Primary Arthroscopic Repair of the Anterior Cruciate Ligament with Femoral Fixation Using an Adjustable EndoButton and Dynamic Reinforcement with High-Strength Suture
Antonio Carlos Moscon, Fabrício Luz Cardoso, Daniel Rocha de Almeida Braga, Claudio Gattás

TL;DR
This paper presents a new arthroscopic technique for repairing ACL tears using adjustable fixation and suture reinforcement, aiming to preserve anatomy and reduce recovery risks.
Contribution
A novel ACL repair method combining adjustable EndoButton fixation with dynamic suture reinforcement is introduced for acute proximal ruptures.
Findings
The technique preserves ligament anatomy and proprioception while avoiding graft harvesting.
Early mobilization and structured rehabilitation are emphasized in the postoperative protocol.
The method is suitable for selected patients like young athletes and skeletally immature individuals.
Abstract
Primary anterior cruciate ligament (ACL) repair has reemerged as an alternative in selected cases thanks to advances in arthroscopic techniques and the development of modern fixation devices. The present paper describes the arthroscopic ACL repair technique with femoral fixation using an adjustable EndoButton (Smith & Nephew) combined with dynamic reinforcement using a high-strength suture. This technique is primarily indicated for acute proximal ruptures (Sherman et al. types I and II), which present a good ligament remnant and healing potential. The procedure aims to preserve the original anatomy and proprioception, reduce the morbidity associated with graft harvesting, and maintain future reconstruction options. The technique involves suturing the ligament stump, using adjustable femoral fixation, and applying internal bracing to provide additional biomechanical stability. The…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
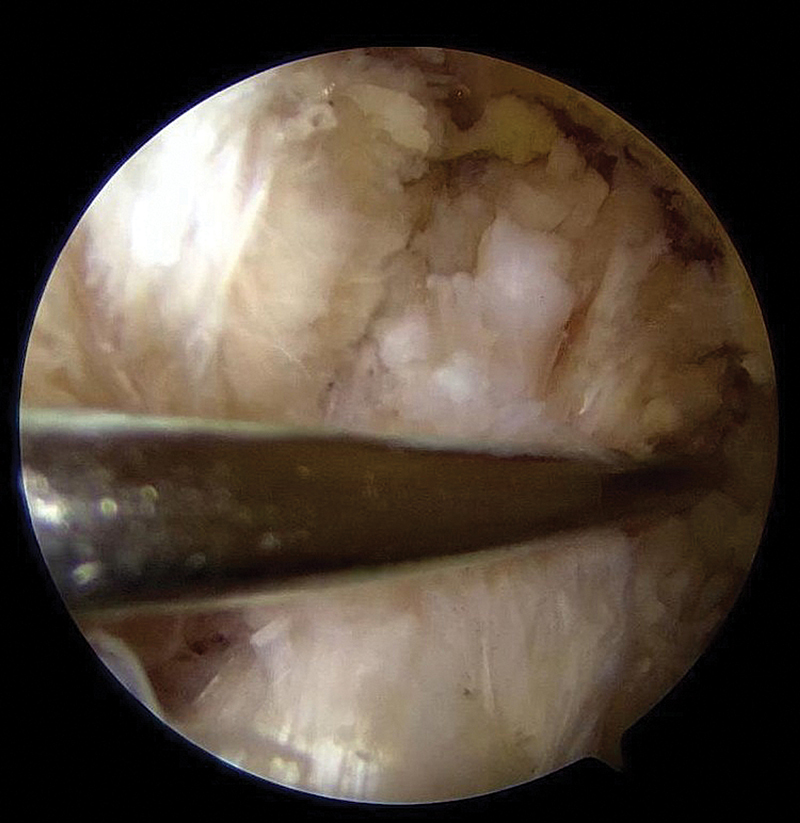 Fig. 1
Fig. 1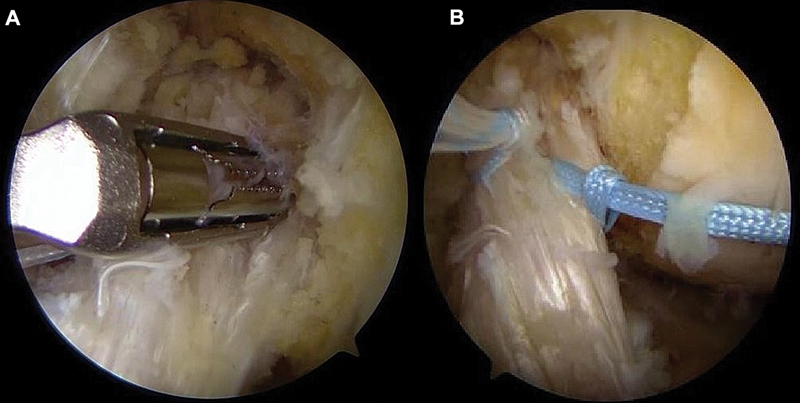 Fig. 2
Fig. 2 Fig. 3
Fig. 3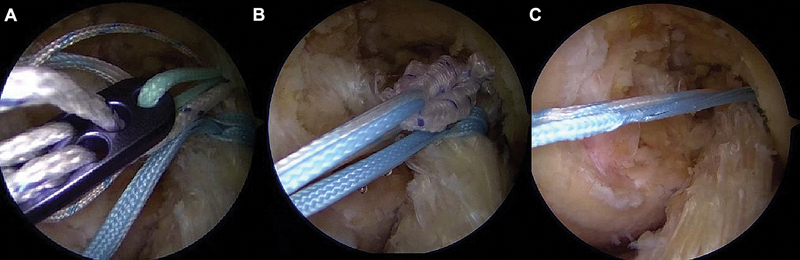 Fig. 4
Fig. 4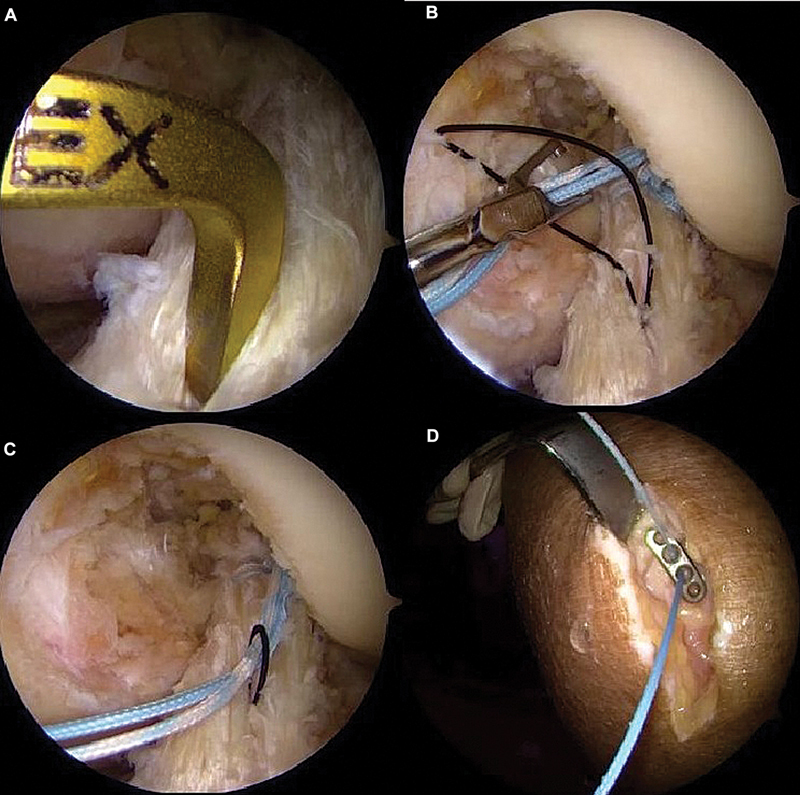 Fig. 5
Fig. 5Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsKnee injuries and reconstruction techniques · Total Knee Arthroplasty Outcomes · Lower Extremity Biomechanics and Pathologies
Introduction
Over the past two decades, advances in arthroscopic techniques and clinical evidence of reliable anterior cruciate ligament (ACL) healing in selected cases, with return-to-sport rates comparable to those of ACL reconstruction (ACLR), sparked an interest in the primary repair of this ligament. 1 2 3
The rationale for primary ACL repair relies on the potential benefits of preserving proprioception, maintaining the original ligament anatomy, and minimizing bone damage with the creation of smaller or fewer tunnels. This strategy also aims to eliminate complications associated with the harvesting of autologous grafts, such as anterior knee pain, hamstring or quadriceps weakness, cramps, and the risk of rupture of the remaining tendons. 2 4
Technological improvements, with the emergence of high-strength sutures and adjustable suspension systems, have enabled the combination of anatomical repair with internal reinforcement techniques (augmentation). This combination aims to promote biological healing, enhance biomechanical safety, and contribute to an expectation of earlier functional recovery, with increased range of motion and a more natural subjective knee sensation. 5 6
The Sherman et al. 7 classification, which identifies which proximal ACL injuries are more prone to healing, was a fundamental milestone in ACLR research.
Recent studies 1 6 report rerupture rates ranging from 7 to 20% in proximal lesions (Sherman et al. 7 types 1 and 2). Currently, these injuries are the most investigated. Although these data support primary repair as a viable alternative in specific scenarios, long-term follow-up studies are still required for a definitive validation of the technique.
The current article provides a detailed description of the arthroscopic technique for primary ACLR with femoral fixation using an adjustable EndoButton (Smith & Nephew) and dynamic reinforcement with high-strength suture. Documentation and refinement of procedural details used a fresh-frozen cadaver model to facilitate the step-by-step demonstration. The study presents the proposed postoperative care and discusses the biomechanical rationale behind this technique, highlighting its theoretical advantages over conventional methods employing external implants.
Patient selection
The success of ACLR depends on meticulous patient selection. The initial evaluation must include detailed medical history, complete physical examination, and analysis of imaging scans.
Patients with ACL rupture frequently report a sharp popping sound at the time of the injury, followed by hemarthrosis and subjective knee instability resulting from anterior tibial translation unresisted by the ruptured ligament. 8
Whenever possible, the physical examination must assess ligamentous laxity using the Lachman and pivot shift tests, which have high specificity to detect anterior tibial and rotational instability. Plain radiographs can help identify associated fractures, such as Segond's fracture, while magnetic resonance imaging (MRI) is essential to confirm the diagnosis, assess the remaining ligament, and detect concomitant injuries.
The ideal indications include acute proximal ruptures, particularly Sherman et al. 7 type-I femoral avulsions, with a good ligament remnant and a short interval between injury and repair, factors that favor greater healing potential and satisfactory clinical outcomes. 6 8 9 Pediatric or skeletally-immature patients also benefit from ACL biological preservation, provided that the integrity of the ligament stump is preserved. 9
In contrast, chronic injuries, ruptures in the mid-substance or distal third of the ligament, degenerated tissue, and recurrences in previously-repaired ligaments represent contraindications, as they compromise the biomechanical quality of the repair and increase the risk of failure. 9
Even in cases of suspected proximal rupture on imaging, the definitive decision between primary repair and reconstruction is made intraoperatively, after direct assessment of the type of rupture and the tissue quality. Moreover, a previous discussion of graft alternatives must occur if reconstruction is required.
Among special populations, such as young athletes in pivoting sports and adults with high physical demands, primary repair may be a viable alternative in selected situations. However, the literature 10 recommends careful evaluation, prudent indication, and structured rehabilitation, given the increased risk of rerupture in these groups.
Description of the technique
Positioning
The patient is in supine position, under general or spinal anesthesia, with a pneumatic tourniquet on the proximal third of the thigh. The limb for treatment is placed on a lateral support for full flexion and extension. Antibiotic prophylaxis is administered according to the institutional protocol.
Arthroscopic portals and inspection
The portals include an anterolateral (optical), an anteromedial (working), and an additional anteromedial portal to construct the femoral tunnel. The joint undergoes inspection and treatment of any associated meniscal or chondral lesions.
ACL identification and stump preparation
The proximal ACL tear is identified, preserving as much of the remaining ligament as possible ( Fig. 1 ). Debridement is minimal, using a shaver or radiofrequency only to remove unstable fibers, preserving vascularization. The femoral footprint is subtly roughened with a shaver or curette to promote healing.
Identification of the proximal anterior cruciate ligament (ACL) injury.
Stump suture
Using an arthroscopic suture passer, 2 sutures are performed with high-strength (no. 2) 100% polyethylene threads in a lasso-loop or locked configuration, from distal to proximal, involving the anteromedial and posterolateral bundles ( Fig. 2 ). The sutures remain free for subsequent tensioning.
Positioning of the arthroscopic suture passer ( A ). Performance of two high-strength sutures involving the anteromedial and posterolateral bundles ( B ).
Femoral fixation
With a femoral guide wire and a 4.5-mm drill bit, a tunnel is created in the anatomical footprint of the ACL through the anteromedial accessory portal, with the knee under hyperflexion ( Fig. 3 ). The ligament stump sutures are passed through the adjustable loop of the EndoButton, guided through the tunnel, and fixed in cortical suspension. The ligament stump is reduced to its footprint by pulling the sutures passed “astride” through the adjustable loop ( Fig. 4 ).
Construction of the femoral tunnel in the anatomical ACL footprint via the anteromedial accessory portal using a 4.5-mm drill bit.
Passing the suture threads through the adjustable loop of the EndoButton ( A ). Guiding the ACL stump through the femoral tunnel ( B ). Suspension fixation of the repaired ACL to the medial wall of the lateral femoral condyle ( C ).
Reinforcement (internal brace)
The same sutures used to close the umbilical stump act as internal reinforcement, providing additional support during ligament healing ( Fig. 4 ).
Tibial fixation and final adjustment
Video 1 Step-by-step of the primary ACL suture technique.
The wires are guided through a 4.5-mm tibial tunnel to the anteromedial band insertion point and secured to the anterior tibial cortex with an EndoButton or knotless anchor ( Fig. 5 ). Knee flexion in 0 to 20° enables the proper tensioning of the adjustable loop.
Positioning of the tibial tunnel ( A ). Passing the wires through the distal ACL ( B ). Guiding the internal brace wires into the tibial tunnel ( C ). Fixation to the anterior tibial cortex with EndoButton ( D ).
A follow-up arthroscopy verifies isometry, absence of impingement, and stability after the repair. Next, three to four microfractures are performed on the medial aspect of the lateral femoral condyle, adjacent to the footprint, to promote biological (bone marrow) stimulation. 11 Drilling into the subchondral bone releases mesenchymal stem cells and bone-marrow growth factors at the repair site, which, by analogy to studies 11 using bone marrow aspirate concentrates (BMACs) in ligament reconstructions, seeks to accelerate and optimize the healing and maturation of the repaired ligament tissue. Video 1 shows the entire procedure, demonstrating the technique step by step.
Closure
After thorough irrigation, the portals are closed with simple nylon sutures, followed by the application of a compression dressing.
Postoperative care
The postoperative protocol involves early mobilization, progressive weight bearing as tolerated, and the initial use of an articulated orthosis. The goal is to stimulate biological healing without compromising joint stability.
Conclusion
This technique combines the principles of primary anatomical ACLR with the use of modern suspension devices, incorporating internal reinforcement through ligament stump sutures passed “astride” the EndoButton loop.
This configuration provides dynamic fixation, promoting continuous approximation of the ligament stump to the femoral footprint even in the presence of slight tibial anteriorization. The choice of an adjustable EndoButton, instead of “fixed” fixations, enables the ideal tensioning and in-situ adjustment of the repair after cortical fixation. This continuous adjustment capability is fundamental for a dynamically-reinforced repair, as it confers a biomechanical advantage to the system, preventing tension loss that can occur during joint movement cycles and favoring constant coaptation of the stump to the biological bed.
This technique is an alternative with key theoretical and biomechanical potential, as it spares native tissue and maintains the possibility of future surgical revisions with lower procedural complexity.
Although the current paper is a “technical note”, limited to a detailed description of the procedure, we used this technique in 15 patients during our initial experience. However, there are not enough results for analysis. The clinical validation of its benefits requires proper follow-up. As such, we plan to prospectively follow up the patients for 6 months to 2 years, through clinical and functional reassessments, using validated knee scores (such as that of the International Knee Documentation Committee) and MRI evaluations at 3, 6, and 12 months postoperatively, aiming to consolidate the results and compare the efficacy with that of the gold standard.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Hoogeslag R AG Veld R HI Brouwer R W De Graaff F Verdonschot N Acute Anterior Cruciate Ligament Rupture: Repair or Reconstruction? Five-Year Results of a Randomized Controlled Clinical Trial Am J Sports Med 202250071779178710.1177/0363546522109052735486517 · doi ↗ · pubmed ↗
- 2Glasbrenner J Raschke M J Kittl C Comparable Instrumented Knee Joint Laxity and Patient-Reported Outcomes After ACL Repair With Dynamic Intraligamentary Stabilization or ACL Reconstruction: 5-Year Results of a Randomized Controlled Trial Am J Sports Med 202250123256326410.1177/0363546522111777736005281 PMC 9527444 · doi ↗ · pubmed ↗
- 3Pang L Li P Li T Li Y Zhu J Tang X Arthroscopic Anterior Cruciate Ligament Repair Versus Autograft Anterior Cruciate Ligament Reconstruction: A Meta-Analysis of Comparative Studies Front Surg 2022988752210.3389/fsurg.2022.88752235521430 PMC 9066561 · doi ↗ · pubmed ↗
- 4Vermeijden H D Van der List J P Benner J L Rademakers M V Kerkhoffs G MMJ Di Felice G S Primary repair with suture augmentation for proximal anterior cruciate ligament tears: A systematic review with meta-analysis Knee 202238192910.1016/j.knee.2022.07.00135870397 · doi ↗ · pubmed ↗
- 5Huntington L S Tulloch S Suture Tape Augmentation of Anterior Cruciate Ligament Reconstruction Increases Biomechanical Stability: A Scoping Review of Biomechanical, Animal, and Clinical Studies Arthroscopy 202238062073208910.1016/j.arthro.2021.12.03634990759 · doi ↗ · pubmed ↗
- 6Robinson J D Jr Williamson T Carson T Whelan R J Abelow S P Gilmer B B Primary anterior cruciate ligament repair: Current concepts J ISAKOS 202380645646610.1016/j.jisako.2023.08.00837633336 · doi ↗ · pubmed ↗
- 7Sherman M F Lieber L Bonamo J R Podesta L Reiter I The long-term followup of primary anterior cruciate ligament repair. Defining a rationale for augmentation Am J Sports Med 1991190324325510.1177/0363546591019003071867333 · doi ↗ · pubmed ↗
- 8Morrow D L Hughes A G Murray R D Bruce J R Arthroscopic Primary Repair of Proximally Based Anterior Cruciate Ligament Tear With Augmentation and All-Epiphyseal Fixation Arthrosc Tech 2024130910304010.1016/j.eats.2024.10304039308583 PMC 11411292 · doi ↗ · pubmed ↗