Hypoxic-Ischemic Encephalopathy in Newborns: Pathophysiology, Early Identification, and Management
Maryam S Alhosani, Giorgi Sakvarelidze

TL;DR
This paper reviews hypoxic-ischemic encephalopathy in newborns, focusing on its causes, early detection, and treatment to improve outcomes.
Contribution
The paper provides a comprehensive review of current understanding and management strategies for HIE in newborns.
Findings
Therapeutic hypothermia improves survival and neurodevelopmental outcomes when started within six hours of birth.
Early identification using MRI and aEEG helps determine severity and prognosis of HIE.
Supportive care including seizure control and metabolic management is crucial for comprehensive treatment.
Abstract
Hypoxic-ischemic encephalopathy (HIE) is a severe neurological condition resulting from impaired oxygen delivery and reduced cerebral blood flow to the neonatal brain during the perinatal period. It remains one of the leading causes of neonatal mortality and long-term neurodevelopmental disability worldwide, despite significant advances in obstetric and neonatal care. The pathophysiology of HIE is complex and evolves through a cascade of events beginning with primary energy failure, followed by secondary energy failure characterized by mitochondrial dysfunction, oxidative stress, inflammation, excitotoxicity, and delayed neuronal cell death. Early identification of affected neonates is critical, as timely intervention can significantly influence neurological outcomes. Diagnosis relies on a combination of clinical assessment, neuroimaging, particularly magnetic resonance imaging (MRI),…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
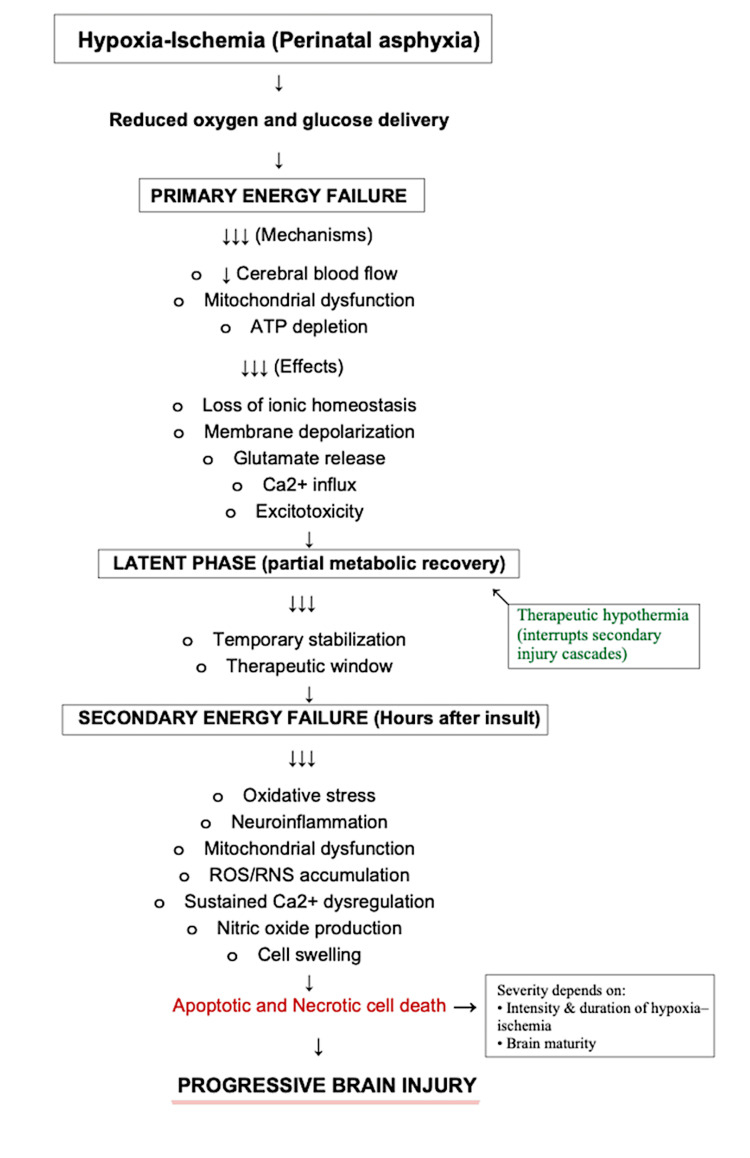 Figure 1
Figure 1| Domain | Stage I (Mild) | Stage II (Moderate) | Stage III (Severe) |
| Consciousness | Hyperalert | Lethargy | Coma/stupor |
| Muscle tone | Normal or mildly increased | Hypotonia or Hypertonia | Flaccid or rigid tone |
| Pupillary response | Mydriasis or dilated pupils with preserved reactivity | Myosis or constricted pupils | Poorly reactive or non-reactive pupils |
| Seizure activity | No seizures or typically absent | Common; often multifocal seizures | May be frequent or difficult to detect due to profound cerebral suppression |
| EEG patterns | Generally normal background activity | Abnormal background with periodic or slow-wave patterns | Severely suppressed activity or near-isoelectric tracing |
| Respiratory patterns | Rapid breathing or hyperventilation | Periodic or irregular respirations | Apnea or dependence on ventilator support |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsNeonatal and fetal brain pathology · Congenital Heart Disease Studies · Blood Coagulation and Thrombosis Mechanisms
Introduction and background
Hypoxic-ischemic encephalopathy (HIE) is a devastating form of neonatal brain injury that results from reduced cerebral blood flow and insufficient oxygen delivery to the brain, most commonly occurring during the perinatal period. It represents one of the most serious complications of neonatal asphyxia and remains a major contributor to neonatal mortality and long-term neurological morbidity worldwide. Survivors of HIE often experience persistent neurodevelopmental impairments, including cerebral palsy, epilepsy, cognitive deficits, and behavioral disorders, which significantly affect quality of life [1].
The pathogenesis of HIE is complex and involves a dynamic sequence of biochemical and molecular events rather than a single acute insult. The initial hypoxic-ischemic event leads to primary energy failure, characterized by impaired oxidative metabolism and depletion of high-energy phosphates. This is followed by a secondary phase of injury that develops hours to days later and is driven by reperfusion injury, excessive glutamate release, oxidative stress, mitochondrial dysfunction, inflammatory responses, and activation of programmed cell death pathways. These interconnected mechanisms ultimately result in progressive neuronal and glial injury [1].
Despite advances in perinatal and neonatal care, therapeutic hypothermia remains the only established standard treatment for neonatal HIE. While hypothermia has been shown to reduce mortality and improve neurodevelopmental outcomes, its neuroprotective effects are limited, and a significant proportion of treated infants continue to develop long-term neurological disabilities [1-3]. This has prompted increasing interest in adjunctive and emerging therapies, including pharmacological agents and regenerative approaches such as stem cell therapy, which aim to target multiple pathways involved in secondary brain injury.
A deeper understanding of the underlying pathophysiological mechanisms of HIE is essential for the development of more effective therapeutic strategies. Ongoing research continues to explore novel neuroprotective interventions that may enhance the efficacy of hypothermia and improve neurological outcomes for affected newborns. This growing body of evidence highlights the need for continued investigation into both the mechanisms and management of HIE.
Review
Methods
A narrative literature review was conducted to summarize current evidence regarding the epidemiology, etiology, pathophysiology, diagnosis, and management of HIE in newborns. An electronic search of the PubMed, Scopus, and Google Scholar databases was performed to identify relevant studies published in English. The search strategy included combinations of the following keywords: "hypoxic-ischemic encephalopathy", "neonatal brain injury", "perinatal asphyxia", "therapeutic hypothermia", and "neuroprotection".
Articles published within the past 10-15 years were prioritized to ensure inclusion of contemporary evidence, although seminal earlier studies were also reviewed when relevant. Eligible publications included review articles, randomized controlled trials, observational studies, and clinical guidelines focusing on neonatal HIE. Studies were excluded if they were not relevant to neonatal populations, lacked clinical relevance, or were duplicate publications.
Titles and abstracts were initially screened for relevance, followed by a full-text review of selected articles. Additional references were identified through manual screening of the bibliographies of relevant articles. The included literature was qualitatively synthesized to provide a comprehensive overview of current understanding and management approaches for HIE in newborns.
Epidemiology and etiopathogenesis of HIE
HIE is a major cause of neonatal morbidity and mortality worldwide, with incidence varying significantly by region. In high-income countries, HIE occurs in approximately 1-2 per 1,000 live births, largely due to advances in prenatal care, intrapartum monitoring, and neonatal resuscitation. However, in low- and middle-income countries, the incidence is substantially higher, ranging from 10 to 20 per 1,000 live births, reflecting disparities in access to obstetric and neonatal care [4].
Despite improvements in perinatal management, HIE continues to be associated with significant long-term neurological sequelae, including cerebral palsy, epilepsy, and cognitive impairment [5]. Although therapeutic hypothermia has improved outcomes in selected cases, its neuroprotective effects remain limited, and a considerable proportion of affected infants develop persistent neurodevelopmental disabilities. These epidemiological trends highlight the global burden of HIE and emphasize the need for effective preventive and therapeutic strategies.
Neonatal HIE primarily results from perinatal asphyxia, a condition characterized by impaired gas exchange leading to insufficient oxygen delivery and reduced cerebral perfusion around the time of birth. The most commonly implicated etiological factors are acute obstetric complications that compromise fetal oxygenation. These include placental abruption, umbilical cord prolapse, and uterine rupture, all of which can abruptly interrupt placental blood flow and precipitate hypoxic-ischemic injury to the neonatal brain.
The severity of brain injury is influenced by both the duration and intensity of hypoxia-ischemia, as well as the newborn’s ability to initiate effective respiration at birth. In severe cases, prolonged oxygen deprivation leads to metabolic acidosis and widespread neuronal dysfunction, contributing to disturbances in consciousness, reflexes, and motor tone. Thus, HIE represents the neurological consequence of a critical failure in oxygen delivery during the perinatal period, most often secondary to identifiable intrapartum events [6,7].
Pathophysiology of HIE
HIE arises from a critical reduction in oxygen and glucose delivery to the neonatal brain, typically secondary to perinatal asphyxia. This deprivation disrupts oxidative metabolism, leading to a cascade of cellular and molecular events that culminate in neuronal injury and death. The pattern of brain injury in HIE is classically described as occurring in two sequential phases of energy failure (Figure 1).
Pathophysiological cascade of HIE.Perinatal asphyxia leads to reduced oxygen and glucose delivery to the neonatal brain, resulting in a primary phase of energy failure characterized by impaired mitochondrial oxidative phosphorylation, adenosine triphosphate depletion, excitotoxic neurotransmitter release, and intracellular calcium influx. Following a brief latent phase of partial metabolic recovery, a delayed secondary energy failure develops, driven by progressive mitochondrial dysfunction, oxidative stress, neuroinflammation, and sustained calcium dysregulation, ultimately culminating in apoptotic and necrotic neuronal cell death. Recognition of this latent phase provides the biological rationale for therapeutic hypothermia to interrupt secondary injury cascades and limit irreversible brain injury.In this schematic, single arrows indicate sequential progression between pathophysiological stages, whereas triple arrows denote a single upstream process leading to multiple downstream mechanisms or effects. Bullet points represent parallel processes occurring within the same pathophysiological phase.HIE: hypoxic-ischemic encephalopathy; ATP: adenosine triphosphate; Ca²⁺: calcium ion; ROS: reactive oxygen species; RNS: reactive nitrogen species.This schematic represents an author-generated synthesis of the pathophysiological cascade of HIE, constructed according to and informed by previously published literature [8,9].
The primary energy failure occurs during the hypoxic-ischemic insult itself. Reduced cerebral blood flow and oxygen availability impair mitochondrial oxidative phosphorylation, resulting in rapid depletion of adenosine triphosphate (ATP). This energy failure causes loss of ionic homeostasis, membrane depolarization, and excessive release of excitatory neurotransmitters, particularly glutamate. Overactivation of glutamate receptors leads to intracellular calcium influx, triggering enzymatic pathways that damage cellular membranes, proteins, and DNA.
Following a brief latent period during which partial metabolic recovery may occur, a secondary energy failure develops hours after the initial insult. This delayed phase is characterized by mitochondrial dysfunction, oxidative stress, and neuroinflammation. Accumulation of reactive oxygen and nitrogen species promotes lipid peroxidation, while sustained calcium dysregulation and nitric oxide production further exacerbate neuronal injury. These processes ultimately result in apoptotic and necrotic cell death, extending the extent of brain damage beyond the initial ischemic event.
The severity and distribution of injury depend on the intensity and duration of hypoxia-ischemia, as well as the maturity of the brain at the time of insult. Clinically, neurological manifestations evolve over the first 72 hours of life, reflecting the progression of these underlying pathophysiological mechanisms. The recognition of this delayed secondary phase provides the rationale for therapeutic hypothermia, which aims to interrupt these injurious cascades during the narrow window of opportunity following birth and thereby limit irreversible brain injury [8,9].
Clinical presentation and severity classification
The clinical presentation of neonatal HIE varies according to the severity and duration of the hypoxic-ischemic insult. Clinical manifestations may be evident immediately after birth or may evolve progressively during the first hours of life.
Mild to moderate manifestations of HIE in newborns commonly include abnormal muscle tone, presenting as hypotonia or hypertonia, feeding difficulties, irritability, fatigue, and a weak or diminished cry. Affected infants may also exhibit altered skin coloration, including pallor or a bluish or gray discoloration of the skin, lips, and extremities, indicative of compromised oxygenation. Neurological findings at this stage are often variable and may fluctuate during the early postnatal period.
Severe HIE is characterized by significant neurological and systemic dysfunction. Clinical features may include episodes of apnea, impaired or absent reflexes, irregular or slowed heart rate (bradycardia), and altered levels of consciousness ranging from stupor to coma. Seizures are frequently observed within the first 24 hours of life and represent a key indicator of ongoing cerebral injury [9]. In the most severe cases, infants may be unable to maintain adequate ventilation or cardiovascular stability without intensive supportive care. The pattern, combination, and progression of these clinical signs are essential for assessing disease severity and guiding further diagnostic evaluation and appropriate management strategies [9-11].
Sarnat staging of neonatal encephalopathy
The severity of HIE is commonly classified using the Sarnat and Sarnat staging system, which categorizes neonatal encephalopathy into three stages based on neurological examination and clinical findings (Table 1) [11]. This assessment involves evaluation of multiple neurological parameters, including mental status, reflexes, muscle tone, autonomic function (including pupillary response and other autonomic indicators), seizure activity, and electroencephalographic (EEG) patterns. This classification system plays a crucial role in guiding treatment decisions, predicting neurological outcomes, and determining eligibility for therapeutic hypothermia.
Stage I (Mild HIE)
Infants with mild HIE are typically hyperalert or irritable and may exhibit an increased startle response. Muscle tone is often normal or mildly increased, and primitive reflexes, such as the Moro and suck reflexes, remain intact. Seizures are uncommon at this stage. Autonomic function is characterized by sympathetic dominance, including findings such as dilated pupils (mydriasis). EEG findings are usually normal. Clinical symptoms generally resolve within 24 hours, and long-term neurological outcomes are generally favorable; however, some infants may still develop subtle neurodevelopmental impairments, particularly affecting cognitive function.
Stage II (Moderate HIE)
Moderate HIE is characterized by lethargy, hypotonia, diminished spontaneous activity, and weakened primitive reflexes. Seizures are common and frequently occur within the first 24 hours of life. Infants may also present with abnormal breathing patterns, feeding difficulties, and autonomic dysfunction characterized by parasympathetic dominance, such as pupillary constriction (miosis). EEG findings are abnormal and often demonstrate low-voltage activity or theta-delta patterns. The duration of this stage typically ranges from 2 to 14 days. Infants with moderate HIE require close neurological monitoring and therapeutic hypothermia when eligible; however, close monitoring is also recommended in mild HIE, as neurological status may evolve during the early postnatal period.
Stage III (Severe HIE)
Severe HIE is associated with profound neurological depression, including severely impaired consciousness, flaccid muscle tone, absent reflexes, and minimal spontaneous movement. Seizures may be frequent and refractory. EEG findings are markedly abnormal, often showing severely suppressed or isoelectric patterns. Infants with severe HIE commonly require intensive supportive care, and the prognosis is poor, with a high risk of mortality or severe long-term neurological disability [11,12].
Other associated complications of HIE
HIE is associated with a broad range of long-term neurological complications that may persist beyond the neonatal period. The extent of chronic neurological impairment is largely determined by the severity and duration of the initial hypoxic-ischemic insult. Survivors may experience outcomes ranging from subtle cognitive deficits to profound motor and cognitive disabilities that significantly limit independence. Long-term sequelae commonly reported include epilepsy, movement disorders, myoclonus, cognitive dysfunction, and disorders of consciousness. In severe cases, persistent vegetative states or severe global neurological impairment may occur. Early prediction of long-term neurological outcomes remains challenging, highlighting the need for prolonged follow-up and comprehensive neurodevelopmental assessment in affected infants [13].
Multiple maternal, intrapartum, and neonatal factors have been associated with the development and severity of HIE, as well as with subsequent neurological outcomes. Maternal factors such as advanced maternal age, underlying medical conditions, medication use during pregnancy, and adverse socioeconomic conditions have been implicated in increasing vulnerability to perinatal hypoxia. Intrapartum complications, including pregnancy-related hypertensive disorders and reduced amniotic fluid volume, further contribute to the risk of hypoxic-ischemic injury. Postnatally, the need for extensive resuscitation at birth and evidence of metabolic acidosis are frequently associated with more severe disease. Neuroimaging patterns, particularly involvement of deep gray matter structures or watershed regions, have also been linked to outcome variability. These findings underscore the complex interplay between antenatal, peripartum, and neonatal factors in influencing both the occurrence of HIE and its clinical trajectory, highlighting the importance of early identification of high-risk infants to guide timely intervention and long-term follow-up [14].
Diagnostic evaluation
The diagnosis of HIE is based on a combination of perinatal history, clinical findings, neurological examination, and laboratory and imaging studies. Early and accurate diagnosis is essential, as timely intervention, particularly therapeutic hypothermia, can significantly improve neurological outcomes [15,16].
A detailed perinatal history is the first step in evaluation and includes evidence of fetal distress, perinatal asphyxia, and low Apgar scores assessed at 5 and 10 minutes after birth. Apgar scoring evaluates appearance, pulse, grimace, activity, and respiration and provides an early indication of neonatal compromise. These findings support early risk stratification but are not diagnostic on their own.
Neurological examination remains central to the diagnostic process. Assessment includes level of consciousness, muscle tone, spontaneous activity, primitive reflexes, respiratory effort, and the presence of seizures. These clinical features assist in determining disease severity and help classify infants according to established staging systems such as the Sarnat classification.
Laboratory investigations support the diagnosis by identifying metabolic and systemic abnormalities associated with hypoxic injury. Arterial blood gas analysis may demonstrate severe metabolic acidosis, commonly defined by a pH less than 7.0 or a base deficit equal to or greater than 12 mmol/L. Elevated lactate levels and evidence of multiorgan dysfunction further reflect the severity of hypoxic-ischemic insult.
EEG and amplitude-integrated electroencephalography (aEEG) play a critical role in diagnostic evaluation by detecting both clinical and subclinical seizure activity and by assessing background cerebral function. Abnormal EEG or aEEG patterns, including low-voltage activity, discontinuous backgrounds, or burst suppression, are associated with more severe brain injury and poorer neurodevelopmental outcomes. Continuous neurophysiological monitoring is particularly valuable in infants undergoing therapeutic hypothermia.
Neuroimaging is an essential component of diagnostic assessment. Cranial ultrasound may be used as an initial bedside tool; however, magnetic resonance imaging (MRI) provides superior sensitivity for defining the extent and pattern of brain injury. Diffusion-weighted imaging is especially useful in identifying early ischemic changes and in determining injury severity. Specific patterns, such as involvement of deep gray matter structures or watershed regions, have been associated with outcome variability.
In addition to neurological findings, systemic involvement should be assessed as part of the diagnostic workup. Evidence of renal or metabolic dysfunction has been associated with more severe disease and poorer prognosis, highlighting the importance of comprehensive multi-system evaluation.
Overall, the integration of clinical assessment, laboratory findings, neurophysiological monitoring, and neuroimaging provides a comprehensive diagnostic approach that guides management decisions and assists in predicting long-term neurological outcomes in infants with HIE.
Management strategies
Management of HIE focuses on early stabilization, neuroprotection, seizure control, and prevention of secondary brain injury. Prompt identification of eligible infants and timely initiation of therapeutic hypothermia remain the cornerstone of treatment for moderate to severe HIE [17].
Initial management includes optimization of airway, breathing, and circulation to ensure adequate oxygenation and cerebral perfusion. Careful control of blood glucose, electrolytes, blood pressure, and acid-base balance is essential to minimize secondary metabolic injury. Seizures should be promptly identified and treated, as ongoing seizure activity is associated with worse neurological outcomes.
Therapeutic hypothermia is currently the only evidence-based neuroprotective therapy shown to improve outcomes in neonates with moderate to severe HIE. Standard protocols aim to achieve a target core temperature of approximately 33.5°C for a duration of 72 hours, followed by gradual rewarming. This intervention has been shown to reduce mortality and long-term neurodevelopmental disability when initiated within the first six hours of life.
Recent evidence suggests that impaired thermoregulation in neonates with HIE may provide additional prognostic information during therapeutic hypothermia. Infants with more severe hypoxic-ischemic injury often exhibit spontaneous hypothermia and therefore require less active cooling to maintain the target temperature. Studies have demonstrated that neonates with unfavorable short-term outcomes required lower cooling device output to sustain core temperatures between 33 and 34°C compared to those with more favorable outcomes. This reduced need for active cooling has been strongly associated with higher MRI injury scores and increased mortality.
Cooling device output temperature has therefore emerged as a potential early physiological biomarker of injury severity during therapeutic hypothermia. Greater impairment in temperature regulation reflects more extensive cerebral injury and may aid in early risk stratification. This association underscores the importance of continuous temperature monitoring and careful adjustment of cooling parameters throughout treatment.
Neuroimaging, particularly MRI with diffusion-weighted sequences performed during the first week of life, plays a crucial role in guiding prognosis and ongoing management. A higher injury burden on MRI correlates with poorer outcomes and may influence decisions regarding escalation of supportive care and long-term follow-up planning.
Management of HIE extends beyond the acute phase and requires a multidisciplinary approach. Infants with moderate to severe disease should undergo long-term neurodevelopmental surveillance to detect cognitive, motor, and behavioral impairments early. Ongoing research into adjunctive neuroprotective therapies aims to enhance the benefits of therapeutic hypothermia and improve outcomes across all severity grades, including mild HIE.
Supportive care in the neonatal intensive care unit (NICU) is a fundamental component of management for infants with HIE. Many affected neonates require respiratory support due to impaired respiratory drive, apnea, or inadequate gas exchange. Supplemental oxygen or mechanical ventilation may be necessary to maintain appropriate oxygenation and carbon dioxide levels, thereby preventing secondary hypoxic injury [18].
Hemodynamic stability is carefully maintained through continuous monitoring of heart rate and blood pressure, judicious fluid administration, and the use of inotropic agents when indicated. Maintaining adequate cerebral perfusion is essential to limit ongoing neuronal damage. Seizure management is a critical aspect of supportive care, as seizures are common in neonates with HIE and are associated with worse neurological outcomes. Anticonvulsant therapy is initiated promptly, with agents such as phenobarbital or levetiracetam commonly used to control both clinical and electrographic seizures.
Ongoing monitoring of vital signs, oxygen saturation, and core temperature is essential throughout treatment to ensure physiologic stability and to minimize secondary brain injury.
Moreover, broader healthcare system factors may influence the management and evaluation of HIE, as highlighted during the COVID-19 pandemic. Disruptions in prenatal and perinatal care, changes in obstetric practices, and increased maternal comorbidities were associated with a rise in NICU admissions for HIE evaluation during this period. Despite the increased number of infants screened for suspected HIE, the proportion of neonates ultimately diagnosed with HIE or treated with therapeutic hypothermia remained comparable to pre-pandemic levels. These observations emphasize the importance of maintaining standardized screening protocols, timely neurological assessment, and access to therapeutic hypothermia, even during periods of healthcare system strain. Ensuring continuity of neonatal neurocritical care pathways is essential to prevent delays in diagnosis and to preserve outcomes for infants at risk of hypoxic-ischemic brain injury [19].
Additionally, *nutritional support *plays an important role in the overall management of neonates with HIE [20,21]. In the acute phase, enteral feeding is often delayed due to hemodynamic instability or impaired gastrointestinal function. However, emerging evidence suggests that minimal enteral nutrition (trophic feeding) during therapeutic hypothermia is safe and beneficial in clinically stable neonates [22]. During this period, nutritional requirements are met through intravenous fluids to maintain hydration and provide essential glucose and electrolytes.
Enteral feeding via tube feeding is initiated once the infant is clinically stable and oral feeding is considered unsafe. The transition to oral feeding is guided by neurological status and swallowing function. Careful metabolic management is essential to reduce additional neurological stress. Hypoglycemia, electrolyte imbalances, and metabolic acidosis are promptly corrected, as these disturbances can exacerbate neuronal injury.
Continuous monitoring and maintenance of adequate oxygen saturation, hemodynamic stability, glycemic control, and normothermia are essential to minimizing secondary brain injury and promoting recovery during both the acute and subacute phases of care. In parallel, several adjunctive neuroprotective strategies are under investigation, including erythropoietin (EPO), xenon gas, and stem cell-based therapies. Although these approaches show promise, their use remains experimental. Early involvement of a multidisciplinary team, encompassing neonatologists, neurologists, and developmental specialists, is strongly recommended to optimize ongoing management and long-term follow-up [23-25].
As affected children grow, some complications may emerge, necessitating additional supportive interventions. These may include physical or occupational therapy, speech and language therapy, and the use of assistive devices such as corrective lenses or hearing aids, which can be implemented to support functional development. Overall, the integration of therapeutic hypothermia with comprehensive supportive care continues to represent the cornerstone of HIE management, with the overarching aim of improving long-term neurological outcomes and quality of life for affected infants.
Prognosis and long-term outcomes
Long-term outcomes following HIE remain a major source of morbidity despite advances in neonatal care. Survivors may experience persistent impairments across multiple neurodevelopmental domains, including motor function, cognition, behavior, and language. Cerebral palsy, epilepsy, learning difficulties, and executive dysfunction are among the most commonly reported sequelae, with risk increasing in parallel with the severity of the initial encephalopathic insult. Although therapeutic hypothermia has significantly improved survival and neurodevelopmental outcomes in term and late-preterm infants with moderate to severe HIE, a substantial proportion of affected infants continue to demonstrate long-term disabilities. Moreover, current evidence does not support a clear long-term benefit of adjunctive neuroprotective therapies when combined with hypothermia, and their role remains under investigation. Ongoing longitudinal follow-up and standardized neurodevelopmental assessment are therefore essential to accurately characterize outcomes, guide early intervention strategies, and optimize quality of life for children affected by HIE [26,27].
Furthermore, evidence from landmark randomized controlled trials, including the NICHD, TOBY, and CoolCap studies, has been central to defining long-term outcomes and establishing therapeutic hypothermia as the standard of care for term infants with HIE. These trials introduced strict inclusion criteria and standardized treatment protocols, representing a major methodological advancement compared with earlier pre-cooling era studies.
In the pivotal NICHD Neonatal Research Network trial, 102 infants were randomized to whole-body hypothermia and 106 to standard supportive care. The composite outcome of death or moderate to severe disability occurred in 44% of infants treated with hypothermia compared with 62% in the control group (p = 0.01). Mortality was lower in the hypothermia group (24%) than in controls (37%), although this difference did not reach statistical significance (p = 0.08). Neurodevelopmental assessment at 18-22 months demonstrated no significant differences between groups in rates of cerebral palsy, blindness, or hearing impairment requiring aids.
Long-term follow-up of the same cohort at 6-7 years of age confirmed sustained survival benefits associated with hypothermia. Death occurred in 28% of children in the hypothermia group compared with 44% in the control group (p = 0.04), while the combined outcome of death or severe disability was observed in 41% versus 60%, respectively (p = 0.03). Although rates of moderate to severe disability, attention-deficit/hyperactivity disorder, and visuospatial dysfunction among survivors were similar between groups, hypothermia significantly reduced mortality and the risk of the combined endpoint of death or an IQ score below 70 [28].
Emerging evidence suggests that biological sex may significantly influence injury mechanisms and recovery trajectories following HIE. Preclinical studies demonstrate sex-specific differences in inflammatory responses and neuronal vulnerability, indicating that males and females may respond differently to both hypoxic injury and neuroprotective interventions. Consequently, future therapeutic strategies should incorporate sex as a critical biological variable to optimize treatment efficacy. Additionally, neonatal responses to neuroprotective agents cannot be directly extrapolated from adult models, as developmental differences in brain maturation, receptor expression, and hepatic and renal drug metabolism substantially affect treatment response and clearance. Recognizing these distinctions is essential for refining targeted therapies and improving long-term outcomes in neonates with HIE [28-31].
Collectively, findings from these trials and subsequent meta-analyses demonstrate that therapeutic hypothermia confers durable survival benefits and reduces the risk of death and severe neurodevelopmental impairment, thereby substantially improving long-term prognosis in infants with moderate to severe HIE.
Discussion
Based on the pathophysiological mechanisms and clinical stages of HIE described in this review, it is evident that HIE represents a progressive and multifaceted disease process rather than a single static injury. The initial hypoxic-ischemic insult triggers a cascade of cellular and molecular events, including energy failure, excitotoxicity, oxidative stress, inflammation, and apoptosis, which evolve across distinct phases and ultimately shape clinical presentation and long-term outcomes. The severity of these processes is reflected in the clinical spectrum of mild, moderate, and severe encephalopathy, emphasizing the close relationship between underlying pathophysiology and neurological staging.
Understanding this relationship has direct implications for diagnosis and management. Early clinical staging provides an initial framework for severity assessment; however, the overlap between stages and the presence of abnormal neurophysiological and imaging findings even in mild cases highlight the limitations of clinical examination alone. Integration of EEG monitoring and advanced neuroimaging allows for more accurate characterization of injury extent and timing, supporting earlier risk stratification and more informed therapeutic decision-making [11,12].
Therapeutic hypothermia targets several key components of the secondary injury phase by reducing metabolic demand, attenuating excitotoxicity, and limiting inflammatory responses. Evidence from randomized clinical trials demonstrates that this intervention improves survival and reduces severe neurodevelopmental disability in infants with moderate to severe HIE. Nevertheless, persistent neurological impairment among survivors indicates that hypothermia does not fully address all mechanisms of injury, particularly those associated with delayed neuronal loss and impaired neural repair [2,3,17].
Supportive care remains essential throughout all stages of HIE, as maintenance of physiological stability directly influences the progression of secondary injury. Careful regulation of oxygenation, hemodynamics, glucose levels, temperature, and nutrition plays a critical role in mitigating further neuronal damage and supporting recovery. Long-term outcomes are further influenced by early access to multidisciplinary follow-up and rehabilitative services, which address emerging motor, cognitive, and sensory deficits [18,19].
Future directions in HIE management must therefore build upon an integrated understanding of pathophysiology and clinical staging. Emerging neuroprotective and regenerative therapies aim to extend the therapeutic window beyond the acute phase and to promote endogenous repair mechanisms that are not fully addressed by hypothermia alone. Advances in biomarker development, individualized risk assessment, and combination treatment strategies may enable more precise targeting of therapies according to disease stage and injury profile. Continued translational research and long-term outcome studies are essential to refine prevention strategies and reduce the lifelong neurological burden associated with HIE [26-31].
Prevention and future directions of HIE
Prevention of HIE focuses on early identification of perinatal risk factors, optimization of obstetric and intrapartum care, and prompt postnatal interventions aimed at limiting secondary neuronal injury. Although therapeutic hypothermia remains the established standard of care, its effectiveness is constrained by a narrow therapeutic window that requires initiation within the first six hours of life. This limitation underscores the need for adjunctive strategies capable of extending neuroprotection beyond the acute phase of injury. Growing evidence indicates that cell-based therapies, particularly the administration of autologous umbilical cord blood stem cells, may provide an expanded therapeutic window by reducing apoptosis, oxidative stress, and excitotoxic injury while simultaneously promoting endogenous repair mechanisms. Experimental models and early clinical studies suggest that these approaches may enhance neuronal survival and facilitate regenerative processes that are not fully addressed by hypothermia alone. Consequently, future directions in the management of HIE are increasingly focused on combination therapies that integrate therapeutic hypothermia with regenerative and neuroprotective interventions. This shift is accompanied by efforts to develop standardized treatment protocols, reliable biomarkers for patient selection, and structured long-term outcome monitoring. Ongoing translational research and well-designed clinical trials are essential to determine the safety, efficacy, and optimal timing of these emerging therapies, with the overarching goal of reducing long-term neurological disability in affected infants [32].
Conclusions
HIE remains a major cause of neonatal mortality and long-term neurological morbidity despite advances in perinatal care. Outcomes depend on injury mechanisms, clinical severity, and the timing of diagnosis and intervention. Therapeutic hypothermia improves survival but does not eliminate long-term neurological impairment. Comprehensive supportive care and structured follow-up, therefore, remain essential. Future progress will rely on earlier risk identification, improved biomarkers, and adjunctive neuroprotective strategies alongside hypothermia protocols. Continued multidisciplinary collaboration and long-term monitoring are necessary to reduce the lifelong burden of HIE and improve the quality of life for affected infants and their families.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Correction to: hypoxic-ischemic encephalopathy: pathogenesis and promising therapies Mol Neurobiol Yang M Wang K Liu B Shen Y Liu G 21236220253919649610.1007/s 12035-024-04441-9 · doi ↗ · pubmed ↗
- 2Hypoxic-ischemic encephalopathy: changing outcomes across the spectrum Clin Perinatol Pappas A Milano G Chalak LF 31525020233686871210.1016/j.clp.2022.11.007 · doi ↗ · pubmed ↗
- 3State of the science: hypoxic ischemic encephalopathy and hypothermic intervention for neonates Adv Neonatal Care Selway LD 60661020102038636910.1097/ANC.0b 013e 3181 d 54b 30 · doi ↗ · pubmed ↗
- 4Pathophysiology of hypoxic-ischemic encephalopathy: a review of the past and a view on the future Acta Neurol Belg Greco P Nencini G Piva I 27728812020203211234910.1007/s 13760-020-01308-3 · doi ↗ · pubmed ↗
- 5Development of epilepsy in newborns with moderate hypoxic-ischemic encephalopathy and neonatal seizures Brain Dev Pisani F Orsini M Braibanti S Copioli C Sisti L Turco EC 64683120091849012510.1016/j.braindev.2008.04.001 · doi ↗ · pubmed ↗
- 6Neonatal hypoxic-ischemic encephalopathy (Article in Spanish)Medicina (B Aires) Papazian O 364178 Suppl 22018 https://pubmed.ncbi.nlm.nih.gov/30199363/30199363 · pubmed ↗
- 7Pathophysiology of perinatal asphyxia in humans and animal models Biomedicines Mota-Rojas D Villanueva-García D Solimano A Muns R Ibarra-Ríos D Mota-Reyes A 10202210.3390/biomedicines 10020347 PMC 896179235203556 · doi ↗ · pubmed ↗
- 8The chilling details: hypoxic-ischemic encephalopathy J Perinat Neonatal Nurs Verklan MT 59702320091920906110.1097/01.JPN.0000346221.48202.7e · doi ↗ · pubmed ↗