Nine Metachronous Cancers Primarily Involving the Head and Neck: A Case Report
Atsushi Miyauchi, Shuichi Matsumoto, Hiroaki Ito, Masamitsu Hyodo, Masanori Teshima

TL;DR
A 62-year-old man developed nine cancers mainly in the head and neck area, highlighting the need for long-term monitoring in cancer survivors.
Contribution
This case report highlights the importance of continuous surveillance for new cancers in long-term survivors of multiple primary malignancies.
Findings
Multiple primary cancers were detected at early stages through extensive surveillance.
Minimally invasive resections contributed to long-term survival.
New malignancies can emerge years after initial cancer treatments.
Abstract
A 62-year-old man presented with multiple malignant tumors, predominantly involving the head and neck region, including the esophagus, gum, oropharynx, larynx, lungs, and stomach. Histopathological analysis revealed that while the majority of the tumors were squamous cell carcinomas, other types including spindle cell carcinoma, mucoepidermoid carcinoma, and adenocarcinoma were also identified. Oropharyngeal cancer and oral cancer developed within a previously irradiated field from treatment 10 years prior. All subsequent primary tumors were detected at early stages through extensive multimodal surveillance, allowing for minimally invasive curative resections and contributing to long-term survival. This case underscores the necessity of lifelong, continuous monitoring for survivors of multiple primary cancers, as new malignancies can emerge long after initial treatments.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
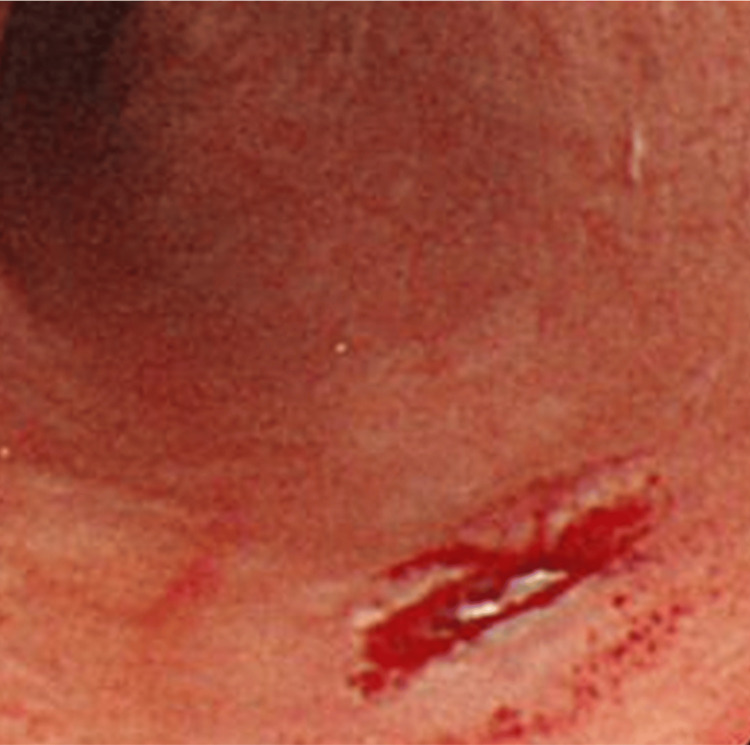 Figure 1
Figure 1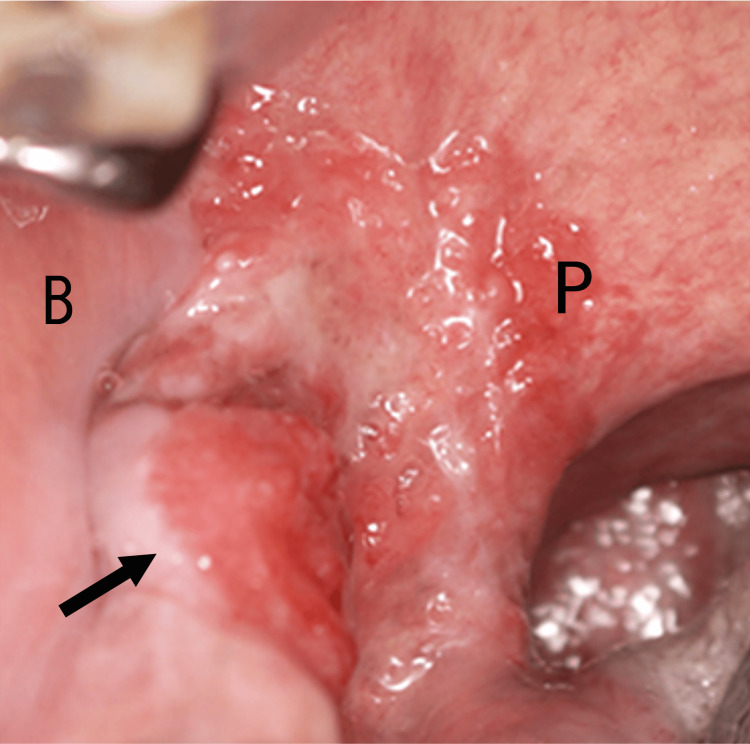 Figure 2
Figure 2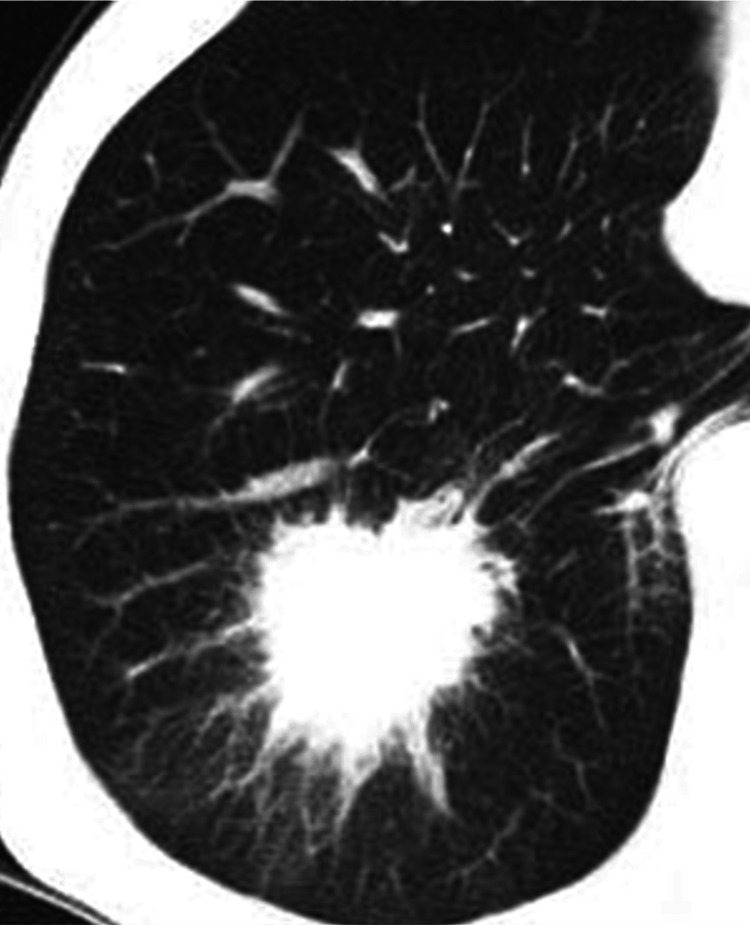 Figure 3
Figure 3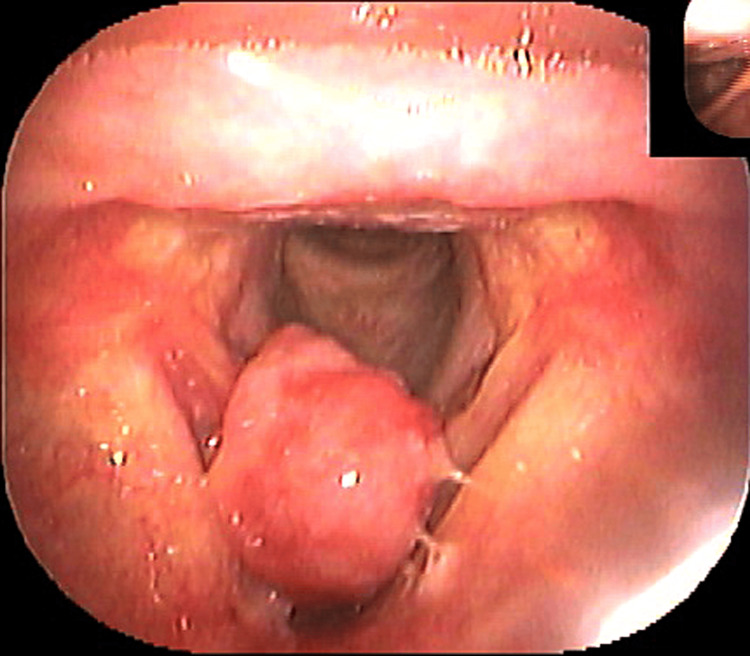 Figure 4
Figure 4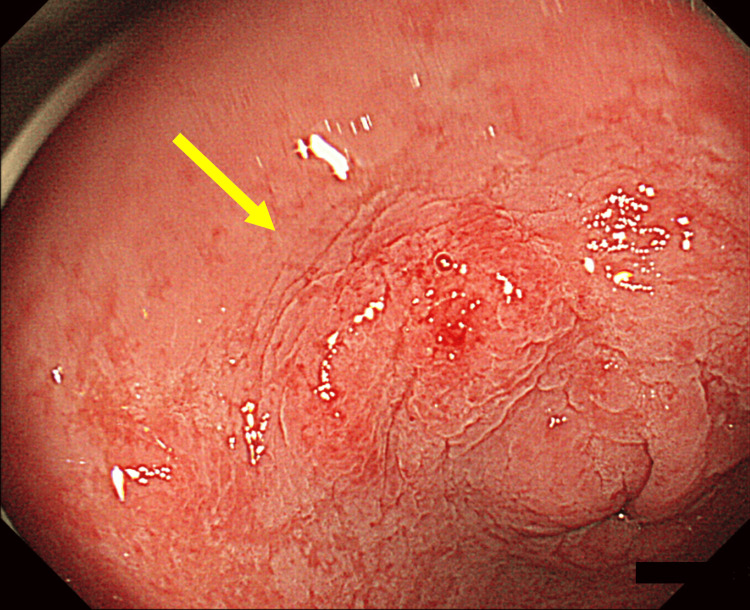 Figure 5
Figure 5 Figure 6
Figure 6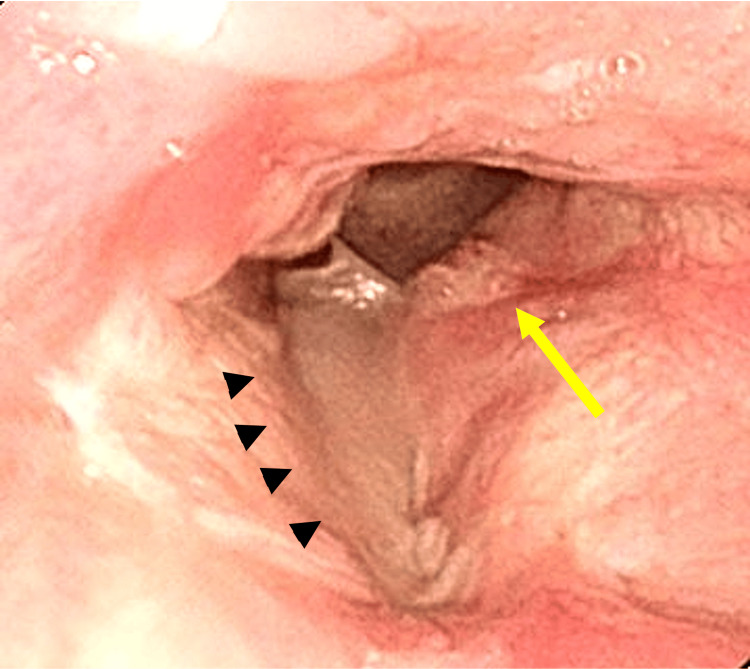 Figure 7
Figure 7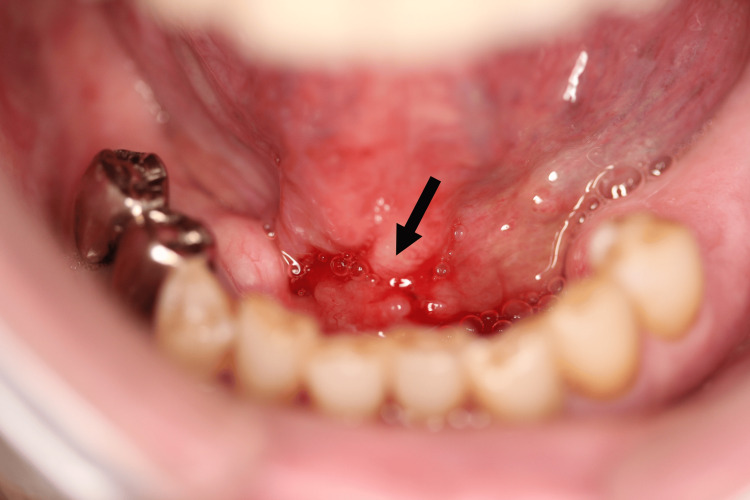 Figure 8
Figure 8 Figure 9
Figure 9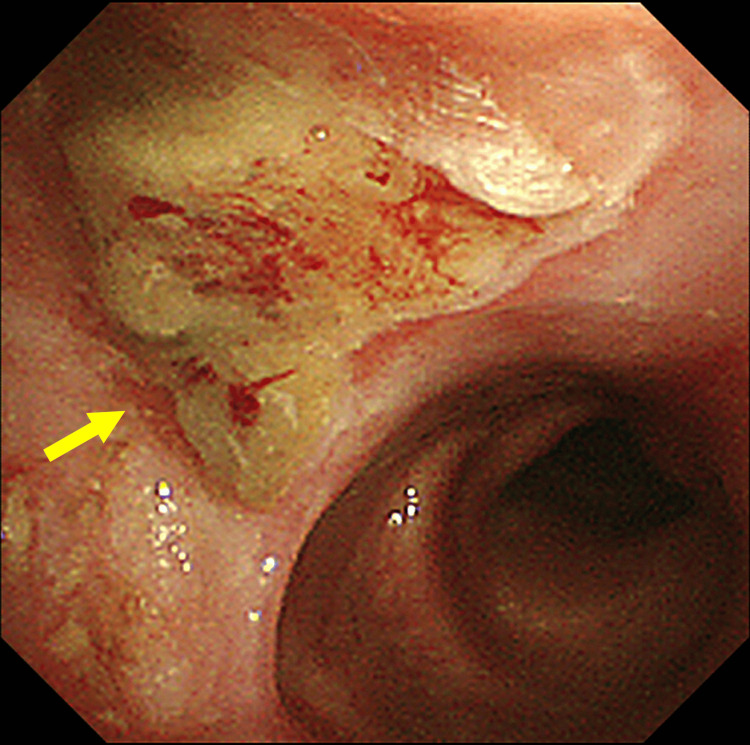 Figure 10
Figure 10| Interval from 1st cancer | Site | Location | Diagnosis | TNM | Pathology | Treatment | Outcome | |
| 1st | 62-year-old | Esophagus | Thoracal | Gastrointestinal endoscope | Tis | Squamous cell carcinoma | Endoscopic resection | Recurrence three times within four years: Endoscopic resection of each |
| 2nd | 1Y | Oral | Right lower gingiva | Clinical finding | T2N0M0 | Squamous cell carcinoma | Chemoradiotherapy: Radiation 40Gy Chemotherapy: CBDCA 900mg, S-1 120mg 4 weeks, peplomycin 40mg | |
| 3rd | 6Y | Lung | Right lower lobe | CT scan | T2N0M0 | Squamous cell carcinoma | Surgery: Right lower lobectomy adjuvant chemotherapy: UFT 400mg/day for two years | |
| 4th | 10Y | Larynx | Right vocal cord | Laryngoscope | T1aN0M0 | Spindle cell carcinoma | Surgery: Resection direct laryngoscopy | Recurrence: Vertical partial laryngectomy |
| 5th | 10Y9M | Stomach | Antrum | Gastrointestinal endoscope | T1aN0M0 | Adenocarcinoma | Endoscopic resection | |
| 6th | 12Y6M | Oropharynx | Right soft palate | Gastrointestinal endoscope | T1N0M0 | Squamous cell carcinoma | Surgery: Transoral CO2 laser resection | |
| 7th | 13Y6M | Larynx | Left vocal cord | PET-CT | T1aN0M0 | Squamous cell carcinoma | Surgery: CO2 laser resection direct laryngoscopy | |
| 8th | 15Y7M | Oral | Floor of mouth | PET-CT | T1N0M0 | Mucoepidermoid carcinoma, Grade III (High grade) | Surgery: Transoral CO2 laser resection | Recurrence twice: 1Y: First recurrence: Marginal mandibulectomy, right neck dissection; 1Y6M: Second recurrence: Marginal mandibulectomy |
| 9th | 17Y1M | Lung | Right upper lobe | CT scan | T1aN0M0 | Squamous cell carcinoma, Grade 3 | Surgery: Right upper lobectomy | Recurrence: Chemotherapy CBDCA (6AUC) and nab-paclitaxel (100mg/m2): two cycles followed by pembrolizumab 200mg: six cycles |
| 18Y7M | Died of ninth lung cancer recurrence, 18 years after the first cancer. |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMultiple and Secondary Primary Cancers · Head and Neck Cancer Studies · Salivary Gland Tumors Diagnosis and Treatment
Introduction
Advances in cancer treatment and early detection have increased the risk that cancer survivors will develop a second primary cancer [1]. This case report aims to examine the prevalence of second primary cancers in patients with head and neck cancers. Multiple primary cancers are defined according to modified Warren-Gates criteria, where each tumor should present a definite picture of malignancy, each tumor should be histologically distinct with at least 2 cm normal mucosa in between or duration of five years, the possibility that one is a metastasis of other must be excluded, and, additionally, tumors in an interval of more than six months are defined as metachronous [2]. Here, we present the case of a patient who developed nine metachronous primary cancers over 18 years. To our knowledge, such a high number of tumors is scarce; they primarily affected the head, neck, and esophageal regions. This case highlights the clinical importance of lifelong, multi-organ surveillance in patients with field cancerization, demonstrating that even with a high frequency of primary cancers, early detection and appropriate intervention can lead to long-term survival.
Case presentation
The first cancer was found in 2000, when a 62-year-old man had a health check with an upper gastrointestinal endoscopy, which revealed an esophageal lesion that was diagnosed as esophageal cancer, tumor in situ (Tis) (Figure 1).
First esophageal cancerLocated 26 cm from the incisor
The patient had a history of silicosis (due to tunnel work), vibration disease, and 98 pack-years of smoking and 108 g/day of alcohol. Endoscopic mucosal resection was performed. Thereafter, the patient was followed up with upper gastrointestinal endoscopy every few months. Although the esophageal cancer recurred three times over a four-year period, all lesions were superficial and successfully treated with curative endoscopic resection.
The second cancer was found in 2001, when the patient had a leukoplakia on the right lower gingiva, which had been bothering him for a year. As the lesion gradually became erythematous and associated with intermittent localized pain, the patient visited the oral and maxillofacial surgery department in our hospital. Biopsy confirmed oral squamous cell carcinoma as the second oral cancer, T2N0M0, stage II (Figure 2).
Second oral cancer: T2Right lower gingiva (indicated by arrow), B: right buccal P: right palatoglossal arch
The patient underwent chemoradiotherapy. Radiation fields were applied from the lower of maxillary sinus to hyoid bone and performed with 6 MV X-rays total 40 Gy (2 Gy/fraction, once a day, five times a week for four weeks). As concomitant chemotherapy, two cycles of carboplatin (300mg for the first cycle and 600mg for the second cycle), oral S-1 (120mg/day) for four weeks, and bleomycin 5 mg two times a week (eight cycles; total dose 40 mg). The disease was completely cured.
The third cancer was found in 2006. The patient had a CT scan during a routine check-up, which revealed an abnormal shadow in the right lower lung. The patient had no respiratory symptoms, and biopsy under bronchoscopy confirmed squamous cell carcinoma (Figure 3).
Third lung cancer: T2Right lower lobe, characterized by a 45 mm mass lesion
This lesion was considered a newly metachronous third lung cancer, T2N0M0, stage I-B, because five years had passed since the second oral cancer was cured, and the lesion was sporadic and spiculated CT finding. The right lower lobe was resected, and adjuvant chemotherapy with tegafur-uracil (400 mg/day) was administered orally for two years. Thereafter, the patient was followed up with regular clinical examinations, and CT scan and PET-CT were added to monitor for any signs of frequent recurrence or the development of multiple primary cancers.
The fourth cancer was found in 2010, when the patient had a slight hoarseness and sore throat for several months. A few months prior to visiting our department, the patient had a loss of appetite and worsening hoarseness. An upper gastrointestinal endoscopy examination performed at a local clinic revealed a vocal tumor. For further evaluation and treatment, the patient was referred to our department. A pedunculated mass was identified on the right vocal cord (Figure 4).
Fourth laryngeal cancer: T1Right vocal cord
The tumor was resected under direct rigid laryngoscopy, and histopathological diagnosis confirmed spindle cell carcinoma, as the fourth cancer, T1aN0M0, stage I. Recurrence was observed five months later, necessitating vertical laryngectomy, and disease was completely cured.
The fifth cancer was nine months later in 2010, when, after the initial diagnosis of the fourth cancer, an upper gastrointestinal endoscopy during a routine check-up for esophageal cancer identified early gastric cancer (Figure 5).
Fifth stomach cancer: T1aTumor in the antrum (indicated by arrow)
The disease was resected endoscopically, and histopathology diagnosed it as adenocarcinoma, T1aN0M0, stage I.
In 2012, a routine upper gastrointestinal endoscopy revealed an ulcerative lesion in the right lower aspect of the soft palate. The patient had no symptoms and no local pain. A biopsy was performed, and it was diagnosed as oropharyngeal squamous cell carcinoma, as the sixth cancer, T1N0M0, stage I (Figure 6). The lesion was resected via a transoral approach with CO2 laser.
Sixth oropharyngeal cancer: T1Right soft palate (indicated by arrow)
The seventh cancer was found in 2013, when the patient had a PET-CT scan during a routine check-up that revealed an abnormal shadow at the left larynx, and a tumor was detected in the left vocal cord with a laryngoscope (Figure 7).
Seventh laryngeal cancer: T1aTumor of left vocal cord (indicated by arrow), Right vocal cord has been replaced skin graft (arrow head) by vertical laryngectomy for recurrent of fourth laryngeal cancer
The patient had no symptoms with hoarseness and local pain. The lesion was suspicious for recurrence of the fourth laryngeal cancer and was surgically resected. Histopathology confirmed it as squamous cell carcinoma. This lesion was identified as a newly metachronous seventh laryngeal cancer, T1aN0M0, stage I, because it was histologically distinct from the previous fourth laryngeal cancer (spindle cell carcinoma), and the lesion appeared on the opposite side.
The eighth cancer was found in 2015. The patient had a PET-CT scan during a routine check-up, which revealed an abnormal shadow at the tip of the tongue, and an ulcerative lesion with induration was found at the median of the oral floor (Figure 8).
Eighth oral cancer: T1Floor of the mouth (indicated by arrow)
The patient had no symptoms and no local pain. A biopsy diagnosed it as mucoepidermoid carcinoma, constituting the eighth metachronous oral cancer, T1N0M0, stage I. The tumor was locally resected with CO2 laser, and histopathological diagnosis was grade III, high grade. One year after the initial surgery, the first local recurrence was identified. The patient underwent marginal mandibulectomy combined with right neck dissection. Six months later (1.5 years after the initial surgery), a second local recurrence occurred. A repeat marginal mandibulectomy was performed to achieve local control. They were all classified as eighth cancer.
The ninth cancer was found in 2017, when a routine CT checkup for screening of recurrence and new metastasis for prior metachronous cancers revealed a lung tumor in the right upper lobe (Figure 9).
Ninth lung cancer: T1aRight upper lobe, 12 mm spiculated mass lesion (indicated by arrow)
The patient had no respiratory symptoms with hemoptysis. Bronchoscope biopsy confirmed squamous cell carcinoma. This lesion was considered a newly metachronous ninth lung cancer, T1aN0M0, stage I, because more than 10 years had passed since the third right lung cancer, the tumor was located inside the bronchus and originated from bronchial epithelium under bronchoscopy (Figure 10) and the CT finding was sporadic and spiculated pattern. The right upper lobectomy was performed. Seven months later, local recurrence occurred. As systemic chemotherapy, two cycles of carboplatin (AUC 6) and nab-paclitaxel (100 mg/m²) were administered, followed by six cycles of pembrolizumab (200 mg). One year and six months after the recurrence, the patient succumbed to the ninth lung cancer, approximately 18 years after the first cancer (Table 1).
Bronchoscopic findings showing the ninth lung tumorTumor (indicated by arrow) was originated from bronchial epithelium.
Discussion
The incidence of a second primary cancer following an initial diagnosis of cancer is approximately 5 to 10%, which is 1.1 to 1.4-fold higher than in the general population [3-5]. This ratio varies depending on the location of the initial cancer: it is lower than 10% if the initial lesions are liver, pancreatic, and breast cancers, but higher than 10% if colorectal and prostate cancers. Moreover, if oral or pharyngeal lesion, the risk increases by more than 20-fold [3]. Maier et al. reported that when the tobacco index was greater than 50 pack-years, the risk of head and neck cancer increased to 12-to-70-fold, and greater than 75 g daily alcohol intake increased to 12-to-16-fold [6]. This elevated risk in the head and neck regions is explained by the concept of field cancerization [7]: widespread exposure to a carcinogen leads the epithelium to cancer preconditioned change across these areas. Over time, irreversible change progresses to malignancy at multiple points, resulting in metachronous cancers. Furthermore, the molecular analyses have detected genetic alterations in more than 30% of samples in clinically normal mucosa adjacent to head and neck primaries [8]. Vrabec proposed the concept of a 'multicentric zone' encompassing the oral cavity, pharynx, larynx, esophagus, stomach, and lung [9]. Atkinson et al. cited chronic exposure to irritants such as smoking and alcohol as common carcinogenic factors in these ‘multicentric zone’, contributing to the recurrence of multiple secondary cancers [10]. Sung et al. and Chen et al. also found the primary and secondary cancers to occur together within the multicentric zone, with an increased risk ranging from several-fold up to 20-fold for both the initial and subsequent cancers, such as lung, laryngeal and esophageal malignancies [4,11]. In this patient, the lifestyle of 98 pack-years of tobacco and around 108 g daily alcohol strongly implicates these exposures, and multiple metachronous cancers occurred in as many as eight locations within a multicentric zone.
Approximately 40-70% of secondary cancers are diagnosed within five years from the primary cancer diagnosis [3-5], and especially, the first year has the highest incidence of secondary cancers, followed by a gradual decline over time [9]. However, new primaries can still occur more than a decade later, emphasizing the need for vigilance during both the early post-treatment period and the long term. In this patient, while the interval from the second oral cancer to the third lung cancer exceeded five years, others were diagnosed within five years, besides four cases within one year. Owing to careful follow-up, each secondary cancer was detected in early T stage and treated with minimally invasive surgery, supporting prospects for extended survival. Paradoxically, the success of early diagnosis and treatment will eventually lead to an increasing incidence of newly identified multiple primary malignancies; consequently, the occurrence of multiple primary cancers, as seen in this case, will become more common.
Genetic susceptibility may also play a role. Among aldehyde dehydrogenase-2 (ALDH2) polymorphisms, the heterozygous and homozygous deficient variants are associated with facial flushing after consuming small amounts of alcohol. This phenotype is linked to field cancerization in the upper aerodigestive tract [12]. This patient reported flushing, suggesting ALDH2 deficiency. Microsatellite instability and reduced p53 expression have also been linked to multiple primaries [13]. Li-Fraumeni syndrome, driven by germline TP53 alterations, has been reported in two cases involving nine primary tumors, including osteosarcoma, lung cancer, gastric cancer, and leukemia over 20-40 years [14,15]. Several other cases with TP53 germ line mutations have been documented [16], involving sarcoma, brain, leukemias, and other organs. Although genetic testing was not performed in this case and field cancerization due to lifestyle factors within the multicentric zone was prominent, genetic evaluation should be considered in cases of such a high number of primary malignancies.
Radiation-induced cancers are difficult to diagnose clinically. Generally, radiation-induced leukemia occurs five to nine years after exposure and solid tumors often develop 10 years or more [1]. Therefore, a solid tumor should be considered as radiation-induced if it appears more than 10 years after in a previously irradiated area. In the present case, both the sixth oropharyngeal cancer and the eighth oral cancer met the clinical criteria for radiation-induced malignancies associated with the prior chemoradiotherapy for second oral cancer. However, the pathogenesis of the oropharyngeal cancer may also be attributed to the patient’s long-standing lifestyle habits (tobacco and alcohol consumption). Regarding the oral cancer, although it is known that such tumors can arise from minor salivary glands in the oral cavity, it was histologically identified as mucoepidermoid carcinoma - a subtype generally recognized as having a potential association with prior radiation exposure [17]. Even when a patient has a history of radiation therapy, careful attention should be paid to the development of secondary cancers within irradiated fields, even after a latency period exceeding 10 years.
Conclusions
This patient presented with multiple malignant tumors, mainly in the head and neck area, including cancers of the esophagus, gum, oropharynx, larynx, lungs, and stomach. The histology included squamous cell carcinoma, spindle cell carcinoma, mucoepidermoid carcinoma, and adenocarcinoma. According to the locations, histological types, and timing of diagnosis, mostly the disease suggests influences from field cancerization for smoking, alcohol, and radiation-related carcinogenesis. All secondary primary tumors were detected early stage and treated with curative resection. Extensive multimodal surveillance enabled early detection and intervention, supporting long-term survival, and strict follow-up proved advantageous especially in head and neck fields. During routine post-treatment monitoring after an initial cancer diagnosis, clinicians should recognize characteristic patterns and high-risk locations for secondary primary cancers, and prolonged, lifelong monitoring is essential.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1The epidemiology of second primary cancers Cancer Epidemiol Biomarkers Prev Travis LB 202020261520061705702810.1158/1055-9965.EPI-06-0414 · doi ↗ · pubmed ↗
- 2Multiple malignant primary tumors (non-head and neck): contemplation needed J Cancer Res Ther Naorem R Ghogale KS Waghmare CM 0719202310.4103/jcrt.jcrt_155_2238384051 · doi ↗ · pubmed ↗
- 3The relative risk of second primary cancers in Switzerland: a population-based retrospective cohort study BMC Cancer Feller A Matthes KL Bordoni A 512020203196435210.1186/s 12885-019-6452-0PMC 6974968 · doi ↗ · pubmed ↗
- 4Association of first primary cancer with risk of subsequent primary cancer among survivors of adult-onset cancers in the United States JAMA Sung H Hyun N Leach CR Yabroff KR Jemal A 2521253532420203335104110.1001/jama.2020.23130 PMC 7756242 · doi ↗ · pubmed ↗
- 5Incidence and relative risk of metachronous second primary cancers for 16 cancer sites, Osaka, Japan, 2000-2015: population-based analysis Cancer Med Odani S Tabuchi T Nakata K 5075191120223484585210.1002/cam 4.4457 PMC 8729047 · doi ↗ · pubmed ↗
- 6Tobacco and alcohol and the risk of head and neck cancer Clin Investig Maier H Dietz A Gewelke U Heller WD Weidauer H 32032770199210.1007/BF 001846681521046 · doi ↗ · pubmed ↗
- 7“Field cancerization” in oral stratified squamous epithelium. Clinical implications of multicentric origin Cancer Slaughter DP Southwick HW Smejkal W 963968619531309464410.1002/1097-0142(195309)6:5<963::aid-cncr 2820060515>3.0.co;2-q · doi ↗ · pubmed ↗
- 8Persistence of genetically altered fields in head and neck cancer patients: biological and clinical implications Clin Cancer Res Tabor MP Brakenhoff RH van Houten VM 1523153272001 https://pubmed.ncbi.nlm.nih.gov/11410486/11410486 · pubmed ↗