Endoscopic ultrasonography-guided rendezvous and fine-caliber multi-hole metal stent for postoperative pancreatic anastomotic stricture
Tatsuya Kurokawa, Hirotsugu Maruyama, Yuji Kawata, Yoshinori Shimamoto, Yuki Ishikawa-Kakiya, Kojiro Tanoue, Yasuhiro Fujiwara

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
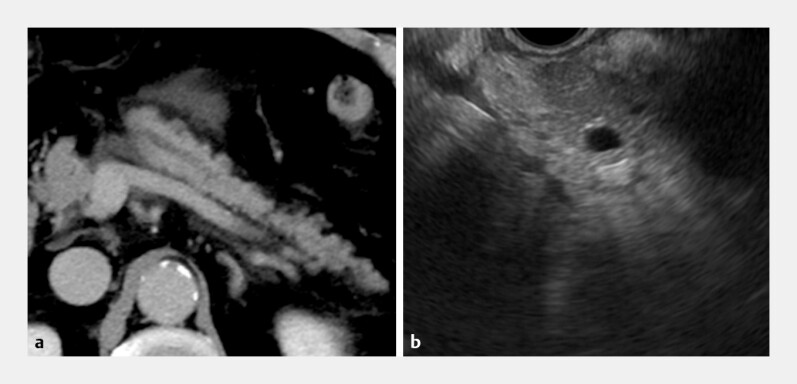 Fig. 1
Fig. 1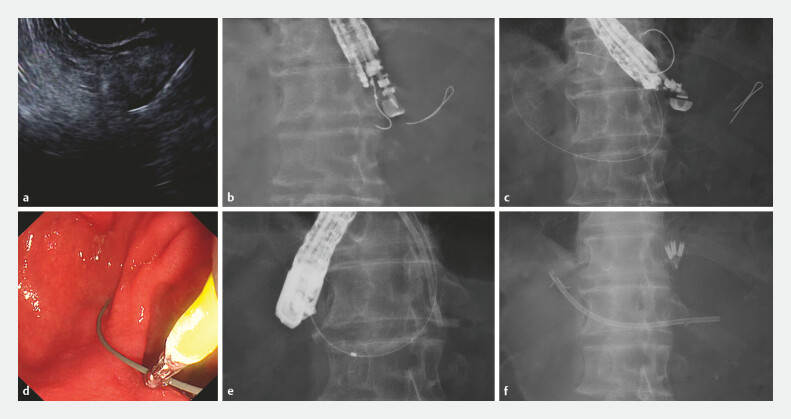 Fig. 2
Fig. 2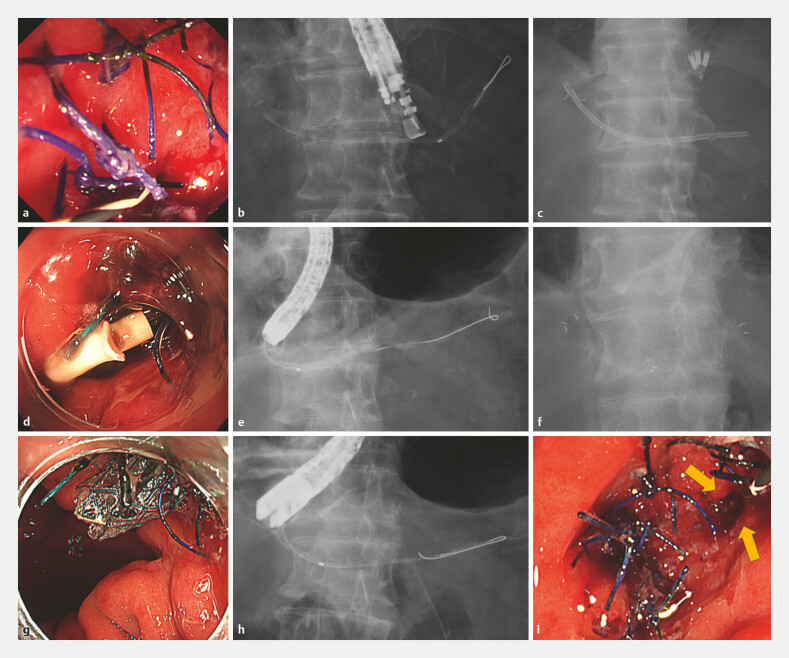 Fig. 3
Fig. 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPancreatic and Hepatic Oncology Research · Gallbladder and Bile Duct Disorders · Esophageal and GI Pathology
Endoscopic treatment for postoperative pancreatic anastomotic strictures is challenging 1 2 . Difficulty in identifying the anastomotic site and the need for repeated plastic stent exchanges further complicate treatment 2 . In such cases, treatment that ensures reliable access to the anastomotic site and directly improves the stricture itself is required 3 4 . Here, we report a case in which an endoscopic ultrasonography (EUS)-guided rendezvous technique successfully secured pancreatic duct access, enabling the effective treatment of a postoperative anastomotic stricture using a novel fine-caliber, multi-hole self-expandable metal stent (MHSEMS). A 73-year-old man who had undergone middle pancreatectomy with gastro-pancreatic anastomosis 15 years earlier presented with abdominal pain. Computed tomography suggested pancreatitis due to an anastomotic stricture ( Fig. 1 ). Pancreatic duct stenting was unsuccessful, and he was referred to our hospital. An EUS-guided rendezvous procedure was performed. Using a 22-gauge FNA needle, the dilated distal pancreatic duct was punctured, and a 0.018-inch guidewire was advanced distally. A double-lumen catheter was used to redirect a 0.025-inch guidewire across the anastomosis and into the stomach. A duodenoscope (TJF-290; Olympus, Tokyo, Japan) was then used to complete the rendezvous and placed a 7 Fr plastic pancreatic stent ( Fig. 2 ). One month later, the plastic stent was exchanged for an MHSEMS (6 mm × 8 cm; Hanarostent Biliary Multi-Hole Benefit; M.I. Tech, Pyeongtaek, South Korea) using a therapeutic gastroscope (GIF-290T; Olympus, Tokyo, Japan). Two months later, the MHSEMS was removed easily using grasping forceps with a duodenoscope ( Video 1 and Fig. 3 ). The anastomosis remained patent, and the patient remained symptom-free 5 months after stent removal.
Preprocedural imaging. a Contrast-enhanced computed tomography showing pancreatic duct dilatation distal to the anastomosis with peripancreatic fluid collection consistent with acute pancreatitis. b Endoscopic ultrasonography demonstrating a dilated pancreatic duct distal to the anastomosis.
EUS-guided rendezvous placement of a plastic pancreatic stent across the anastomotic stricture. a Pancreatography after puncture showing the dilated pancreatic duct distal to the anastomosis. b A guidewire advanced into the stomach via the anastomosis. c Placement of a plastic pancreatic stent across the anastomotic stricture using the rendezvous approach. d The 0.025-inch guidewire was grasped with biopsy forceps and carefully drawn into the working channel. e With the rendezvous technique, a catheter was advanced across the anastomosis over the guidewire. f A plastic pancreatic stent was placed across the anastomosis. EUS, endoscopic ultrasonography.
EUS-guided rendezvous and MHSEMS dilation for the postoperative pancreatic anastomotic stricture. EUS, endoscopic ultrasonography.Video 1
Serial endoscopic and fluoroscopic findings during treatment. a An endoscopic view of the stenotic postoperative anastomosis. b Pancreatography demonstrating upstream pancreatic duct dilatation. c A fluoroscopic image showing plastic stent placement across the anastomosis. d An endoscopic view after plastic stent placement across the anastomosis. e Pancreatography after plastic stent removal showing improved pancreatic duct dilatation. f A fluoroscopic image showing the deployment of the MHSEMS across the anastomosis. g An endoscopic view after MHSEMS deployment across the anastomosis. h Pancreatography after MHSEMS removal showing the resolution of pancreatic duct dilatation. i An endoscopic view of the patent anastomosis after MHSEMS removal.
This 6 mm MHSEMS achieved effective dilation of a postoperative pancreatic anastomotic stricture. Its design could reduce the risks of pancreatitis and migration. The combination of the EUS-guided rendezvous technique allows more reliable treatment of pancreatic duct anastomotic strictures.
Endoscopy_UCTN_Code_TTT_1AS_2AI
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Kikuyama M Itoi T Ota Y Therapeutic endoscopy for stenotic pancreatodigestive tract anastomosis after pancreatoduodenectomy (with videos)Gastrointest Endosc 20117337638210.1016/j.gie.2010.10.01521295649 · doi ↗ · pubmed ↗
- 2Kida A Shirota Y Kawane T Long-term outcomes after endoscopic retrograde pancreatic drainage for symptomatic pancreaticojejunal anastomotic stenosis Sci Rep 202111448910.1038/s 41598-021-84024-z 33627731 PMC 7904781 · doi ↗ · pubmed ↗
- 3Chen YI Levy MJ Moreels TG An international multicenter study comparing EUS-guided pancreatic duct drainage with enteroscopy-assisted endoscopic retrograde pancreatography after Whipple surgery Gastrointest Endosc 20178517017710.1016/j.gie.2016.07.03127460390 · doi ↗ · pubmed ↗
- 4Bhurwal A Tawadros A Mutneja HEUS guided pancreatic duct decompression in surgically altered anatomy or failed ERCP – A systematic review, meta-analysis and meta-regression Pancreatology 202121990100010.1016/j.pan.2021.03.02133865725 · doi ↗ · pubmed ↗