Freeze-Dried Mother's Own Milk for Novel Fortification in a Late Preterm Infant with Complicated Intestinal Atresia and Congenital Shortened Bowel: A Case Report
Allyson Ward, Sarah M. Reyes, Berkley Luck, Laura Serke, Lauren Figard, Amy Kimball

TL;DR
A late preterm infant with intestinal issues successfully gained weight using freeze-dried mother's own milk as a fortification strategy after hospital discharge.
Contribution
Introduces freeze-dried mother's own milk as a novel fortification method for medically complex infants with feeding intolerance.
Findings
The infant transitioned from the 24th to the 66th percentile for weight-for-age within 86 days using freeze-dried mother's own milk.
Symptoms like fussiness and abdominal distention resolved within 24 hours after switching to freeze-dried mother's own milk fortification.
Freeze-dried mother's own milk allowed exclusive mother's milk feeding while supporting growth post-discharge.
Abstract
Feeding intolerance and growth failure commonly complicate recovery in infants with complicated intestinal atresia, often requiring prolonged human milk fortification after hospital discharge. Our objective was to describe a novel fortification strategy that enabled an exclusive mother's own milk (MOM) diet during postdischarge fortification in a medically complex infant with feeding intolerance. This case report details the use of freeze-dried mother's own milk (FDMOM) to fortify expressed MOM in a late preterm infant with complicated atresia and congenital shortened bowel to resolve feeding intolerance and weight faltering. Freeze-drying of MOM took place at a commercial facility using SafeDry, a patented contact-free process. FDMOM was used to increase the caloric density of expressed MOM under medical supervision using a targeted fortification approach. The patient tolerated…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
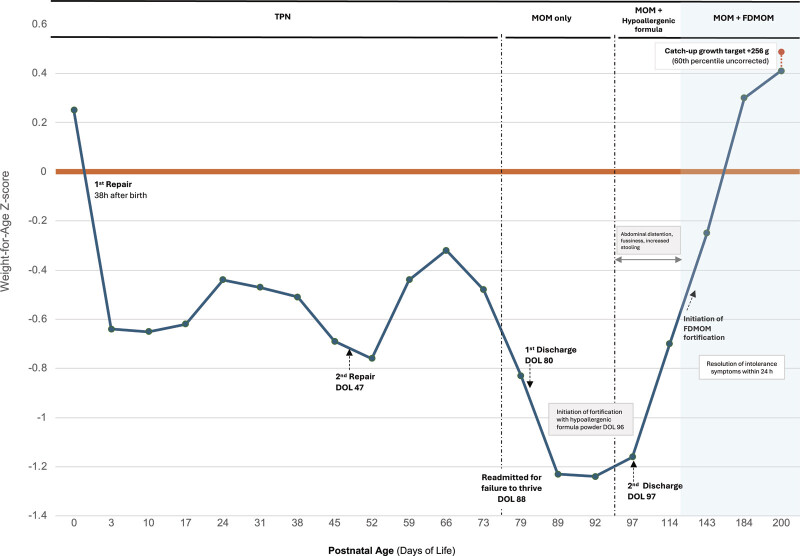 Fig. 1
Fig. 1| Sample | True protein (g/L) | Carbohydrate (g/L) | Fat (g/L) | Energy (kcal/100 mL) |
|---|---|---|---|---|
|
Baseline MOM
| 7.0 | 80.9 | 29.3 | 63.2 |
|
FDMOM-fortified MOM (+6 kcal/oz)
| 7.3 | 84.3 | 30.2 | 83.5 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsInfant Nutrition and Health · Infant Health and Development · Child Nutrition and Feeding Issues
Introduction
Feeding intolerance and impaired growth are common and clinically challenging sequelae in infants with complicated intestinal atresia. 1 These complications frequently necessitate nutritional fortification, with fortification of human milk (HM) often extending into the postdischarge period. 2 HM is widely recognized as the preferred source of nutrition for infants and may be particularly important following gastrointestinal surgery due to its rich content of bioactive components that support mucosal healing and protect against infection, including immunoglobulins, HM oligosaccharides, bioactive proteins, and growth factors. 3 4 However, additional fortification is often required to meet the increased nutritional demands necessary for adequate growth following surgical repair.
HM-derived fortifiers allow infants to remain on an exclusive HM diet when fortification is required. However, current products are not available for use after hospital discharge, creating a gap in nutritional support for medically complex infants after transitioning home. The following case describes the use of freeze-dried mother's own milk (FDMOM) to fortify expressed mother's own milk (MOM) as a strategy to resolve feeding intolerance and weight faltering in an infant with complicated intestinal atresia and congenital shortened bowel due to apple peel deformity of the small intestine. 5
Case Report
A male singleton was delivered vaginally at 35 ^5/7^ weeks' gestation at a tertiary academic referral center with a Level IV neonatal intensive care unit (NICU) following preterm labor in the context of prenatal polyhydramnios with suspicion for bowel obstruction. The center provides comprehensive neonatal surgical and multidisciplinary nutrition support, including established HM-based feeding protocols for medically complex infants. Birth weight was 2.77 kg (weight-for-age 60th percentile, Fenton and Kim 2013 6 ; Fig. 1 ). An initial abdominal radiograph demonstrated a classic double-bubble sign with minimal distal bowel gas. At approximately 38 hours after birth, the infant underwent surgery for duodenal obstruction. Intraoperative findings revealed type IV duodenal atresia with two distinct areas of complete atresia and a markedly enlarged intervening segment, which was dilated to 9 cm (approximately eight times normal) and filled with bile. The distal small bowel also exhibited apple peel deformity and malrotation. The total length of the small bowel was 70 cm. Surgical repair involved resection of atretic segments with reanastomosis incorporating the intervening segment and resection of the apple peel deformity.
Weight-for-age Z-score (WAZ) trajectory in a late preterm infant with complex intestinal atresia. Following multiple intestinal surgeries, congenital shortened bowel, and prolonged periods of TPN, weight faltering was observed, with WAZ reaching a nadir of −1.24 SD on DOL 92. WAZ were calculated using Fenton 2013 growth references through 50 weeks postmenstrual age and WHO standards using corrected age thereafter. 6 7 During fortification with hypoallergenic formula powders (Nutramigen, Neocate, EleCare), clinically significant feeding intolerance was observed, characterized by abdominal distension, increased stooling, and irritability, which prompted a change in fortification strategy. After initiation of MOM fortified with FDMOM, an upward inflection in growth velocity was observed, with weight reaching 8,119 g (66th percentile; WAZ = 0.41 SD corrected age WHO) by DOL 200, approaching the catch-up growth target (8,375 g; 60th percentile WAZ uncorrected WHO standards). FDMOM, freeze-dried mother's own milk; DOL, day of life; MOM, mother's own milk; NPO, nil per os; TPN, total parenteral nutrition.
Postoperatively, the infant continued to exhibit signs of obstruction. Contrast follow-through showed marked dilation of the second and third segments of the duodenum with no distal contrast passage after 4 hours. The infant returned to surgery on day of life (DOL) 47. The intraoperative findings showed that the duodenal segment remained markedly dilated, and its excessive diameter was thought to impair effective peristalsis. The distal anastomosis had narrowed, consistent with a postoperative stricture. Significant resection of the dilated segment with a stepped tapering procedure was performed with revision of the distal anastomosis to restore luminal patency.
Nutrition and Intolerance Symptoms
The infant remained on total parenteral nutrition (TPN) for a total of 75 days, receiving hyperalimentation with SMOFlipid and Omegaven. Trophic feeds of MOM were started on DOL 63 and advanced by 10 mL/kg/day as tolerated. During initial hospitalization, the infant received MOM exclusively. He was discharged on DOL 80, weighing 4.68 kg (20th percentile) and taking MOM orally ad libitum.
The infant was readmitted on DOL 88 with dehydration and poor weight gain despite intake of approximately 850 mL of MOM daily. He had ≥15 loose stools daily. Weight upon readmission was 4.73 kg (10th percentile). Beginning on DOL 96, MOM was fortified with an extensively hydrolyzed formula powder to provide an additional 6.8 kcal/ 100 mL (equivalent to +2 kcal/ounce) (Nutramigen with Probiotic LGG, Mead Johnson Nutrition, Chicago, IL). The infant was discharged the following day. However, this fortification was discontinued on DOL 100 due to feeding intolerance, defined as abdominal distention, fussiness, increased stooling, and inability to tolerate feeds exceeding 30 mL. Subsequent fortification strategies using amino acid-based formula powders (Nutricia Neocate, Nutricia North America, Gaithersburg, MD, and Abbott Nutrition EleCare, Abbott Nutrition, Columbus, OH) were also associated with significant abdominal distention, discomfort, and continuation of increased stooling. Parents reported persistent irritability, poor sleep with intervals under 45 minutes, and inability to tolerate feed volumes greater than 30 mL. Neither the cow milk-based hydrolyzed formula nor the amino acid-based formulas were tolerated above +13.5 kcal/100 mL (equivalent to +4 kcal/ounce), the amount deemed necessary to achieve growth goals, assuming the MOM caloric density of 20 kcal/ounce.
Ongoing symptoms prompted a medically supervised trial of FDMOM fortification. Frozen MOM was processed in a certified Good Manufacturing Practices (cGMP) facility using a patented, contactless freeze-drying method (SafeDry, Milkify, Inc., Houston, TX) with subsequent water activity testing (AQUALAB3, Addium, Pullman, WA) to confirm low residual moisture and mitigate microbial risk. Macronutrient composition of both baseline MOM and FDMOM was measured using a MIRIS Human Milk Analyzer (08-02-107, Uppsala, Sweden; Table 1 ). These measurements revealed a baseline MOM caloric density of 63.2 kcal/100 mL (equivalent to 18.7 kcal/ounce) and an FDMOM caloric density of 4.83 kcal/g. A targeted fortification strategy was then developed using these measurements, incorporating both MIRIS-derived nutrient density and water activity data, to calculate the amount of FDMOM required to increase the caloric density of baseline MOM by +20.3 kcal/100 mL (equivalent to +6 kcal/ounce).
FDMOM fortification of +20.3 kcal/100 mL (equivalent to +6 kcal/ounce). began on DOL 122, resulting in immediate and sustained improvement in feeding tolerance. Within 24 hours, abdominal distention resolved, and the infant was able to consistently finish full fortified feeds with no further signs of intolerance observed. Parents reported a marked improvement in his overall disposition, and weight-for-age reached the 66th percentile by DOL 200 (WHO reference standard using corrected age 7 ).
Discussion
To our knowledge, this is the first reported case of targeted postdischarge fortification using FDMOM in an infant with complicated intestinal atresia and congenital shortened bowel due to an apple peel deformity. This late preterm infant was at high risk for growth failure due to two separate surgical repairs, congenitally shortened bowel, prolonged dependence on TPN, and ongoing feeding intolerance. Following discharge, the infant was readmitted with dehydration and poor weight gain. Fortification with hydrolyzed cow milk-based and amino acid-based formulas resulted in significant intolerance. In contrast, intolerance resolved within 24 hours of initiating FDMOM fortification, with subsequent rapid catch-up growth. Weight-for-age plotted with the WHO standards using corrected age reached the 66th percentile within 86 days, demonstrating meaningful improvement in both feeding tolerance and growth following the transition to FDMOM fortification of MOM.
This case underscores key safety considerations for the use of FDMOM as a fortifier. Targeted fortification was possible by measurement of baseline MOM caloric density, which was 18.7 kcal/ounce, below the standard 20 kcal/ounce assumption. Existing data show that freeze-drying preserves the majority of macro- and micronutrients and many bioactive components, 8 with only modest reductions that supplement rather than displace fresh MOM. Our macronutrient analysis supports these findings.
Microbial safety is a primary consideration when evaluating FDMOM for postdischarge fortification in medically fragile infants. In this case, freeze-drying was performed in a cGMP facility using a patented, contact-free process designed to prevent environmental exposure and cross-contamination with HM from other mothers. This closed-system approach offers a substantial safety advantage over traditional freeze-drying methods involving direct contact with equipment and exposure to the surrounding environment. Additional safeguards included environmental pathogen monitoring, water activity testing of the final powder to prevent postdrying microbial growth, and medically supervised fortification with individualized mixing protocols. These measures were essential for the safe implementation of FDMOM fortification in this vulnerable patient.
Some evidence suggests that HM-based fortifiers may be associated with reduced feeding intolerance compared with cow milk-based fortifiers, although findings remain mixed and data on postdischarge strategies are limited. 9 10 11 FDMOM may offer additional advantages by avoiding industrial pasteurization while largely preserving the native composition of MOM. 12
Conclusion
In summary, this case demonstrates the feasibility and potential clinical benefit of medically supervised, targeted postdischarge fortification using FDMOM in select high-risk infants with weight faltering and feeding intolerance. It highlights a critical gap in postdischarge nutritional care and warrants further investigation.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Riddle S Karpen H Special populations-surgical infants Clin Perinatol 2023500371572837536774 10.1016/j.clp.2023.04.008 · doi ↗ · pubmed ↗
- 2Haiden N Luque V Domellöf M Assessment of growth status and nutritional management of prematurely born infants after hospital discharge: A position paper of the ESPGHAN Nutrition Committee J Pediatr Gastroenterol Nutr 2025810242144140341618 10.1002/jpn 3.70054 · doi ↗ · pubmed ↗
- 3Ballard O Morrow A L Human milk composition: nutrients and bioactive factors Pediatr Clin North Am 20136001497423178060 10.1016/j.pcl.2012.10.002PMC 3586783 · doi ↗ · pubmed ↗
- 4Section on Breastfeeding Meek J Y Noble L Policy Statement: Breastfeeding and the Use of Human Milk Pediatrics 202215001 e 202205798835921640 10.1542/peds.2022-057988 · doi ↗ · pubmed ↗
- 5Seashore J H Collins F S Markowitz R I Seashore M R Familial apple peel jejunal atresia: Surgical, genetic, and radiographic aspects Pediatrics 198780045405443309863 · pubmed ↗
- 6Fenton T R Kim J HA systematic review and meta-analysis to revise the Fenton growth chart for preterm infants BMC Pediatr 2013135923601190 10.1186/1471-2431-13-59PMC 3637477 · doi ↗ · pubmed ↗
- 7WHO Multicentre Growth Reference Study Group WHO Child Growth Standards based on length/height, weight and age Acta Paediatr Suppl 2006450768516817681 10.1111/j.1651-2227.2006.tb 02378.x · doi ↗ · pubmed ↗
- 8Sproat T DR Ghosh A Alshaikh B N Lyophilized (freeze-dried) human milk for preterm infants: A scoping review J Perinatol 2024440561262738225373 10.1038/s 41372-023-01861-8 · doi ↗ · pubmed ↗