with intralesional triamcinolone injection | \ | Early intervention using PDL combined with TAILI could prevent the recurrence or progression of hypertrophic CS scarring after surgical scar removal. |
| Lee 2008 ( | Triamcinolone acetonide intralesional injection + Interferon- | Triamcinolone acetonide intralesional injection | Intralesional IFN-伪2b is an effective and safe treatment for keloids. |
| Lee 2015 ( | 6-MeV electron beam | \ | Radiotherapy should be initiated within 72 h of surgical excision. |
| Leeuwen 2014 ( | Intralesional Cryotherapy | \ | Intralesional cryotherapy for the treatment of keloid scars shows favorable results in terms of reduction of volume and complaints of pain and pruritus. However, no complete eradication was obtained in some cases, and recurring scars were observed. |
| Levenberg 2020 ( | Intralesional 5FU and corticosteroids | \ | Improved appearance of keloids and symptomatic relief were achieved by intralesional administration of combined 5-fluorouracil and corticosteroid through high-pressure jet injections. |
| Li 2020 ( | Intralesional 1,470 nm bare-fiber diode laser | \ | The intralesional 1,470 nm bare-fiber diode laser significantly improved hypertrophic and keloid scars based on both subjective and objective analyses and supports this type of laser therapy as a safe and effective minimally invasive treatment option. |
| Li 2022 ( | Excision followed by 5-FU and betamethasone intralesional injections | 5-FU and betamethasone intralesional injections/excision followed by radiotherapy | Excision followed by intralesional low concentrations of 5-FU (12.5 mg/mL) with betamethasone is a safe and sustainable treatment for keloids, with no significant difference from excision followed by radiotherapy. |
| Liu 2023 ( | Combined pulsed dye laser and triamcinolone acetonide | Triamcinolone acetonide | Compared with TAC injection alone, PDL dynamically combined with TAC in the treatment of keloid with post-operative recurrence can shorten the relative cure time, reduce the number of TAC injections, and improve the clinical efficacy. |
| Luo 2023 ( | The combined application of bleomycin and triamcinolone | \ | The combined application of bleomycin and triamcinolone acetonide can effectively cure keloids and hypertrophic scars. |
| Lv 2021 ( | Ablative fractional CO2 laser surgery | Conventional surgery | CO2-AFL surgery significantly improved sleep quality and reduced pain and pruritus in patients with hypertrophic scars. |
| Maemoto 2020 ( | electron beam radiation therapy | \ | Multiple lesions and irregular shape were risk factors of keloid recurrence after postoperative electron beam radiotherapy. |
| Manjunath 2021 ( | Surgical excision and adjuvant high-dose rate brachytherapy | \ | Surgical excision with postoperative radiotherapy is best for preventing recurrence. |
| Manuskiatti 2021a ( | Laser + steroid | Laser + petrolatum | Fractional laser monotherapy is an effective treatment for hypertrophic scars, and the application of a topical corticosteroid provides no long-term synergistic effect to fractional laser monotherapy. |
| Manuskiatti 2021b ( | Thermomechanical fractional injury-assisted topical corticosteroid (40 mg/mL) | Corticosteroid injection (40 mg/mL) | TMFI-assisted topical corticosteroid delivery is an effective treatment for HTS with a lower risk of adverse effects compared with corticosteroid injection |
| Martin-Garcia 2005 ( | Imiquimod 5% Cream | \ | Imiquimod 5% cream may prove to be a therapeutic alternative for the prevention of recurrences in excised earlobe keloids. |
| Meseci 2019 ( | Topical corticosteroid ointment | Untreated | The clinical outcomes in both groups were similar. |
| Meymandi 2014 ( | Intense pulsed light method along with corticosteroid injection | \ | Intralesional corticosteroid injection + IPL increases the recovery level of hypertrophic and keloid scars. |
| Meymandi 2016 ( | Intense pulsed light | Cryotherapy | Both methods were highly successful in curing scars |
| Monteiro 2022 ( | Intralesional 5-Fluorouracil (50 mg/mL) | Combination of 5 fluorouracil (50 mg/mL) with triamcinolone acetonide (40 mg/mL) | 5-FU, both as a single agent or in combination with steroids, is equally efficacious in reducing the keloid size. The side effects are fewer with the combination group |
| Moravej 2022 ( | Intralesional bleomycin (1.5 mg/mL) | Intralesional triamcinolone (20 mg/mL) | Intralesional bleomycin is effective as triamcinolone in the treatment of keloids and hypertrophic scars; however, bleomycin should be used carefully, due to adverse events such as pain, ulceration, and hyperpigmentation. |
| Muneuchi 2009 ( | Intralesional injection of triamcinolone acetonide | \ | Intralesional injection of triamcinolone acetonide proved to be a potentially effective and safe modality in keloids. |
| Neinaa 2021 ( | Intralesional injection of botulinum toxin type-A (5 IU/injection point) | Intralesional injection of platelet rich plasma (0.1 mL/injection point)/intralesional injection of triamcinolone acetonide (20 mg/session) | Both BTX-A and PRP could yield a chance for cosmetically better outcomes in keloid treatment than conventional TAC injection. |
| Nishi 2022 ( | Combination of cryotherapy with intralesional corticosteroid | A combination of fractional CO2 laser followed by topical corticosteroids | Both regimens showed excellent responses with minimum recurrence rates |
| Nor 2016 ( | Either daily topical clobetasol propionate 0.05% cream under occlusion with a silicone dressing | Monthly intralesional triamcinolone injection | Clobetasol propionate 0.05% cream under occlusion with silicone dressing is equally effective and has fewer adverse effects compared to IL triamcinolone. |
| Noruri 2003 ( | 585-nm pulsed dye laser | Not treated | The 585-nm PDL is effective and safe in improving the quality and cosmetic appearance of surgical scars in skin types I–IV starting on the day of suture removal. |
| Ogawa 2002 ( | Electron beam radiation therapy | \ | A keloid with a high risk of recurrence should be treated with electron beam radiation doses and posttreatment self-management |
| Ogawa 2014 ( | Surgical excision and radiotherapy | \ | We recommend surgical removal together with postsurgical radiation therapy consisting of 15-Gy irradiation administered in three fractions over 3 days. |
| Ollstein 1981 ( | Combined surgical excision and immediate X-ray therapy | \ | Intralesional excision combined with immediate X-ray therapy is effective in treating keloids |
| Intralesional steroid injections (20 mg/mL) | \ | Surgical excision followed by intra- and postoperative intralesional steroid injection therapy has provided reasonable success at preventing recurrence | |
| Payapvipapong 2014 ( | Intralesional triamcinolone acetonide (10 mg/mL) | Intralesional bleomycin (1 mg/mL) | No skin atrophy was detected in this study. Intralesional bleomycin is a safe and effective treatment for keloids and hypertrophic scars. |
| Qiao 2017 ( | Surgery combined with lucortriticod and electron irradiation group | In the treatment of ear scar, the efficacy of Surgery combined with lucortriticod and electron irradiation group > Surgery combined with local injection of glucocorticoid group = Surgery combined with superficial X-ray group > Surgery group | |
| Ragoowansi 2002 ( | Surgical excision and immediate single-fraction radiotherapy | \ | Extralesional excision of keloid followed by early, single-fraction, postoperative radiotherapy is both simple and effective in preventing recurrence at excision sites. |
| Ramadan 2021 ( | Pulsed Nd: YAG laser and intralesional bleomycin | Pulsed Nd: YAG laser only | Long-pulsed Nd-YAG laser combined with intralesional bleomycin could be a promising way for the treatment of keloids or hypertrophic scars. |
| Rasaii 2018 ( | Intralesional triamcinolone (40 mg/mL) in combination with botulinum toxin A (20 mg/mL) | Intralesional triamcinolone (40 mg/mL) alone | Intralesional injection of triamcinolone and BTA has been found to have a similar effect on keloidal cosmesis to triamcinolone alone. |
| Reinholz 2020 ( | Intralesional 5-fluorouracil (50 mg/mL) in combination with triamcinolone acetonide (40 mg/mL) | \ | The results of this study confirm the efficacy and safety of the use of a combination of 5-FU and TAC in a 3:1 ratio in keloids based on objective measurements. Treatments were well tolerated and demonstrated stable results at 12-month FU. |
| Sabry 2019 ( | CO2 laser and topically applied 5-FU | CO2 laser and topically applied verapamil hydrochloride/ablative fractional CO2 laser monotherapy | Combined fractional CO2 laser and topical 5-FU or verapamil hydrochloride offer a safe therapy for HTSs and keloids |
| Sabry 2020 ( | Combined laser and intralesional injection of botulinum toxin A | Intralesional injection of botulinum toxin A | Laser-assisted delivery of Botox is a novel modality of treatment with minimal side effects and promising efficacy. |
| Sadeghinia 2012 ( | Intralesional triamcinolone acetonide | 5-FU tattooing | 5-FU tattooing was more effective than intralesional TAC for treating keloids. |
| Saha 2012 ( | 5-FU (50 mg/mL) | Triamcinolone acetonide (40 mg/mL) | Triaclcinolone is a better-tolerated and less toxic alternative to 5-FU in the management of keloids |
| Saki 2019 ( | Intralesional triamcinolone acetonide | Intralesional Verapamil | Verapamil is not as effective as triamcinolone in the treatment of keloids. |
| Saray 2005 ( | Dermojet injections of bleomycin (1.5 IU/mL) | \ | Intralesional jet injection of bleomycin is an effective and safe method of treating keloids and hypertrophic scars that are unresponsive to intralesional steroid therapy. |
| Seo 2011 ( | Topical and intralesional mitomycin C (1 mg/mL) | \ | Topical application of mitomycin C was safe and effective for the treatment of keloids and HTS |
| Shaarawy 2014 ( | Intralesional botulinum toxin type A | Intralesional steroid | The current work establishes the possible effective and safe “off-label” use of BTA in such an indication. |
| Sharma 2007 ( | Combination of liquid nitrogen and intralesional triamcinolone acetonide (5 mg/mL) | Liquid nitrogen alone | the combination therapy is a better modality of treatment of small keloids compared with liquid nitrogen cryosurgery alone |
| Sharma 2021 ( | Intralesional 5-FU and triamcinolone acetonide | Combination of intralesional bleomycin and triamcinolone acetonide | A greater improvement in the signs and symptoms of keloids (with respect to cosmetic problems, restriction of movement, and tenderness) was observed in the patients treated with a combination of intralesional bleomycin and triamcinolone acetonide compared to those treated with a combination of intralesional 5-FU and triamcinolone acetonide |
| Shen 2015 ( | Hypofractionated electron-beam radiation | \ | Early postoperative radiotherapy with limited hypofractionation could be a good choice for keloid treatment |
| Shin 2019 ( | Combination of non-ablative fractional laser and intralesional triamcinolone injection | Intralesional triamcinolone injection | Combination therapy with non-ablative fractional laser and intralesional steroid injection showed better results for the treatment of hypertrophic scars and keloids with fewer treatment sessions, better patient satisfaction, and longer remission periods. |
| Son 2014 ( | 578 nm copper bromide laser combined with intralesional corticosteroid injection | \ | The adjunctive use of 578 nm copper bromide laser decreased the telangiectatic side effects of an intralesional corticosteroid injection by reducing the vascular components of scars. |
| Son 2020 ( | A single dose of low-energy superficial X-ray radiation | \ | A single 8Gy dose of superficial 50 kV radiation delivered an average of 34 days following keloid excision maybe sufficient to minimize recurrence. |
| Song 2014 ( | Single-fraction radiotherapy | \ | Surgical excision of the keloid, followed by immediate, single-fraction, high-dose radiotherapy, is both safe and effective in preventing recurrence of therapy-resistant keloids |
| Song 2018 ( | Hyperbaric oxygen therapy | Surgical excision and radiotherapy | Adjunctive HBOT effectively reduces the keloid recurrence rate after surgical excision and radiotherapy by improving the oxygen level of the tissue and alleviating the inflammatory process |
| Song 2018 ( | Intralesional triamcinolone acetonide injection | \ | The treatment efficacy was better when applied during the static stage of pathological scarring rather than the early stage |
| Srivastava 2018 ( | Intralesional triamcinolone acetonide (40 mg/mL) and 5-fluorouracil (50 mg/mL) | Intralesional triamcinolone acetonide (40 mg/mL)/intralesional 5-fluorouracil (50 mg/mL) | TAC, 5FU, and their combination are all effective in keloid scars. A combination of TAC + 5FU seems to offer the balanced benefit of faster and more efficacious response with lesser adverse effects when compared to individual drugs |
| Sruthi 2017 ( | Single-fraction radiation | \ | Radiation as an adjuvant therapy in the postoperative period within 48 h is a cosmetically acceptable, safe, painless, cost-effective treatment with good patient compliance to prevent keloid recurrence. |
| Stephanides 2011 ( | Intralesional triamcinolone (10 mg or 40 mg/dl) and pulsed dye laser | \ | Pulsed-dye laser with or without intralesional triamcinolone is a moderately effective treatment of keloid scars with a very good side-effect profile and high patient satisfaction. |
| Stern 1989 ( | Carbon dioxide laser excision | \ | The carbon dioxide laser excision can not effectively cure Earlobe Keloids. |
| Stewart 2006 ( | The combination of surgical excision with the application of topical mitomycin-C | \ | The topical application of mitomycin-C is an effective therapy for preventing keloid recurrence in the head and neck. |
| Stromps 2013 ( | Intralesional cryotherapy combined with postoperative silicone gel sheeting | Intralesional cryotherapy alone | The use of combined intralesional cryosurgery followed by the application of silicone gel sheeting to treat refractory keloids. |
| Sunil 2018 ( | Fractional CO2 laser | Intralesional triamcinolone (40 mg/mL)/intralesional verapamil (2.5 mg/ mL) | fractional CO2 laser and verapamil are as efficient as triamcinolone acetonide (TAC) for treating keloids, except it takes longer for the laser and verapamil to act compared to TAC. |
| Suwanchinda 2022 ( | Cold atmospheric-pressure plasma | untreated | CAP technology could be considered an alternative treatment for keloids, offering mild-to-moderate improvement with minimal side effects. |
| Tawaranurak 2022 ( | Treated with fractional CO2 laser + topical TA | Intralesional TA | The combination of a fractional CO2 laser with topical TA was an alternative option for the treatment of keloids without any adverse effects. |
| Tawfic 2020 ( | Combined: Fractional and Nd YAG | Nd: YAG alone/Fractional laser alone | Long-pulsed Nd: YAG laser is an effective and safe treatment for hypertrophic scars and keloids. Fractional CO2 laser yields better improvement in hypertrophic scars, while in keloids, both fractional CO2 and Nd: YAG lasers achieve comparable improvement. Combination in the same session did not add significant additional benefit, and the side-effect profile was higher. |
| Tawfik 2019 ( | Combined 5-fluorouracil and fractional erbium YAG laser | Topical 5-fluorouracil cream | Treatment of severe HTS with combined 5-FU and ablative fractional erbium YAG laser is more effective than 5-FU alone. |
| Tsai 2019 ( | Combination of 1,064-nm neodymium-doped yttrium aluminum garnet laser and steroid tape | Steroid Tape | Nd: YAG laser treatment effectively decreased the total treatment time of hypertrophic cesarean-section scars. |
| Viani 2009 ( | Strontium 90 brachytherapy | \ | Excision plus Sr-90 brachytherapy is effective in the eradication of keloids. |
| Wang 2020 ( | Combined ultrapulse fractional carbon dioxide laser and topical triamcinolone | \ | Combination keloid therapy using UFCL and tropical triamcinolone has overall significant improvement and low recurrence rate with a long-term stable results. |
| Wang 2020 ( | Combined surgical excision and electron external beam radiation | \ | Surgical excision followed by immediate adjuvant radiation therapy for keloids provides excellent local control of disease as well as cosmetic appearance. |
| Wen 2021 ( | Hypofractionated radiotherapy | \ | A postoperative hypofractionation with radiation dose of 20Gy in 5 fractions may be effective, easy to accept and safe for keloid patients. |
| Weshahy 2012 ( | Combined intralesional cryosurgery and intralesional steroid injection | \ | Combined Intralesional cryosurgery and intralesional steroid injection seems to be a useful treatment for keloids scars |
| Weshay 2015 ( | Combination of Radiofrequency and intralesional steroids (10 mg/mL) | \ | Radiofrequency tissue volume reduction combined with IL steroid is an effective treatment modality for keloids. It is an easy procedure with acceptable cosmetic outcome and less rate of recurrence. |
| Wittenberg 1999 ( | 585-nm flashlamppumped pulsed-dye laser | Silicone gel sheeting | The improvements in scar sections treated with silicone gel sheeting and pulsed-dye laser were no different from those in control sections. |
| Yii 1996 ( | Cynthaskin and topical steroid | \ | All patients achieved symptomatic relief of itch and pain |
| Yosipovitch 2009 ( | Cryotherapy and steroid injection | Cryotherapy alone/Steroid injection | Combined injection of intralesional steroids with cryotherapy appears to be superior to other current modalities. |
| Zawahry 2015 ( | Fractional CO2 laser | Untreated | Fractional CO2 laser is a safe and effective modality for the treatment of hypertrophic burn scars, with improvement achieved |
| Zouboulis 2020 ( | Combined liquid nitrogen contact cryosurgery with intralesional corticosteroids | Liquid nitrogen contact cryosurgery | Cryosurgery without and with intralesional corticosteroids is effective and safe on young, |
| Zhou 2023 ( | Ablative fractional carbon dioxide laser +1 g triamcinolone external application | Ablative fractional carbon dioxide laser + 40 mg/mL triamcinolone Intralesional injection | Using the ablative fractional carbon dioxide laser followed by different topical triamcinolone delivery methods is effective and safe for thicker hypertrophic scar improvement. |
| Zhang 2023 ( | Intervention of the experimental group | Intervention of the controlled group | The combination of CO2 fractional laser and narrowband IPL efficiently improved the appearance and profile of hypertrophic scars, offering a comprehensive and reliable approach for scar therapy. |
| Li 2024 ( | Combined Intense Pulsed Light (IPL) with Fractional CO2-Laser | Fractional CO2-Laser | Keloid-cross-flap surgery could provide favorable morphologic repair of the auricular keloid, and postoperative superficial radiotherapy shows higher compliance and lower recurrence rate compared to compression treatment. |
| Pazyar 2024 ( | Intralesional cryosurgery | Contact cryosurgery | It seems that the injection of vitamin D at the site of the lesion helps to treat it, but the effectiveness of the usual triamcinolone treatment was still higher |
| Khan 2025 ( | Intralesional verapamil (2.5 mg/mL) | Intralesional corticosteroids (40 mg/mL) | Surgical excision and radiotherapy can not effectively cure Keloids. |
| Jiang 2024 ( | Intralesional triamcinolone (40 mg/mL) | \ | Fractional CO2 laser followed by 5-ALA PDT is a promising method for treating keloids. |
| Hu 2023 ( | A triple therapy comprising the use of steroid injections and cream (triamcinolone acetonide), surgery, and silicone gel strip/sheet pressure application | \ | Surgical resection, super-subtraction sutures, and superficial radiotherapy are treatment methods with short courses, low recurrence rates, and good safety profiles. |
| Yang 2025 ( | Iridium-192 high-dose rate surface mold brachytherapy | \ | The sequentially comprehensive treatment based on surgery has a significant curative effect, as well as a low recurrence rate |
| Park 2024 ( | Intralesional verapamil hydrochloride (concentration 2.5 mg/mL) | Intralesional triamcinolone acetonide (concentration 40 mg/mL) | Dual therapy involving TAC injection and Nd: YAG laser treatment was more effective than TAC injection alone for managing keloid scars after surgery. |
| Harsono 2023 ( | Intralesional triamcinolone (concentration 40 mg/mL) | intralesional 5-fluorouracil (concentration 250 mg/5 mL)/intralesional verapamil (concentration 2.5 mg/mL)/intralesional platelet-rich plasma (2.4 mL) | Intralesional injection of umbilical cord Mesenchymal stem cells is effective in the eradication of keloids. |
| Qiu 2025 ( | Fractional CO2 laser with intralesional steroid | Intralesional steroid alone | The findings indicate that laser-assisted drug delivery using MFT with a CO2 laser demonstrates significant clinical efficacy, a low recurrence rate, and an absence of serious adverse reactions in treating hypertrophic scars. |
| Aristides 2024 ( | Fractional carbon dioxide laser with intralesional 5-fluorouracil (50 mg/mL) | \ | A combination of two ablative laser delivery modes within a single laser platform provided for effective and safe keloid management and left patients highly satisfied. |
| Lim 2024 ( | Combination of surgical excision and perioperative corticosteroid injection (40 mg/mL) | \ | This demonstrates the use of transdermal gene-silencing technology in scar inhibition and that siRNA microneedle patches can be effective and safe in reducing scar tissue formation |
| Study | Intervention of the experimental group | Intervention of the controlled group | Outcomes | Indicators of outcome (experimental group) | Indicators of outcome (controlled group) |
|---|---|---|---|---|---|
| Choi 2020 ( | Triamcinolone acetonide intralesional injection | \ | Recurrence rate | 0.05 | \ |
| Darougheh 2007 ( | Intralesional triamcinolone acetonide | Combination of TA and 5-fluorouracil | Efficacy | 0.2 | 0.55 |
| Muneuchi 2009 ( | Intralesional injection of triamcinolone acetonide | \ | Efficacy | 0.55 | \ |
| Saki 2019 ( | Intralesional Triamcinolone Acetonide | Intralesional Verapamil | VSS | 3.1 ± 1.85 | 0.21 ± 0.56 |
| Acosta 2016 ( | Intralesional Triamcinolone (40 mg/mL) | \ | Size reduction | 82.7% | \ |
| Hietanen 2018 ( | Intralesional triamcinolone | Efficacy | 60% | 46% | |
| Song 2018 ( | Intralesional triamcinolone acetonide injection | \ | Efficacy | 78.2% | \ |
| Albalat 2021 ( | Intralesional triamcinolone (concentration 40 mg/mL) | Intralesional 5-fluorouracil (concentration 250 mg/5 mL)/intralesional verapamil (concentration 2.5 mg/mL)/intralesional platelet-rich plasma (2.4 mL) | Efficacy | 0.75 | 55%/80%/72% |
| Payapvipapong 2014 ( | Intralesional triamcinolone acetonide (10 mg/mL) | Intralesional bleomycin (1 mg/mL) | POSAS improvement rate | 0.2754 | 0.3812 |
| Disphanurat 2023 ( | Triamcinolone acetonide-loaded dissolving microneedle patch | Drug-free DMN patch | Mean change of POSAS | −7.2(−12.94, −1.46) | --5.2(−12.17, 1.77) |
| SADEGHINIA 2012 ( | Intralesional triamcinolone acetonide | 5-FU tattooing | Efficacy | \ | \ |
| Study | Intervention of the experimental group | Intervention of the controlled group | Outcomes | Indicators of outcome (experimental group) | Indicators of outcome (controlled group) |
|---|---|---|---|---|---|
| manuskiatti 2021 ( | Fractional Laser + steroid | Laser + petrolatum | Reduction in hypertrophic scars thickness | 0.66 ± 0.39 | 0.69 ± 0.36 |
| Son 2014 ( | 578 nm copper bromide laser combined with intralesional corticosteroid injection | \ | PGA | 2.08 | \ |
| Levenberg 2020 ( | Intralesional 5FU and corticosteroids | \ | VSS improvement rate | 0.53 | \ |
| Yii 1996 ( | Cynthaskin and topical steroid | \ | Efficacy | 0.7562 | \ |
| Francisco 2013 ( | Combination of bleomycin and triamcinolone acetonide | \ | Efficacy | 0.9729 | \ |
| Weshahy 2012 ( | Combined intralesional cryosurgery and intralesional steroid injection | \ | Reduction area of Keloids | 0.935 | \ |
| Meymandi 2014 ( | Intense pulsed light method along with corticosteroid injection | \ | Efficacy | 89.1% | \ |
| Stephanides 2011 ( | Intralesional triamcinolone (10 mg or 40 mg/dL) and pulsed dye laser | \ | Efficacy | 76% | \ |
| Kim 2015 ( | Intense pulsed light device and intralesional corticosteroid injection | \ | Improvement in MVSS | 0.981 | \ |
| Kim 2022 ( | Pulsed dye laser therapy combined with intralesional triamcinolone injection | \ | VSS | 3.11 ± 1.52 | \ |
| Hye 2015 ( | Copper bromide laser and intralesional triamcinolone injection (2.5 mg/mL or 5 mg/mL) | \ | VSS | \ | \ |
| Aljodah 2021 ( | Combination of surgical excision and perioperative corticosteroid injection (40 mg/mL) | \ | Recurrence rate | 9.6% | \ |
| Park 2012 ( | Intralesional steroid injections (20 mg/mL) | \ | Recurrence rate | 23.5% | \ |
| Reinholz 2020 ( | Intralesional 5-fluorouracil (50 mg/mL) in combination with triamcinolone acetonide (40 mg/mL) | \ | Improvement in POSAS | 39% | \ |
| Hewedy 2020 ( | Intralesional triamcinolone acetonide (20 mg/mL) and platelet rich plasma | TA (20 mg/mL) alone | Patients’ satisfaction | 65% | 55% |
| Weshay 2015 ( | Combination of radiofrequency and intralesional steroids (10 mg/mL) | \ | Volume reduction/Recurrence rate | 95.42 ± 7.62/10% | \ |
| Tawaranurak 2022 ( | Treated with fractional CO2 laser + topical triamcinolone | Intralesional TA | Efficacy/Recurrence rate | 63.6%/9.1% | 72.7%/18.2% |
| Luo 2023 ( | The combined application of bleomycin and triamcinolone | \ | Recurrence rate | 6.9–7.9% | \ |
| Khalid 2018 ( | Intralesional 5-FU/TA injections | Radiotherapy | Efficacy | 0.7333 | 0.4333 |
| Manuskiatti 2021 ( | Thermomechanical fractional injury-assisted topical corticosteroid (40 mg/mL) | Corticosteroid injection (40 mg/mL) | VSS | 2.28 ± 1.7 | 2.52 ± 1.83 |
| Erlendsson 2022 ( | A pneumatic jet injection with 5-fluorouracil and triamcinolone acetonide | 5-FU + TA | Improvement in VSS | 55% | 25% |
| Nishi 2022 ( | Combination of cryotherapy with intralesional corticosteroid | A combination of fractional CO2 laser followed by topical corticosteroids | MSS | 15.67 | 12.56 |
| Sharma 2021 ( | Intralesional 5-FU and triamcinolone acetonide | Combination of intralesional bleomycin and triamcinolone acetonide | Efficacy | 93.33% | 93.33% |
| Yosipovitch 2009 ( | Cryotherapy and steroid injection | Cryotherapy alone/Steroid injection | Thickness, pain, and itch | 7.7 ± 4.2 mm | 3.1 ± 2.2 mm/−0.25 ± 1.2 mm |
| Rasaii 2018 ( | Intralesional triamcinolone (40 mg/mL) in combination with botulinium toxin A (20 mg/mL) | Intralesional triamcinolone (40 mg/mL) alone | VSS | 6.43 ± 0.37 | 5.52 ± 0.32 |
| Srivastava 2018 ( | Intralesional triamcinolone acetonide (40 mg/mL) and 5-fluorouracil (50 mg/mL) | Intralesional triamcinolone acetonide (40 mg/mL)/intralesional 5-fluorouracil (50 mg/mL) | VSS | 0.3 ± 0.47 | 0.61 ± 0.45/0.2 ± 0.41 |
| Zouboulis 2020 ( | Combined liquid nitrogen contact cryosurgery with intralesional corticosteroids | Liquid nitrogen contact cryosurgery | Efficacy | 90% | 83.3% |
| Alexander 2018 ( | Fractional CO2 laser with intralesional steroid | Intralesional steroid alone | Efficacy | \ | \ |
| Gamil 2019 ( | Combined intralesional triamcinolone acetonide with botulinum toxin type A | Intralesional triamcinolone acetonide/intralesional botulinum toxin type A | Photographic documentation, the SBSES score, and CDU results | 0.673 ± 0.466 | 1.18 ± 1.44/1.63 ± 2.19 |
| Dogahe 2023 ( | Intralesional triamcinolone (40 mg/mL) and verapamil (2.5 mg/mL) | Intralesional triamcinolone alone (40 mg/mL) | VSS | 1.5 ± 0.6 | 4.1 ± 1.9 |
| Shin 2019 ( | Combination of non-ablative fractional laser and intralesional triamcinolone injection | Intralesional triamcinolone injection | Recurrence rate | 35.3% | 38.1% |
| Sharma 2007 ( | Combination of liquid nitrogen and intralesional triamcinolone acetonide (5 mg/mL) | Liquid nitrogen alone | Efficacy | 100% | 86.7% |
| Tsai 2019 ( | Combination of 1,064-nm neodymium-doped yttrium aluminum garnet laser and steroid tape | Steroid Tape | Time of total JSS score <3 | 16.9 months | 24.3 months |
| Hou 2023 ( | Punch excision combined with intralesional steroid injection | Intralesional steroid injection alone | VSS and POSAS | \ | \ |
| Liu 2023 ( | Combined pulsed dye laser and triamcinolone acetonide | Triamcinolone Acetonide | VSS | 4 | 5 |
| Lee 2008 ( | Triamcinolone acetonide intralesional injection + Interferon-α | Triamcinolone acetonide intralesional injection | Efficacy | 81.6% | 66% |
| Zhou 2023 ( | Ablative fractional carbon dioxide laser +1 g triamcinolone external application | Ablative fractional CO2 laser + 40 mg/ml triamcinolone intralesional injection | VSS | 5.94 ± 24.07 | 19.77 ± 21.25 |
| Park 2024 ( | Intralesional triamcinolone + ND: YAG laser | Intralesional triamcinolone | MVSS, POSAS, recurrence rate, and overall patient satisfaction | MVSS: 3.5 ± 0.3; POSAS: 1.9 ± 0.3; Recurrence rate: 4.35%; Overall patient satisfaction:4.5 ± 0.5 | MVSS: 3.7 ± 0.5; POSAS: 2.7 ± 0.4; Recurrence rate: 12.5%; Overall patient satisfaction:4.4 ± 0.6 |
| Study | Intervention of the experimental group | Intervention of the controlled group | Outcomes | Indicators of outcome (experimental group) | Indicators of outcome (controlled group) |
|---|---|---|---|---|---|
| Al-Mohamady 2016 ( | 595-nm Pulsed dye laser | Nd: YAG laser | VSS improvement rate | 0.5514 | 0.6544 |
| Li 2020 ( | Intralesional 1,470 nm bare-fiber diode laser | \ | VSS improvement rate | 0.42 | \ |
| Cho 2010 ( | 1,064-nm Q-switched Nd: YAG laser with low fluence | \ | The modified Vancouver General Hospital Burn Scar Assessment score | 5.9 | \ |
| Behera 2016 ( | CO2 Laser | Cryotherapy | Efficacy | 0.5278 | 0.6296 |
| Erol 2008 ( | Intense pulsed light | \ | Efficacy | 0.925 | \ |
| Davari 2012 ( | Pulsed dye laser | Nine weeks after suture removal | Elasticity values | 0.357 | 0.246 |
| Friedman 2020 ( | Erbium glass, 1,540 nm laser | Not treated | POSAS | 1.55–3 | 2.28–4.42 |
| Noruri 2003 ( | 585-nm pulsed dye laser | Not treated | Improvement in the VSS | 0.54 | 0.1 |
| Khedr 2019 ( | Nd: YAG laser | Combined intense pulsed light and radiofrequency | VSS | 3.75 ± 1.09 | 2.08 ± 0.86 |
| Stern 1989 ( | CO2 laser excision | \ | Recurrence rate | 73.91% | \ |
| ANG 2013 ( | CO2 laser ablation | Cold steel debulking surgery | Recurrence rate | 100 | 100 |
| Lv 2021 ( | Ablative fractional CO2 laser surgery | Conventional surgery | VAS | 3.57 ± 1.36 | 5.82 ± 1.86 |
| Meymandi 2016 ( | Intense pulsed light | Cryotherapy | Efficacy | 89.3% | 91.5% |
| Wittenberg 1999 ( | 585-nm flashlamp-pumped pulsed-dye laser | Silicone gel sheeting | blood flow, volume, and pruritus | \ | \ |
| Sunil 2018 ( | Fractional CO2 laser | Intralesional triamcinolone (40 mg/mL)/intralesional verapamil (2.5 mg/ mL) | VSS | 0.25 ± 44 | 0 ± 0/0.05 ± 0.22 |
| Gamil 2018 ( | Er: YAG laser | Long-pulsed Nd: YAG laser | efficacy | 91.8% | 88% |
| Zawahry 2015 ( | Fractional CO2 laser | Untreated | POSAS | 20.27 ± 14.7 | 15.42 ± 8.7 |
| Study | Intervention of the experimental group | Intervention of the controlled group | Outcomes | Indicators of outcome (experimental group) | Indicators of outcome (controlled group) |
|---|---|---|---|---|---|
| Daoud 2019 ( | Combined Intense Pulsed Light (IPL) With Fractional CO2-Laser | Fractional CO2-Laser | Average decrease in MSS score | Color: 2.21; Matte vs. shiny: 0.67; Contour: 1.87; Distortion: 1.83; Texture: 1.97 | Color: 1.2; Matte vs. shiny: 0.87; Contour: 1.5; Distortion: 1.6; Texture: 1.3 |
| Manuskiatti 2021 ( | Laser + steroid | Laser + petrolatum | Reduction in hypertrophic scars thickness | 0.66 ± 0.39 | 0.69 ± 0.36 |
| Son 2014 ( | 578 nm Copper Bromide Laser Combined with Intralesional Corticosteroid Injection | \ | PGA | 2.08 | \ |
| Tawfic 2020 ( | Combined: Fractional and Nd YAG | Nd: YAG alone/Fractional laser alone | VSS and POSAS | VSS: 45.63 ± 21.34; PSASA: 44.92 ± 10.13 | VSS: 47.34 ± 19.96; PSASA: 46.5 ± 9.22/VSS: 47.34 ± 19.96; PSASA: 46.5 ± 9.22 |
| Wang 2020 ( | Combined ultrapulse fractional carbon dioxide laser and topical triamcinolone | \ | Patient and observer scores | Observer: 19.17 ± 9.09; patient: 15.15 ± 7.51 | \ |
| Sabry 2020 ( | Combined laser and intralesional injection of botulinum toxin A | Intralesional injection of botulinum toxin A | VSS | 0.6 ± 0.2 | 0.7 ± 0.2 |
| Alhamzawi 2021 ( | Fractional carbon dioxide laser with intralesional 5-Fluorouracil (50 mg/mL) | \ | VSS improvement rate | 0.65 | \ |
| Annabathula 2017 ( | Fractional carbon dioxide, long pulse Nd: YAG and pulsed dye laser | \ | Efficacy | 0.7273 | \ |
| Meymandi 2014 ( | Intense pulsed light method along with corticosteroid injection | \ | Efficacy | 89.1% | \ |
| Stephanides 2011 ( | Intralesional triamcinolone (10 mg or 40 mg/dL) and pulsed dye laser | \ | Efficacy | 76% | \ |
| Kim 2015 ( | Intense pulsed light device and intralesional corticosteroid injection | \ | Improvement in MVSS | 0.981 | \ |
| Kim 2022 ( | Pulsed dye laser therapy combined with intralesional triamcinolone injection | \ | VSS | 3.11 ± 1.52 | \ |
| Hye 2015 ( | Copper bromide laser and intralesional triamcinolone injection (2.5 mg/mL or 5 mg/mL) | \ | VSS | \ | \ |
| Tawaranurak 2022 ( | Treated with fractional CO2 laser + topical triamcinolone | Intralesional TA | Efficacy/Recurrence rate | 63.6%/9.1% | 72.7%/18.2% |
| Ramadan 2021 ( | pulsed Nd: YAG laser and intralesional bleomycin | Pulsed Nd: YAG laser only | Efficacy | 1 | 0.8 |
| Dai 2021 ( | Combination of ablative fractional carbon dioxide laser and platelet-rich plasma | Ablative fractional carbon dioxide laser | VSS | 6.06 ± 1.44 | 8.16 ± 1.93 |
| Dina 2021 ( | Combined fractional ablative 2,940 nm Er: YAG laser and topical application of steroid cream | Intralesional corticosteroid injection | VSS | 2.07 ± 2.02 | 2.63 ± 2.09 |
| Alexander 2018 ( | Fractional CO2 laser with intralesional steroid | Intralesional steroid alone | Efficacy | \ | \ |
| Sabry 2019 ( | CO2 laser and topically applied 5-FU | CO2 laser and topically applied verapamil hydrochloride/ablative fractional CO2 laser monotherapy | VSS | 5.33 ± 1.6 | 4.3 ± 1.5/1.89 ± 1.05 |
| Shin 2019 ( | Combination of non-ablative fractional laser and intralesional triamcinolone injection | Intralesional triamcinolone injection | Recurrence rate | 35.3% | 38.1% |
| Tsai 2019 ( | Combination of 1,064-nm neodymium-doped yttrium aluminum garnet laser and steroid tape | Steroid Tape | Time of total JSS score <3 | 16.9 months | 24.3 months |
| Tawfik 2019 ( | Combined 5- fluorouracil and fractional erbium YAG laser | Topical 5-fluorouracil cream | VSS | 2.17 ± 1.11 | 4 ± 1.76 |
| Liu 2023 ( | Combined pulsed dye laser and triamcinolone acetonide | Triamcinolone acetonide | VSS | 4 | 5 |
| Zhang 2023 ( | Fractional carbon dioxide laser + 5-aminolevulinic acid photodynamic therapy | \ | POSAS | 38.58 ± 4.71 | 44.04 ± 5.07 |
| Jiang 2024 ( | Intralesional triamcinolone + ND: YAG laser | Intralesional triamcinolone | VSS and VAS | VSS: 9.75 ± 0.43; VAS: 2.5 ± 2.4 | \ |
| Park 2024 ( | Combined continuous wave and repetitive fractionated CO2 laser | \ | MVSS, POSAS, Recurrence rate, and Overall patient satisfaction | MVSS: 3.5 ± 0.3; POSAS: 1.9 ± 0.3; Recurrence rate: 4.35%; Overall patient satisfaction:4.5 ± 0.5 | MVSS: 3.7 ± 0.5; POSAS: 2.7 ± 0.4; Recurrence rate: 12.5%; Overall patient satisfaction:4.4 ± 0.6 |
| Aristides 2024 ( | Fractional carbon dioxide laser + 5-aminolevulinic acid photodynamic therapy | \ | VSS | 1.7 ± 2.1 | \ |
| Study | Intervention of the experimental group | Intervention of the controlled group | Outcomes | Indicators of outcome (experimental group) | Indicators of outcome (controlled group) |
|---|---|---|---|---|---|
| Wen 2021 ( | Hypofractionated radiotherapy | \ | Efficacy | 0.848 | \ |
| Arnault 2009 ( | Iridium 192* brachytherapy | \ | Recurrence rate | 0.236 | \ |
| Bijlard 2017 ( | High-dose-rate brachytherapy | \ | Recurrence rate | 0.083 | \ |
| Lee 2015 ( | 6-MeV electron beam | \ | Recurrence rate | 0.1891 | \ |
| Bischof 2007 ( | 6-MeV electron beam radiotherapy | \ | Recurrence rate | 0.85 | \ |
| Clavere 1997 ( | Iridium 192 brachytherapy | \ | Efficacy | 0.63 | \ |
| BERMAN 2020 ( | Superficial Radiation Therapy | \ | Efficacy | 85.6% | \ |
| Barragan 2022 ( | Interstitial high-dose-rate brachytherapy | \ | Efficacy | 71% | \ |
| Jiang 2015 ( | Interstitial high-dose-rate brachytherapy | \ | Efficacy | 94% | \ |
| Jiang 2017 ( | Interstitial high-dose-rate brachytherapy | \ | Efficacy | 92% | \ |
| Guix 2001 ( | Interstitial high-dose-rate brachytherapy | \ | Recurrence rate | 4.7% | \ |
| Hafkamp 2017 ( | Interstitial high-dose-rate brachytherapy | \ | Efficacy/Recurrence rate | 76%/24.1% | \ |
| Maemoto 2020 ( | Electron beam radiation therapy | \ | Recurrence rate | 68% | \ |
| Ogawa 2002 ( | Electron beam radiation therapy | \ | Recurrence rate | 33.33% | \ |
| Song 2014 ( | Single-fraction radiotherapy | \ | Recurrence rate | 0% | \ |
| Shen 2015 ( | Hypofractionated electron-beam radiation | \ | Efficacy and Recurrence rate | 88.25%/9.59% | \ |
| Ahmad 2017 ( | Iridium-192 high-dose rate surface mould brachytherapy | \ | Efficacy | 89.5% | \ |
| Sruthi 2017 ( | Single-fraction radiation | \ | Recurrence rate | 16.2% | \ |
| Son 2020 ( | A single dose of low-energy superficial X-ray radiation | \ | Recurrence rate | 6.25% | \ |
| VIANI 2009 ( | Strontium 90 brachytherapy | \ | Recurrence rate and efficacy | 12.4%/70.6% | \ |
| Hoang 2016 ( | Interstitial high dose rate brachytherapy | excision alone/external beam radiotherapy | Recurrence rate | 0.23 | 54%/19% |
| Cicco 2013 ( | High-dose-rate interstitial brachytherapy | low-dose-rate interstitial brachytherapy | Recurrence rate | 38% | 30.4% |
| Study | Intervention of the experimental group | Intervention of the controlled group | outcomes | Indicators of outcome (experimental group) | Indicators of outcome (controlled group) |
|---|---|---|---|---|---|
| Manjunath 2021 ( | Surgical Excision and Adjuvant High-dose Rate Brachytherapy | \ | Recurrence rate | 0.02 | \ |
| Escarmant 1993 ( | Iridium 192 interstitial irradiation after surgical excision | \ | Efficacy | 0.8 | \ |
| Ogawa 2014 ( | Surgical excision and radiotherapy | \ | Recurrence rate | 4.8% | \ |
| Ollstein 1981 ( | Combined surgical excision and immediate X-ray therapy | \ | Recurrence rate | 28% | \ |
| Ragoowansi 2002 ( | Surgical excision and immediate single-fraction radiotherapy | \ | Recurrence rate | 16% | \ |
| Weshay 2015 ( | Combination of radiofrequency and intralesional steroids (10 mg/mL) | \ | Volume reduction/Recurrence rate | 95.42 ± 7.62/10% | \ |
| Emad 2010 ( | Surgical excision and radiotherapy | Cryotherapy and intralesional steroid | efficacy and tolerability | 0.818 | 0.719 |
| Kaushal 2020 ( | Combined intralesional radiofrequency and intralesional triamcinolone acetonide | Intralesional triamcinolone acetonide alone | Efficacy | 0.9 | 0.867 |
| Li 2024 ( | Keloid-cross-flap surgery and radiotherapy | Keloid-cross-flap surgery and compression therapy | Recurrence rate | 13.56% | 28.81% |
| Khan 2025 ( | Surgical excision and radiotherapy | \ | Recurrence rate | 65% | \ |
| Study | Intervention of the experimental group | Intervention of the controlled group | Outcomes | Indicators of outcome (experimental group) | Indicators of outcome (controlled group) |
|---|---|---|---|---|---|
| Antipyrimidine monotherapy | |||||
| Li 2022 ( | Excision followed by 5-FU and betamethasone intralesional injections | 5-FU and betamethasone intralesional injections/excision followed by radiotherapy | VSS and POAS | 0.5516 | 37.11%/54.11% |
| Reinholz 2020 ( | Intralesional 5-fluorouracil (50 mg/mL) in combination with triamcinolone acetonide (40 mg/mL) | \ | improvement in POSAS | 39% | \ |
| Khalid 2018 ( | Intralesional 5-FU/TA injections | Radiotherapy | Efficacy | 0.7333 | 0.4333 |
| Erlendsson 2022 ( | A pneumatic jet injection with 5-fluorouracil and triamcinolone acetonide | 5-FU + TA | Improvement in VSS | 55% | 25% |
| Sharma 2021 ( | Intralesional 5-FU and triamcinolone acetonide | Combination of intralesional bleomycin and triamcinolone acetonide | Efficacy | 93.33% | 93.33% |
| Srivastava 2018 ( | Intralesional triamcinolone acetonide (40 mg/mL) and 5-fluorouracil (50 mg/mL) | Intralesional triamcinolone acetonide (40 mg/mL)/intralesional 5-fluorouracil (50 mg/ml) | VSS | 0.3 ± 0.47 | 0.61 ± 0.45/0.2 ± 0.41 |
| Sabry 2019 ( | CO2 laser and topically applied 5-FU | CO2 laser and topically applied verapamil hydrochloride/ablative fractional CO2 laser monotherapy | VSS | 5.33 ± 1.6 | 4.3 ± 1.5/1.89 ± 1.05 |
| Tawfik 2019 ( | Combined 5-fluorouracil and fractional erbium YAG laser | Topical 5-fluorouracil cream | VSS | 2.17 ± 1.11 | 4 ± 1.76 |
| Levenberg 2020 ( | Intralesional 5FU and corticosteroids | \ | VSS improvement rate | 0.53 | \ |
| Monteiro 2022 ( | Intralesional 5 Fluorouracil (50 mg/mL) | Combination of 5 Fluorouracil (50 mg/mL) with Triamcinolone Acetonide (40 mg/mL) | Efficacy | \ | \ |
| Davison 2009 ( | 5-FU + steroid with excision | 5FU + steroid without excision/steroid treatment with excision | Reduction area of Keloids | 0.92 | 81%/73% |
| Antipyrimidine combination therapy | |||||
| George 2005 ( | Intralesional 5-fluorouracil | \ | Recurrence rate | 0.3 | \ |
| Study | Intervention of the experimental group | Intervention of the controlled group | Outcomes | Indicators of outcome (experimental group) | Indicators of outcome (controlled group) |
|---|---|---|---|---|---|
| Bleomycin monotherapy | |||||
| Espana 2001 ( | Bleomycin | \ | Efficacy | 100 | \ |
| Moravej 2022 ( | Intralesional bleomycin (1.5 mg/mL) | Intralesional triamcinolone (20 mg/mL) | Reduction area of Keloids | 0.615 | 0.655 |
| Saray 2005 ( | Dermojet injections of bleomycin (1.5 IU/mL) | \ | Efficacy | 100% | \ |
| Khan 2019 ( | Intralesional bleomycine | Intralesional triamcinolone | Improvement in POSAS | 26 ± 11.91 | 34 ± 12.28 |
| Bleomycin combination therapy | |||||
| Ramadan 2021 ( | Pulsed Nd: YAG laser and intralesional bleomycin | Pulsed Nd: YAG laser only | Efficacy | 1 | 0.8 |
| Luo 2023 ( | The combined application of bleomycin and triamcinolone | \ | Recurrence rate | 6.9–7.9% | \ |
| Study | Intervention of the experimental group | Intervention of the controlled group | Outcomes | Indicators of outcome (experimental group) | Indicators of outcome (controlled group) |
|---|---|---|---|---|---|
| Verapamil monotherapy | |||||
| Ahuja 2013 ( | Intralesional verapamil hydrochloride (concentration 2.5 mg/mL) | Intralesional triamcinolone acetonide (concentration 40 mg/mL) | VSS | \ | \ |
| Abedini 2018 ( | Intralesional verapamil (2.5 mg/mL) | Intralesional corticosteroids (40 mg/mL) | VSS | 11.08 ± 0.94 | 3.9 ± 1.23 |
| Verapamil combination therapy | |||||
| Kant 2018 ( | Triamcinolone and verapamil | \ | Patient, Observer, and POSAS scores | \ | \ |
| Copcu 2004 ( | Combination of Surgery and Intralesional Verapamil Injection | \ | Patient satisfaction (1–10) | 6.4 | \ |
| Dogahe 2023 ( | Intralesional triamcinolone (40 mg/mL) and verapamil (2.5 mg/mL) | Intralesional triamcinolone alone (40 mg/mL) | VSS | 1.5 ± 0.6 | 4.1 ± 1.9 |
| Khattab 2019 ( | Intralesional verapamil alone 2.5 mg/mL. | Combination of PDL and intralesional verapamil alone 2.5 mg/ml | VSS and PSS | 0.27 ± 0.7 | 0.13 ± 0.35 |
| Study | Intervention of the experimental group | Intervention of the controlled group | Outcomes | Indicators of outcome (experimental group) | Indicators of outcome (controlled group) |
|---|---|---|---|---|---|
| Copcu 2004 ( | Combination of Surgery and Intralesional Verapamil Injection | \ | Patient satisfaction (1–10) | 6.4 | \ |
| Manjunath 2021 ( | Surgical Excision and Adjuvant High-dose Rate Brachytherapy | \ | Recurrence rate | 0.02 | \ |
| Aljodah 2021 ( | Combination of Surgical Excision and Perioperative Corticosteroid Injection (40 mg/mL) | \ | Recurrence rate | 9.6% | \ |
| Ogawa 2014 ( | Surgical excision and radiotherapy | \ | Recurrence rate | 4.8% | \ |
| Ollstein 1981 ( | Combined surgical excision and immediate X-ray therapy | \ | Recurrence rate | 28% | \ |
| Ragoowansi 2002 ( | Surgical Excision and immediate single-fraction radiotherapy | \ | Recurrence rate | 84% | \ |
| Stewart 2006 ( | The combination of surgical excision with the application of topical mitomycin-C | \ | Efficacy | 0.9 | \ |
| Wang 2020 ( | Combined surgical excision and electron external beam radiation | \ | Recurrence rate | 0.086 | \ |
| Emad 2010 ( | Surgical excision and radiotherapy | Cryotherapy and intralesional steroid | Efficacy and tolerability | 0.818 | 0.719 |
| Hou 2023 ( | Punch Excision Combined With Intralesional Steroid Injection | Intralesional Steroid Injection alone | VSS and POSAS | \ | \ |
| Qiao 2017 ( | Surgery combined with lucortriticod and electron irradiation group | Efficacy | 0.975 | 52.5%/80%/82.5% |
| Study | Intervention of the experimental group | Intervention of the controlled group | Outcomes | Indicators of outcome (experimental group) | Indicators of outcome (controlled group) |
|---|---|---|---|---|---|
| Intralesional cryosurgery monotherapy | |||||
| Chopinaud 2014 ( | Intralesional Cryosurgery | \ | Reduction area of Keloids | 0.585 | \ |
| Bijlard 2018 ( | Intralesional cryotherapy | Excision with corticosteroid injections or brachytherapy | POSA | \ | \ |
| Leeuwen 2014 ( | Intralesional Cryotherapy | \ | Recurrence rate | 0.24 | \ |
| Abdel-Meguid 2014 ( | Intralesional cryosurgery | Contact cryosurgery | Efficacy | 0.87 | 0.6 |
| Intralesional cryosurgery combination therapy | |||||
| Weshahy 2012 ( | Combined intralesional cryosurgery and intralesional steroid injection | \ | Reduction area of Keloids | 0.935 | \ |
| Nishi 2022 ( | Combination of cryotherapy with intralesional corticosteroid | Combination of fractional CO2 laser followed by topical corticosteroids | MSS | 15.67 | 12.56 |
| Yosipovitch 2009 ( | Cryotherapy and steroid injection | Cryotherapy alone/Steroid injection | Thickness, pain, and itch | 7.7 ± 4.2 mm | 3.1 ± 2.2 mm/−0.25 ± 1.2 mm |
| Zouboulis 2020 ( | Combined liquid nitrogen contact cryosurgery with intralesional corticosteroids | liquid nitrogen contact cryosurgery | Efficacy | 90% | 83.3% |
| Stromps 2013 ( | Intralesional cryotherapy combined with postoperative silicone gel sheeting | Intralesional cryotherapy alone | Efficacy | \ | \ |
| Study | Intervention of the experimental group | Intervention of the controlled group | Outcomes | Indicators of outcome (experimental group) | Indicators of outcome (controlled group) |
|---|---|---|---|---|---|
| Topical monotherapy | |||||
| Martin-Garcia 2005 | Imiquimod 5% Cream | \ | Recurrence rate | 0.25 | \ |
| Berman 2002 ( | Imiquimod 5% cream | \ | Recurrence rate | 0% | \ |
| Nor 2016 ( | Either daily topical clobetasol propionate 0.05% cream under occlusion with a silicone dressing | Monthly intralesional triamcinolone injection | POSAS | 26(IQR 18–44) | 31(IQR 18–39) |
| Chernoff 2007 ( | Dermatix gel | Silicone gel sheeting | elevation of the scars | 0.79 mm | 1.39 mm |
| Meseci 2019 ( | Topical corticosteroid ointment | Untreated | MVSS | 2.5(0–11) | 4(1–10) |
| Francesca 2010 ( | Self-Drying Silicone Gel | POSA | 2.48 | 2.55 | |
| Topical combination therapy | |||||
| Dina 2021 ( | Combined fractional ablative 2,940 nm Er: YAG laser and topical application of steroid cream | Intralesional corticosteroid injection | VSS | 2.07 ± 2.02 | 2.63 ± 2.09 |
| Study | Intervention of the experimental group | Intervention of the controlled group | Outcomes | Indicators of outcome (experimental group) | Indicators of outcome (controlled group) |
|---|---|---|---|---|---|
| Chen 2020 ( | Continuous tension reduction | \ | Recurrence rate | 7.90% | \ |
| SONG 2018 ( | hyperbaric oxygen therapy | Surgical excision and radiotherapy | Recurrence rate | 5.97% | 14.15% |
| Shaarawy 2014 ( | Intralesional botulinum toxin type A | Intralesional steroid | efficacy | 0.827 | 0.792 |
| Suwanchinda 2022 ( | Cold atmospheric-pressure plasma | Untreated | efficacy | 0.944 | \ |
| Neinaa 2021 ( | Intralesional injection of botulinum toxin type-A (5 IU/injection point) | Intralesional injection of platelet rich plasma (0.1 mL/injection point)/Intralesional injection of triamcinolone acetonide (20 mg/session) | efficacy | 0.85 | 85%/35% |
| Berman 1997 ( | Interferon alfa-2b | excision alone/injection with triamcinolone acetonide | Recurrence rate | 0.187 | 51.2%/58.5% |
| Seo 2011 ( | Topical and intralesional mitomycin C (1 mg/mL) | \ | VSS | \ | \ |
| Pazyar 2024 ( | Intralesional vitamin D injection | Intralesional triamcinolone injection | VSS | 6.91 ± 2.5 | 4.59 ± 1.4 |
| Harsono 2023 ( | Intralesional injection of umbilical cord Mesenchymal stem cells | Intralesional injection of triamcinolone acetonide | POSAS | 3.5(2–4) | 1(0–3) |
| Lim 2024 ( | Small interfering RNA microneedle patches | Silicone sheets | Percentage reduction in scar volume | 83.78 ± 15.39 | 74.11 ± 21.6 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsDermatologic Treatments and Research · Laser Applications in Dentistry and Medicine · Body Contouring and Surgery
Introduction
Hypertrophic scars and keloids represent pathological skin conditions resulting from abnormal wound healing mechanisms (1). Keloids develop at sites of trauma or infection and are more common in areas of the skin with increased tensile tension and frequent activity (such as the torso, upper arm/shoulder (deltoid area), and knees) (2, 3). The clinical features of keloid are raised but smooth surface scars, hard on palpation, and hypopigmentation and hyperpigmentation. It may be accompanied by symptoms such as itching and pain (3). Because of its potential psychological and physical adverse effects, patients’ quality of life may be impaired (4).
The combination of cells and chemicals promotes and completes the normal tissue repair process. During normal scar healing, collagen production and degradation are usually balanced. In keloids and hypertrophic scars, this balance is disrupted, with increased collagen synthesis and decreased collagen degradation (5). Collagen accumulates in the lesion, leading to excessive scar tissue. Hypertrophic scars and keloid formation are associated with patient age, family history, pregnancy, injury site, secondary trauma, post-injury infection, burn, and tension suture (6, 7). Genetic predisposition and cutaneous injury are major contributors to keloid pathogenesis (6). The incidence is 4.5 to 16% in blacks and Hispanics (6), with lighter skin tone being a protective factor, affecting whites ranging from 5 to 37% (8). Recurrence of keloid and hypertrophic scars after treatment is a major clinical challenge (9).
Clinically and pathologically, there are some differences between keloids and hypertrophic scars (7). Keloids are clinically characterized by raised lesions that extend beyond the original wound margins and do not spontaneously regress (10). The onset time is several months after the injury, and the growth appears to be gradual and undefined. Although keloids vary in size and shape, most are associated with itching and burning. Hypertrophic scars are generally growths less than 1 cm wide that grow in the original skin lesion area. It usually occurs about 4 weeks after the original injury and grows strongly over several months, resolving itself within a year (7).
No universally accepted treatment standard exists, and the effectiveness of available interventions remains controversial (9). Combined interventions are the current routine option for both types of scar treatment (1, 11). Although evidence of superiority is inconclusive, combined modalities frequently exhibit synergistic or complementary effects or are applied sequentially at different treatment stages. Principal therapeutic approaches include pharmacotherapy, pressure therapy, surgical excision, radiotherapy, and light-based therapies (12). Corticosteroids are considered first-line drug therapy for the treatment of hypertrophic scars and keloids, and are the most commonly used option for intralesional administration (11). Other intrafocal drug treatment options include bleomycin (6) and 5-fluorouracil (5-FU) (10). Topical drug forms include gels, creams, sprays, or flexible gel tablets (6). Cryosurgery and scar removal are currently available surgical procedures that may be useful. Cryotherapy techniques lead to scar tissue necrosis by reducing blood flow (6, 13). Scar excision includes the removal of the core of the scar or the overall removal of the scar (11). Light source therapy includes intense pulsed light (IPL) therapy and laser therapy. IPL is designed to promote vascular ischemia and interfere with collagen production (14), whereas laser therapy reduces scar volume by targeted tissue ablation (6, 13).
Despite numerous therapeutic options, diagnosis remains challenging, and recurrence rates remain high. Clinical diagnostic accuracy for keloids has been reported at approximately 81% (15). The recurrence rate in patients treated with surgical resection alone is 70 to 100% (16). With an in-depth understanding of the pathological mechanisms of keloid, the range of related treatment methods is increasingly enriched. For example, the important role of vitamin D in the synthesis and degradation of collagen in the treatment of skin fibrosis diseases such as scleroderma (17); Intralesional corticosteroid injection, cryotherapy, pressure therapy, radiotherapy, laser therapy, onion extract, topical imiquimod cream, bleomycin, interferon and photodynamic therapy were used to inhibit collagen synthesis in keloid tissue (18); The sHLA-E profile may inform trials evaluating systemic agents, such as monoclonal antibodies, in combination with local therapies (19).
Given the multiplicity of interventions and the absence of a definitive gold standard, a systematic review that synthesizes indications, methodologies, and clinical efficacy of available therapies is warranted.
Methods
Research design
The present systematic review was conducted according to the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-analyses statement) (20).
Search strategy and data sources
We searched PubMed, EMBASE, Cochrane and Web of Science with a pre-designed search strategy in April 2025 to retrieve all relevant clinical trials, using the following search strategy: [‘keloid’ and (‘occlusive dressings’ or ‘imiquimod’ or ‘steroids’ or ‘mitomycin’ or ‘fluorouracil’, ‘interferons’ or ‘bleomycin’ or ‘surgical procedures, operative’ or ‘cryotherapy’, ‘radiotherapy’ or ‘lasers, dye’ or ‘platelet-rich plasma’)], as well as other relevant key words (Supplementary Table 1). Additional searches using the terms ‘Antigens, CD’ and ‘MicroRNAs’ were conducted to identify studies addressing the molecular mechanisms associated with keloid and hypertrophic scars. The detailed search strategy for all databases is reported in Supplementary Table 1. The reference lists of relevant articles and reviews were screened for additional eligible studies, and manual searches were performed as necessary. Each study was assessed by two independent reviewers, and disagreements were resolved by discussion with a third reviewer.
Inclusion and exclusion criteria
Our selection criteria were generated based on the PICOS principle as follows.
Inclusion criteria:
P: Patients with a clinical diagnosis of keloid or hypertrophic scar;
I: Intervention groups or control groups received any anti-keloid treatment;
C: No restriction on the intervention of control groups;
O: Studies detailed the treatment strategy or molecular mechanisms for keloid, and provided outcome indicators such as clinical remission rate, scar area improvement, and scar score scale to evaluate the treatment effect;
S: Single-arm or controlled design for treatment-related studies and no restrictions on molecular mechanisms-related studies;
Language: studies published in English.
Exclusion criteria:
Ineligible study design, such as case series, observational studies, commentary, conference abstracts;Essential data were absent from studies, although authors were emailed to obtain it;Older duplicate reports published by the same team based on the same group of participants;Studies included ineligible participants, such as participants with hypertrophic scars or dermatofibrosarcoma protuberans.
Data extraction
Data were extracted into a pre-designed Excel spreadsheet. Paired independent reviewers extracted study data and resolved disagreements by discussion or consultation with a third reviewer. For studies with missing data, we contacted the authors to request the necessary information as the remaining data were publicly available as reported in this study. The characteristics of the included studies are summarized as follows: name of the first author, year of publication, study country, study design, clinical diagnosis, sample size, mean age, intervention of experimental group, intervention of controlled group, radiotherapy parameter, follow-up period, treatment evaluation tool, treatment evaluation outcomes (experimental group and controlled group), and main conclusion.
Quality assessment
Based on the different study designs of the included studies, we selected two different scales for quality assessment. The RoB2 (21) was selected to assess the risk of bias and quality of evidence of the 48 included RCTs. The MINORS (22) was used to evaluate the potential bias and quality of the remaining 101 non-randomized trials. Quality assessment was conducted by two investigators.
RoB2 assessed bias across domains, including the randomization process, deviations from intended interventions, missing outcome data, measurement of the outcome, and selection of the reported result. MINORS consists of a total of 12 programs, requiring a study with a clear purpose, inclusion of consecutive patients, prospective data collection, selection of endpoints appropriate for the purpose of the study, unbiased evaluation of the endpoints, matching the primary endpoint for the follow-up period, follow-up loss less than 5%, and prospective calculation of the sample size. Articles 9 through 12 provide additional criteria for evaluating control studies, including selection of the gold standard as intervention for the control group, baseline equivalence between groups, and statistical analysis consistent with the study design. Each MINORS item is scored 0–2 (0 = not reported, 1 = reported inadequately, 2 = reported adequately), yielding a maximum score of 24 for comparative studies (Figure 1).
Flowchart of the study selection.
Results
Results of study selection
In total, 13,571 articles were identified in electronic and manual searches. However, 3,015 articles were excluded for duplication. A total of 2,750 studies were excluded because their study designs did not fulfill the established inclusion criteria. This exclusion comprised 745 meeting abstracts, 954 reviews, 83 editorials, 265 case reports, 87 meta-analyses, 254 letters, 98 notes, and 264 studies of other designs. After excluding 5,964 studies for irrelevant results and 1,638 studies with inapplicable participants, a total of 204 studies were screened for full-text evaluation. Ultimately, 162 studies concentrated on treatment methodologies, while eight studies examined mechanisms of action (17–19, 23–27); both categories were included in the systematic review.
Study characteristics
The basic characteristics of the 162 included full-text studies are presented in Table 1. The main conclusions of these studies were summarized in Table 2. One hundred sixty-two studies were conducted in 30 countries, most of them were performed in China (n = 23), Egypt (n = 19), the USA (n = 16), India (n = 14), Iran (n = 14), and Korea (n = 13). Some studies have been published in Japan (n = 6), Thailand (n = 6), Germany (n = 5), Netherlands (n = 5), France (n = 4), Spain (n = 4), Turkey (n = 4), Pakistan (n = 3), Brazil (n = 3), England (n = 3), Israel (n = 3), Singapore (n = 3), Iraq (n = 2), and Italy (n = 2). The remaining 10 studies were conducted Canada, Greece, Chile, Finland, Ghana, Malaysia, Indonesia, Mexico and Denmark. Study designs comprised 75 cohort studies, 52 randomized controlled trials (RCTs), 25 retrospective studies, and 10 prospective studies. Of the 162 studies, 112 targeted the population with keloids, 17 included patients with hypertrophic scars, 28 included people with keloids and hypertrophic scars, and 5 studied included patients with keloids or hypertrophic scars. A total of 9,510 patients with keloid and/or hypertrophic scars were included in our analysis, with sample sizes ranging from 6 to 612 per study. Most patients were young adults with a mean age of 30.69 years, and the mean age of patients included in every single study ranged from 12 to 60.18 years. The follow-up period of the included studies varied widely, ranging from 1 month to 10 years. Due to the diversity of treatment modalities included in the studies, study outcome measures also varied greatly, and most studies only assessed the efficacy of treatment regimens and/or the impact on recurrence rates (n = 88). Twenty-four of the included studies assessed scars at each stage using the Vancouver Scar Scale (VSS) (28). Furthermore, a limited number of studies employed single scar assessment scales, including Manchester Scar Scale (MSS), Modified Vancouver Scar Scale (MVSS), Patient and Observer Scar Assessment Scale (POSAS), Patient Scar Assessment Scale (PSAS), Stony Brook Scar Evaluation Scale (SBSES), and Japan Scar Workshop Scar Scale (JSS), or utilized a combination of multiple outcome indicators to evaluate the efficacy of treatment.
The treatment options for keloid and hypertrophic scar included in the study could be roughly divided into monotherapy (MT) and combination therapy, of which 80 were monotherapy studies, and 82 were combination therapy (CT) studies (72 studies with double combined therapy and 10 studies with triple combined therapy). From the classification of intervention methods, the treatment methods we retrieved included: Corticosteroid therapy [e.g., triamcinolone acetonide (TA)] (MT = 11; CT = 40), optical therapy (IPL or laser) (MT = 17; CT = 29), radiation therapy (MT = 22; CT = 12), antipyrimidine therapy [5-fluorouracil (5-FU)] (MT = 2; CT = 10), anticancer drug therapy (bleomycin) (MT = 4; CT = 2), calcium channel blocker therapy (verapamil) (MT = 3; CT = 3), surgical resection (MT = 0; CT = 15), topical therapy (gel or cream) (MT = 9; CT = 2), cryosurgery (MT = 4; CT = 5), botulinum toxin (MT = 2; CT = 2), interferon (MT = 1; CT = 1) and other physical therapy (MT = 3; CT = 0). Furthermore, two studies investigated two newer monotherapy approaches: intralesional vitamin D injection (29) and intralesional injection of umbilical cord mesenchymal stem cells (30).
Study quality
Quality assessment of 52 RCTs using RoB2 classified 36 studies as having low risk of bias and 16 studies as having some concerns. Ten of the 16 studies raised concerns due to a substantial proportion of missing outcome variables. Four studies were classified as at risk of bias due to the subjective nature of their outcome measures, while two studies demonstrated potential selective bias in outcome reporting (Supplementary Table 2 and Figure 2).
Quality assessment result for included randomized controlled trials (RCT) studies.
Of 110 nonrandomized studies assessed with MINORS, 34 were comparative, and 75 were uncontrolled. Among comparative studies, 31 were rated as high quality (≥18) and 3 as moderate quality (14–17). All 75 uncontrolled studies were rated as high quality (≥12). The limitations of controlled studies mirror those of single-arm studies, including improper selection of study endpoints and short follow-up periods (Supplementary Table 3).
Hormone monotherapy
TA is a topical (skin) steroid drug used to treat different skin conditions (31). TA is currently considered to be the primary intrafocal treatment for keloid and hypertrophic scars (31). The study demonstrated that local injections of TA alone proved to be a potentially effective and safe treatment (32, 33). Eleven of the studies included in this review involved TA monotherapy. Eight of the 11 studies confirmed the efficacy of TA monotherapy, and one small sample study also confirmed that TA has an anti-recurrence effect comparable to radiotherapy (31) and is very effective in the treatment of keloids in children (33). Studies of the timing of administration have shown that the treatment efficacy was better when applied during the static stage of pathological scarring rather than the early stage (34). Advances in delivery, such as TA-loaded dissolving microneedle patches, showed promising results (35) (Table 3).
However, results from six comparative studies showing the efficacy of TA alone remain controversial. The results of Darougheh’s study showed that although TA alone was as effective as the combination of 5-FU, the combination treatment was more acceptable to patients and therefore achieved better results (3). A small sample study published in 2019 showed that verapamil was less effective than TA in the VSS score for the treatment of keloids (36). Conversely, a 2021 cohort study of 160 patients concluded that although TA monotherapy had no significant side effects, plaque verapamil was the most effective treatment (patient observer scar assessment scale (POSAS) 29 ± 10.91 vs. 36 ± 12.74) (37). Such differences may be due to differences in outcome measures, with VSS assessing thickness and POSAS using surface area, which also takes into account the patient’s perception of symptoms (38). Second, two RCT studies with similar publication years and similar sample sizes reached opposite conclusions about the efficacy of TA and 5-FU. The results of the Hietanen 2018 (39) study showed no statistically significant difference in 6-month response rates between the 5-FU and TA groups (46 and 60%, respectively). Sadeghinia 2012 (35) found that at 44 weeks of follow-up, erythema, pruritus, height, surface, and induration were improved in both groups, but the improvement was more significant in the 5-FU group (p < 0.05). This may be due to the difference in the length of follow-up, and the efficacy and repeatability of TA monotherapeutics need to be further investigated.
Hormone combination therapy
There were 38 of the included studies that discussed the efficacy of corticosteroid hormones in the treatment of keloid and hypertrophic scars. There were 36 of the included studies that discussed the efficacy of corticosteroid hormones in the treatment of keloid and hypertrophic scars. Similar to hormonal monotherapy regimens, TA was the corticosteroid of choice in most of the studies (n = 21), and the remaining 17 studies used a combination regimen of intralesional steroid injections (Table 4).
The 21 studies that examined the TA combination included 6 single-arm studies and 11 controlled studies. The results of single-arm studies were consistent, showing that the TA combined regimen could effectively treat keloid and hypertrophic scar. These programs include TA in combination with bleomycin (n = 2), TA in combination with pulsed dye laser (PDL)/copper bromide laser (n = 5), and TA in combination with 5-FU (n = 1). Among them, Kim 2022 (40) confirmed that early intervention of PDL combined with TA can prevent recurrence or progression after hypertrophic scar resection. The results of the 5-FU combined TA cohort study measured the ratio of drug combinations, and the combination treatment was well tolerated at a ratio of 3:1 and stable at 1 year (41). The selection of TA combination regimen in controlled studies is relatively rich, and all studies confirm the superiority of the combination regimen over monotherapy. The included TA combination regimen includes laser combination (fractional CO_2_ laser, non-ablative fractional laser, PDL) (n = 3) (42–44), surgical combination (excision and freezing) (n = 2) (45, 46), and 5-FU combination (n = 2) (47, 48), botulinum toxin type A combination (n = 2) (49, 50), bleomycin combination (n = 1) (51), verapamil combination (n = 1) (52), interferon-α combination (n = 1) (53), and platelet-rich plasma combination (n = 1) (54).
Among the 17 other corticosteroid injection regimens included in the analysis were: surgical combination (excision and freezing) (n = 7), optical combination (laser and IPL) (n = 6), 5-FU combination (n = 1), Cynthaskin combination (n = 1), thermomechanical fractional injury-assisted (n = 1), and radiofrequency (n = 1). Heterogeneity of the study conclusions was observed in the hormone combination laser study. Three of the four combined laser studies confirmed the efficacy of the fractional CO_2_ laser (55), the 1,064 nm neodymium-doped yttrium aluminum garnet laser (Nd: YAG) (56), and the 578 nm copper bromide laser combined with corticosteroid hormones (57), respectively. Son 2014 also proposed that laser therapy reduced the telangiectasia side effects of intrafocal corticosteroid injections (57). However, the results of the RCT study published in 2021 with a follow-up period of 6 months showed that local corticosteroids and monotherapy with fractional laser (4 times, 28 J/cm^2^, pulse width 300 us, and 5% density) have no long-term synergistic effect on the thickness reduction of abdominal hypertrophic scars (58). This disagreement may be due to differences in laser mode, but it should also be considered in clinical practice that laser therapy may be a better choice than intralesional corticosteroid injection for patients with thicker scars.
Optical monotherapy
The number of studies on optical monotherapy included was 17, and the study time span was large, from 1989 to 2021. With the update of instruments, the treatment depth, treatment density, and energy density of optical therapy continued to increase. The pulse energy density has increased from 6.5 to 8.0 J/cm2 in 1999 (59) to 20–150 mJ/cm^2^ in 2021 (60). However, the available optical therapy methods have considerable limitations, mainly concentrated in all types of laser therapy [pulsed dye laser (PDL), bare-fiber diode laser, Nd: YAG laser, and carbon dioxide laser (CO_2_ laser)] and IPL treatment (14). These optical therapies have been reported to have significant effects on the long-term improvement in the appearance of hypertrophic scars. The results of controlled studies confirmed that laser therapy for keloid and hypertrophic scars performed as well as cryosurgery (61–63), verapamil (64), radiofrequency therapy (37), and silicone gel sheeting (59) in terms of efficacy and anti-recurrence. The pigmentation and erythema values improved significantly after early treatment, and the elasticity values were the lowest after late treatment (65). The only concern was the results of a single-arm study published in 1989 (66) that showed that carbon dioxide laser excision, in either continuous or 0.2 s pulse mode with an average intensity of 12 W, was not effective in treating earlobe keloids. Given the technical capacity and level of evidence at the time of publication, we believe that such results are of limited significance as a guide to clinical practice today (Table 5).
Optical combination therapy
Research on optical combination therapy has mostly been published between 2019 and 2024, focusing on the combination of new technologies that have gradually matured in recent years. Combination treatment regimens include: IPL combined with laser (n = 5), IPL combined with corticosteroid hormones (n = 5), laser combined with bleomycin (n = 1), 5-FU (n = 3), botulinum toxin A (n = 1), and corticosteroid hormones (n = 12) (Table 6).
Nine single-arm studies have confirmed the preventive and therapeutic effects of laser combined with corticosteroid hormone (67), laser combined with 5-FU (68) and IPL combined hormone (40, 69) on keloid and hypertrophic scar (57). Adjuvant use of the 578 nm CO_2_ laser reduced the telangiectasia side effect of intrafocal corticosteroid injection (57), but the effect was slower and required 3 to 4 courses to reduce the scar VSS score by 50% (70).
The results of 14 controlled studies showed that the treatment effect of laser combined with IPL, laser combined with corticosteroid hormone, laser combined with botulinum toxin A, and laser combined with 5-FU were all better than that of laser or other monotherapy. Notably, the results of a small sample RCT study published in 2020 showed that the combination of the two laser modes (fractional and Nd YAG) in the same course of treatment did not add significant additional benefit and had higher side effects (VSS: 45.63 ± 21.34; PSASA: 44.92 ± 10.13) (71).
Radiation monotherapy
The radiation therapy regimen was the only regimen in this search in which monotherapy was significantly more than combination therapy. This is mainly because almost all radiation therapy is used as an adjunctive treatment option after surgical resection to aid in the recovery and later management of keloids (Table 7).
Of the 22 radiation monotherapy regimens included, 20 were single-arm studies, all of which confirmed the efficacy and safety of radiation therapy in the adjuvant treatment of postoperative keloids and hypertrophic scars. These adjuvant treatment options include: hypofractionated radiotherapy (n = 1), Iridium 192* brachytherapy (n = 3), high-dose-rate Brachytherapy (n = 6), 6-MeV electron beam (n = 2), Superficial Radiation Therapy (n = 2), electron beam radiation therapy (n = 3), single-fraction radiotherapy (n = 2), and strontium 90 brachytherapy (n = 1).
These studies of monotherapy with radiation have highlighted several key points related to treatment: (1) perioperative high-dose brachytherapy for keloid was effective, with a recurrence rate of only 4.9% (72); (2) Brachytherapy can be used as a remedy after external radiation therapy and other treatment methods have failed (73, 74); (3) Early postoperative radiotherapy is a good choice for keloid treatment (48–72 h) (75, 76); (4) Recent studies have shown that, for example, a single dose of low-energy superficial X-ray radiation (single dose of 50 kV superficial radiation of 8 Gy administered on average 34 days) is sufficient to inhibit keloid recurrence (77).
One of the two controlled studies included in the review supplemented the results of the single-arm study. A 2013 Cicco (78) study found that low-dose-rate interstitial brachytherapy (LDR) and high-dose-rate interstitial brachytherapy (HDR) had similar recurrence rates. However, the HDR treatment regimen provided better symptom relief than the LDR regimen. However, another controlled study contradicted the conclusions of the one-arm study: the results of the Hoang 2016 study (79) showed that keloid recurrence of external beam radiotherapy was significantly later than that of interstitial high dose rate brachytherapy.
Radiation combination therapy
There are two types of combined treatment of radiotherapy: one is as postoperative adjuvant treatment, and the other is combined with corticosteroid hormones. Radiotherapy regimens used in combination regimens include HDR, Iridium 192 interstitial irradiation, X-ray therapy, single-fraction radiotherapy, and radiofrequency. The greatest benefit of radiation combination therapies is to control the recurrence of keloid and hypertrophic scars. The rate of recurrence control with this protocol as an adjunctive postoperative treatment gradually decreased from 28% in 1981 (combined surgical excision and immediate X-ray therapy) (80) to 0.02% in 2021 (combined surgical excision and adjuvant HDR) (81). The researchers believe that a postoperative sterile environment created by radiotherapy is an important condition for recurrence control (82). Given the significant influence of scar repair on patient satisfaction, recent research has sought to incorporate advancements in plastic surgery into procedures that combine surgical intervention with radiotherapy. For instance, studies have demonstrated that the application of innovative super-tension suture technology to alleviate skin tension can effectively decrease the rate of postoperative recurrence (83). At the same time, the scar treatment effect and tolerance of excision surgery combined with radiotherapy were better than that of cryotherapy combined with corticosteroids (efficacy: 0.818 vs. 0.719) (84). Furthermore, underdeveloped surgical and radiotherapy techniques may significantly influence treatment outcomes. A limited retrospective study conducted on Pakistani patients, published in 2025, revealed that the postoperative recurrence rate following the combination of surgery and radiotherapy was as high as 65% (85) (Table 8).
Antipyrimidine therapy
5-fluorouracil is the first antimetabolic drug synthesized according to certain assumptions and is the most widely used antipyrimidine drug in the clinic. It has good efficacy in digestive tract cancer and other solid tumors, and plays an important role in medical oncology. This treatment mode has fewer cases of single drug use (n = 1), and more combined with glucocorticoids (TA) (n = 7), which has better, faster efficacy and fewer side effects than glucocorticoids alone (48) (Table 9).
There has also been a gradual increase in the number of new joint programs in recent years. Surgical resection combined with 5-FU is an effective treatment for ear keloids (45). The VSS score of laser combined with 5-FU was better than that of laser or 5-FU monotherapy (64, 86). However, the comparative results also showed that patients treated with a combination of bleomycin and triamcinolone within the lesion experienced greater improvements in keloid signs and symptoms (regarding cosmetic problems, mobility limitations, and tenderness) than patients treated with a combination of 5-FU and triamcinolone (51).
Bleomycin therapy
Bleomycin belongs to the glycopeptide antibiotic family, which has potent antitumor activity against a variety of lymphomas, head and neck cancers, and germ cell tumors. A small number of studies were retrieved, including four monotherapies and two combination therapies (Table 10).
Bleomycin monotherapy is administered locally and intrafocally, and four studies have confirmed its efficacy. In the comparative study with intralesional triamcinolone, bleomycin had the same effect as TA in reducing scar area (87) and was better than the TA in improving the POSAS score (88). However, its adverse reactions, such as pain, ulceration, and pigmentation, should not be ignored and should be used with caution (87).
Combined administration studies have shown that bleomycin combined with TA can effectively treat keloid and hypertrophic scar, with a recurrence rate of 6.9 to 7.9% (89). Combined intrafocal bleomycin therapy is a promising approach compared to long-pulse Nd-YAG laser monotherapy (efficacy: 100% vs. 80%) (90).
Verapamil therapy
Verapamil is a calcium channel blocker. It was introduced as a coronary dilator in 1962. In recent years, it has been used to treat hypertension, cardiovascular and cerebrovascular diseases, pulmonary hypertension, and prevent premature birth (91). Intralesional injection was used to treat keloids, and the number of relevant studies was relatively small. We retrieved 2 studies on monotherapy and 4 studies on combination therapy (Table 11).
The results of monotherapy studies do not support verapamil’s ability to treat keloid and hypertrophic scars alone (VSS: 11.08 ± 0.94 vs. 3.9 ± 1.23) (91), although it is less costly and has fewer side effects than TA (92).
The results of the controlled study showed that the efficacy of verapamil combination therapy was highly recognized (93), and the efficacy of the combination with TA was long-term stable and better than that of TA alone (52). Combined surgery or PDL is also a good choice for clinical treatment, but the number of studies and samples is small, and further research support is needed (94, 95).
Perioperative adjuvant therapy
Perioperative adjuvant treatment options have been discussed in the above review of various treatment options, and many adjuvant treatment options are considered to be effective in preventing postoperative keloid formation and recurrence. The adjuvant treatment options we searched included: radiotherapy (X-ray therapy, HDR, single-fraction radiotherapy, electron external beam radiation) (n = 6), perioperative corticosteroid injection (n = 2), verapamil (n = 1), and topical mitomycin-C (n = 1) (96). Two other controlled studies compared the effectiveness of different combination treatment regimens. Results of a cohort study involving 160 patients with earlobe keloid showed that in the treatment of ear scar, the efficacy of surgery combined with glucocorticoid and electron irradiation group was superior to surgery combined with local injection of glucocorticoid group, equivalent to surgery combined with superficial X-ray group, and superior to surgery group (97) (Table 12).
Intralesional cryosurgery
Intralesional Cryosurgery is a safe and effective new treatment that differs from traditional resection, so we summarized the relevant findings separately. It causes minimal damage to the skin surface by destroying hypertrophic scar tissue (98) (Table 13).
The results of monotherapy studies suggest that intrafocal freezing is superior to contact freezing in terms of efficacy and safety (99), and can reduce the volume, pain, and pruritus of primary scars (100, 101). However, in the treatment of refractory keloids, the efficacy is not as good as excision surgery combined with radiotherapy (101). Combined therapy studies have shown that the adjuvant effect of hormones is not significant when freezing combined hormones, but the effect is better than monotherapy (102–104).
Topical therapy
Topical therapy is frequently employed for mild keloid and hypertrophic scar treatment, including facial (105) and postcesarean scars (106). The number of relevant studies searched in this study was limited, mainly monotherapy (n = 6), and there was only 1 study of combination therapy (107) (Table 14).
Topical therapies studied included 5% imiquimod cream (n = 2), 0.05% clobetasol propionate cream (n = 1), dermatix gel (n = 1), topical corticosteroid ointment (n = 1), and facial treatment self-drying silicone gel (n = 1). 5% imiquimod cream for keloid can achieve a very low recurrence rate (0–25%) (108, 109). Clobetasol 0.05% propionate cream has fewer adverse reactions than triamcinolone (110). However, the topical corticosteroid ointment group had the same effect as the untreated ointment group [MVSS:2.5 (0–11) vs. 4 (1–10)] (105).
Other monotherapy
In addition to the above treatment regimens, we also identified seven other studies related to monotherapy. Seven studies included 6 different rare treatment options: continuous tension reduction (111), hyperbaric oxygen therapy (112), intralesional botulinum toxin type A (BTX-A) (113, 114), cold atmospheric-pressure plasma (CAP) (115), interferon alfa-2b and topical (116) and intralesional mitomycin C (117), intralesional vitamin D injection (29), small interfering RNA microneedle patches (118), and intralesional injection of umbilical cord mesenchymal stem cells (30) (Table 15).
Continuous tension reduction and hyperbaric oxygen therapy both achieved lower recurrence rates (7.8 and 5.97%) (111, 112). The CAP technique can provide mild to moderate scarring improvement with minimal side effects (115). Compared to traditional TA injections, BTX-A has better cosmetic results in the treatment of keloids (113, 114). Interferon alfa-2b injection at the site of keloidectomy can be an effective postoperative adjuvant therapy (116). Recent studies have investigated the efficacy of innovative therapies for keloids, demonstrating that siRNA microneedle patches can significantly reduce scar volume (118). Additionally, intralesional injection of umbilical cord mesenchymal stem cells has demonstrated potential effectiveness in the treatment of keloids; however, further studies with extended follow-up periods are necessary to assess its cost-effectiveness (30). Limited supporting evidence for these interventions limits their applicability for clinical guidance.
Triple combination therapy
Considering the propensity of keloid and hypertrophic scars for recurrence and the current absence of a gold standard therapy, the study results demonstrated that multimodal combination therapy achieves long-term remission (119). Therefore, with the advent of multiple treatment schemes, multimodal combined treatment schemes emerged. The pertinent treatments identified in this study can be classified into two categories: triple therapy incorporating surgical resection and intralesional corticosteroid injection (n = 5), and triple therapy involving intralesional corticosteroid injection in conjunction with 5-FU (n = 5).
There were 4 triple treatments based on surgical resection combined with intralesional corticosteroid injection included in this review, and they were combined with three different physiotherapy methods: ablative CO_2_ laser (n = 1) (119), shaving (n = 1) (120) and local pressure (n = 2) (121, 122), respectively. As an adjunctive treatment after surgery, they all helped patients achieve good efficacy and recurrence control (efficacy: 0.824/0.9167; recurrence rate: 12.5%) (119–122), but the scheme to combine local pressure was seen as too inefficient and a lengthy and time-consuming process for both doctors and patients (122).
The construction concept of the triple therapy regimen, based on intrafocal corticosteroid injection combined with 5-FU, is to reduce the recurrence of small keloids after local injection of triamcinolone and 5-fluorouracil (123). Therefore, the combination regimen of radiotherapy (Strontium-90 brachytherapy) (123) and laser therapy [1,064-nm Nd: YAG laser (124) or PDL (3)] was chosen. Combined radiotherapy reduced the recurrence rate of TA combined with local injection of 5-FU by about 40% (44.4% vs. 85.7%) (123).
Discussion
This review included 162 articles evaluating therapeutic interventions for keloid and hypertrophic scars. The included studies described and compared multiple monotherapy and combination regimens, including intralesional corticosteroid injection, optical therapies, radiotherapy, 5-FU therapy, bleomycin, verapamil, surgical excision, cryotherapy, topical treatments, other monotherapies, and triple-modality regimens. This qualitative systematic review synthesizes nearly all available clinical treatment studies for keloids and hypertrophic scars since 1981. Unfortunately, due to the lack of a gold standard in this area, the included studies are highly personalized, and quantitative comparison of the efficacy of various treatment methods is not supported at this time. Even so, through a systematic review, we can still find that, with the advancement of technology, the treatment options for this disease are gradually expanding, but various combination treatment options still center on local corticosteroid injection, excision surgery, laser, and radiation therapy. At present, the main difficulty in treating keloids and hypertrophic scars is controlling recurrence. Studies have shown that multimodal combined therapy is more effective than monotherapy in solving this problem.
The mechanisms of physical interventions such as phototherapy and surgical procedures for keloid and hypertrophic scar treatment are relatively straightforward. Intralesional corticosteroids (e.g., TA) exert anti-inflammatory and antifibrotic effects by suppressing fibroblast proliferation and collagen synthesis (31, 89). Antimetabolites such as 5-fluorouracil inhibit fibroblast growth through interference with DNA synthesis (41, 47), while bleomycin induces DNA strand breaks, arresting cell division (89, 125–127). Verapamil, a calcium-channel blocker, may modulate extracellular matrix remodeling by influencing collagenase activity (37). Physical modalities, including laser/IPL (6, 13, 14), radiotherapy (78, 128), cryotherapy (6, 13), and surgical excision (11), act via direct tissue ablation, inhibition of proliferating cells, or physical removal of scar tissue. The observed superiority of combination regimens likely stems from complementary mechanisms that simultaneously target different pathways in scar pathogenesis. Therefore, this discussion elaborates on disease recurrence mechanisms and the pharmacological principles of major therapeutic agents (intralesional TA, 5-FU, bleomycin, and verapamil). Post-treatment recurrence rates represent a primary impetus for investigating intralesional TA as an alternative therapeutic strategy. Long-term follow-up investigations indicate that recurrence rates associated with TA monotherapy or combination therapy range from 5 to 7% over 2–5 years (31, 89).
Keloid and hypertrophic scars, as pathological scar tissue secondary to skin trauma or spontaneous overgrowth, demonstrate therapeutic resistance and elevated post-treatment recurrence rates similar to neoplastic diseases (129). Clinical studies have shown that mono-mode treatment and inadequate treatment (not according to the course of treatment or insufficient dosage) are high-risk factors for keloid recurrence (89). The researchers found that, during keloid treatment, the drug has a temporary effect and is difficult to penetrate the scar. The recurrence rate of keloid with a larger scar area and thicker hyperplasia is higher than that of a smaller scar. This may be caused by inadequate administration or insufficient coverage of medications (89). The recurrence rate of keloid with a larger scar area and thicker hyperplasia is higher than that of a smaller scar. This may be caused by inadequate administration of the drug in some areas or insufficient coverage of the drug. The high recurrence rate after treatment is also the main reason the search for alternatives to intralesional TA has never stopped, despite its widespread use. Furthermore, researchers speculate that the above dilemma may be caused by high heterogeneity among cases, and differences in race, local tissue tension, infections, and even different endocrine environments may affect the traits and prognosis of the disease (130–132). Thus, several studies have provided further insight into the pathogenesis and possible biomarkers of the disease. Recently, S1P-induced signal transduction has been associated with increased collagen synthesis in keloid tissues via S1PR-mediated signaling pathways (17). In terms of genetic and epigenetic aspects of keloid, studies have found that sHLA-E (18), PAI-1, and VDR (19) can effectively be used as diagnostic markers to assess the risk of keloid formation, among which sHLA-E has the potential to be a prognostic marker for clinical outcomes of localized treatment (18). Molecular mechanism studies have shown that EGFR/miR-370-3p/ LCC-GLB1L-1, ITGB5/miR-204/ LCC-Casp9-3 (23), and Hsa_circ_0043688 (25) may be involved in the pathogenesis of keloid. By analyzing the differences in gene expression between keloid and normal dermal fibroblasts through gene profiling, we found that differential expression of the HOX gene (24) and downregulation of Smad7 via MeCP2 may play a role in keloid development (27). Recent studies have also found that five central genes, CHI3L1, IL1RN, MMP7, TNFAIP3, and TNFAIP6, are associated with keloid recurrence (26).
Keloid and hypertrophic scar are tumor-like diseases, and the attempt of antitumor drugs to treat these diseases is also a topic of interest to researchers. As an intralesional TA combination regimen, bleomycin has been found to reduce keloid volume and inhibit keloid recurrence when used in combination with bleomycin (89). Bleomycin can bind to the DNA of the cell, break the DNA chain, and block cell division and proliferation. The M-stage cells are the most sensitive to bleomycin (125, 126). Bleomycin’s role in disrupting cell division in fibroblasts has also been demonstrated in vitro (127).
The pyrimidine analogue 5-FU has also been selected as a TA combination therapy, and its therapeutic effect on keloid and hypertrophic scar is also derived from the inhibition of fibroblast proliferation (41). Studies have shown that the combination of 5-fluorouracil and corticosteroids has a faster clinical response and fewer side effects than single-drug therapy (47). Meanwhile, long-term follow-up results indicated that the two-year recurrence rate of intralesional 5-FU monotherapy could be reduced to 3% (133). At present, the discussion on the administration ratio and regimen of combination therapy is the focus of relevant studies, and the regimen with a 5-FU ratio of TA equal to 3:1 is the conclusion that researchers generally tend to reach (41, 47).
Finally, verapamil is a calcium channel blocker that promotes collagen breakdown by reducing the expression of MMP-9 and vascular endothelial growth factor in keloid tissues, preventing the synthesis and secretion of collagen and fibronectin (extracellular matrix molecules) (37). However, the research results we retrieved only support the application of verapamil as an adjuvant therapy, and the efficacy of a single drug in the treatment of scar remains doubtful (91, 95). Furthermore, the clinical research results of some new therapies, such as botulinum toxin type A, biologics (dupilumab), and interferon (interferon alfa-2b), are also very encouraging. Due to the small number of studies and sample sizes, it is still unable to shake the status of mainstream treatment. However, until the gold standard of care for keloids and hypertrophic scars is established, designing stability and cost-effective protocols to compare traditional treatment (relative to corticosteroid therapy and excision) and new therapies remains the focus of head-to-head trials.
It is imperative to note that previous studies have reported concerning long-term recurrence rates associated with physics-based radiotherapy, surgical resection, and laser therapies. Six studies included in the analysis reported recurrence rates ranging from 2 to 10 years for both combined modalities of radiotherapy and surgery or as standalone treatments. Notably, the recurrence rate following carbon dioxide laser ablation alone may reach as high as 100% within a 2-year period (61). Furthermore, the implementation of continuous tension reduction has been shown to decrease the recurrence rate by 92.1% (111). The recurrence rate for radiotherapy was documented at 38% within 2 years (78), escalating to between 60 and 80% over a 5 to 10-year timeframe (128, 134). Previous studies have indicated that the declining trend in local control rates of lesions following physical interventions is associated with the presence of multiple lesions and the delineation of scar boundaries. This phenomenon parallels the relationship observed between drug dosage and therapeutic efficacy in localized pharmacological treatments. Consequently, future research should undertake a comprehensive investigation into the impact of the local treatment area on both the therapeutic outcomes and recurrence rates of keloids and hypertrophic scars.
As for combination therapy, the ‘S2k guidelines for the therapy of pathological scars (hypertrophic scars and keloids) – Update 2020’ provided a set of treatment algorithms based on scar size, treatment difficulty, and erythema persistence. Non-active flat keloid scars with small areas can be treated with TA and/or cryosurgery. A combination of TA and cryosurgery and 5FU or surgery with follow-up treatment is recommended for further refractory keloid. On this basis, the pulsed dye laser should be considered for persistent erythema. For narrow-base refractory keloids, excision and mandatory follow-up treatment (compression /TA/ cryosurgery/radiation, plus appropriate conservative local treatment) or local cryosurgery are recommended. Local treatment was currently the main treatment for the disseminated and confluent refractory keloids (135). Although this guideline puts forward a detailed treatment algorithm, a number of reviewed studies, including the guideline itself, believed that the preferred treatment method for keloid scars cannot be standardized (136). The need for keloid treatment and the issue of personalized therapeutic goals limited the design and development of standardized clinical trials to a certain extent. At present, there are few high-quality, large-sample RCTs evaluating different treatment methods of keloids. Most evidence supporting keloid therapy consists of retrospective cohorts, prospective cohorts, and systematic reviews. Designing reliable trials to investigate keloid treatment modalities requires a standardized set of experimental methods. Such an approach requires that studies accurately identify keloid populations, design consistent indicators for evaluating treatment quality, and apply validated scar assessment tools. Therefore, the accumulation of treatment plans based on high-quality studies with reproducible outcomes is the difficulty and direction of progress in the field of keloid diagnosis and treatment.
A critical appraisal reveals marked heterogeneity across studies in design, patient populations, interventions, outcome measures, and follow-up duration, which limits pooled comparison and weakens causal inference. Evidence strength is highest for intralesional corticosteroids, radiotherapy as a surgical adjuvant, and several laser modalities because multiple controlled studies and long-term cohorts support their efficacy; however, many trials report variable endpoints and incomplete reporting. Combination regimens consistently outperform monotherapies, yet optimal combinations, dosing ratios, and sequencing remain undefined. Future trials must standardize diagnostic criteria, adopt validated scar scales (e.g., VSS, POSAS), ensure adequate follow-up, and prioritize randomized, adequately powered designs to reduce heterogeneity and strengthen evidence.
Optimal multimodal therapy may vary by anatomical site. For example, earlobe keloids, given their small size and low tension, often respond well to surgical excision combined with adjuvant intralesional steroids or radiation. Conversely, keloids on the chest or shoulders may require tension-relieving techniques in addition to antiproliferative therapies. Regarding specific laser and steroid parameters, current evidence does not define a single optimal protocol; studies report wide variations in laser settings (e.g., fluence, density) and triamcinolone concentrations (10–40 mg/mL) (42, 58, 70). Future studies should aim to standardize these parameters to establish more precise treatment guidelines.
Limitation
This systematic review integrates a substantial portion of the existing literature and employs the MINOR and ROB2 checklist criteria for quality assessment; however, several potential limitations warrant acknowledgment. First, the study’s inclusion criteria were restricted to English-language publications, which may introduce bias into the comprehensive evaluation results, particularly given that the incidence of keloids and hypertrophic scars is influenced by racial factors. Secondly, conference abstracts, which frequently appear in contemporary research on treatment approaches, were excluded, potentially resulting in the omission of some of the latest therapeutic modalities. Thirdly, there is a notable lack of discussion of the potential short- and long-term side effects of treating keloids and hypertrophic scars. This oversight may be attributed to the localized nature of the interventions employed. Nevertheless, given the possible adverse effects of long-term treatments, such as corticosteroids, it is essential that future research more thoroughly examine the potential safety risks involved. Moreover, the review has limited analytical depth and lacks a quantitative synthesis of the findings, making it challenging to draw definitive conclusions regarding the effectiveness of various treatment strategies. Furthermore, in the absence of a gold standard for the treatment of keloids and hypertrophic scars, there is considerable variability in treatment modalities and outcome variables across different studies, which hinders the quantitative synthesis of analytical results. This study, therefore, provides only a qualitative summary of the evidence. Although a range of treatment methods has been reviewed, a uniform conclusion regarding their efficacy remains elusive. Consequently, the findings presented in this study should be interpreted with caution.
Conclusion
This systematic review synthesizes existing literature on treatment modalities and outcomes for keloid and hypertrophic scars. Following a qualitative analysis of 162 studies, we conclude that intralesional glucocorticoid injection, excisional surgery, and laser therapy represent the three most frequently employed treatment strategies. Multimodal combination therapy is often regarded as superior to monotherapy for mitigating recurrence rates. Proper administration and adherence to treatment protocols are crucial for ensuring favorable prognoses. Currently, standardized management guidelines for keloid treatment remain absent. The development of standardized trial protocols for keloid treatment, informed by quantitative evidence-based medical investigation, is essential for accumulating robust evidence in future studies.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Bouzari N Davis SC Nouri K. Laser treatment of keloids and hypertrophic scars. Int J Dermatol. (2007) 46:80–8. doi: 10.1111/j.1365-4632.2007.03104.x 17214728 · doi ↗ · pubmed ↗
- 2Köse O Waseem A. Keloids and hypertrophic scars: are they two different sides of the same coin? Dermatologic Surg. (2008) 34:336–46. doi: 10.1111/j.1524-4725.2007.34067.x, 18177398 · doi ↗ · pubmed ↗
- 3Asilian A Darougheh A Shariati F. New combination of triamcinolone, 5-fluorouracil, and pulsed-dye laser for treatment of keloid and hypertrophic scars. Dermatologic Surg. (2006) 32:907–15. doi: 10.1111/j.1524-4725.2006.32195.x 16875473 · doi ↗ · pubmed ↗
- 4Bock O Schmid-Ott G Malewski P Mrowietz U. Quality of life of patients with keloid and hypertrophic scarring. Arch Dermatol Res. (2006) 297:433–8. doi: 10.1007/s 00403-006-0651-716528552 · doi ↗ · pubmed ↗
- 5Cho SB Lee JH Lee SH Lee SJ Bang D Oh SH. Efficacy and safety of 1064-nm Q-switched Nd:YAG laser with low fluence for keloids and hypertrophic scars. J Eur Acad Dermatol Venereol. (2010) 24:1070–4. doi: 10.1111/j.1468-3083.2010.03593.x, 20158584 · doi ↗ · pubmed ↗
- 6Alster TS Tanzi EL. Hypertrophic scars and keloids: etiology and management. Am J Clin Dermatol. (2003) 4:235–43. doi: 10.2165/00128071-200304040-00003 12680802 · doi ↗ · pubmed ↗
- 7Seifert O Mrowietz U. Keloid scarring: bench and bedside. Arch Dermatol Res. (2009) 301:259–72. doi: 10.1007/s 00403-009-0952-8, 19360429 · doi ↗ · pubmed ↗
- 8Li-Tsang CW Lau JC Chan CC. Prevalence of hypertrophic scar formation and its characteristics among the Chinese population. Burns. (2005) 31:610–6. doi: 10.1016/j.burns.2005.01.022 15993306 · doi ↗ · pubmed ↗