Endoscopic ultrasound-guided botulinum toxin injection to prevent mis-injection: improving safety and potential efficacy in spastic esophageal disorders
Abdeldjalil Sais, Jérôme Rivory, Alexandru Lupu, Jean Grimaldi, Mathieu Pioche

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
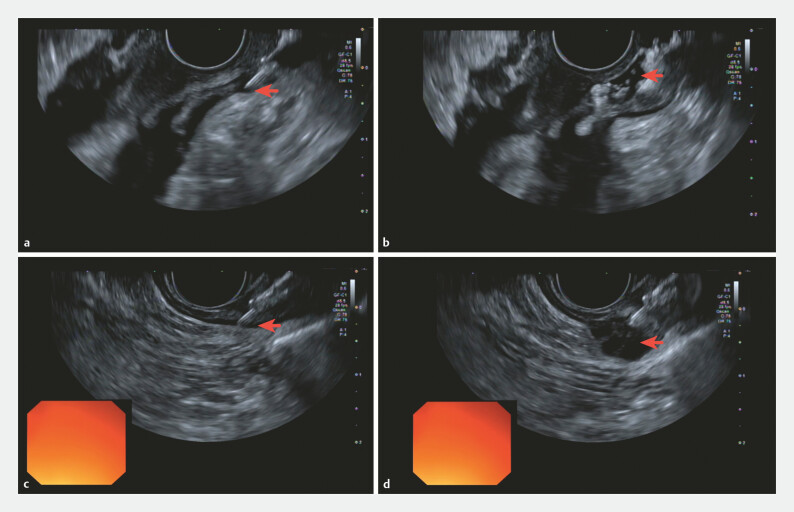 Fig. 1
Fig. 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGastroesophageal reflux and treatments · Dysphagia Assessment and Management · Esophageal Cancer Research and Treatment
A 69-year-old man presented with disabling solid dysphagia evolving into painful crises despite medical therapy. Initial endoscopy showed no stricture and mild cardiospasm; no mechanical obstruction was observed. A barium esophagogram demonstrated a reduced expansion in the distal thoracic esophagus without stasis and without radiological evidence of lower esophageal sphincter hypertonia.
High-resolution manometry was initially inconclusive, but repeated manometry with a solid provocation reproduced the patient’s “blockage” episodes and showed esophageal shortening with pressurization of the upper half of the esophagus and a few distal spastic contractions, while integrated relaxation pressure remained normal.
Botulinum toxin injection is sometimes used as a rescue therapy in refractory spastic esophageal disorders 1 when per oral endoscopic myotomy is not indicated and was proposed by the motility multidisciplinary team meeting of our hospital. Nevertheless, our experience includes one case of fatal mediastinitis attributable to a misdirected injection of the toxin 2 and a precise protocol of previous antibiotics and directed injection in the muscle layer was proposed following this severe issue.
Therefore, we performed injection under linear endoscopic ultrasound (EUS) guidance to maximize intramuscular delivery and minimize extramural mis-injection 3 . Under general anesthesia with intubation, linear EUS confirmed muscular thickening without a clearly predominant segment. A standard endoscopic sclerotherapy needle was used to deliver the botulinum toxin in multiple small volumes along the distal 10 cm of the esophagus ( Video 1 ). Continuous EUS monitoring was used to keep the needle tip within the muscularis propria and avoid injection “behind” the muscle. As shown in the second part of the video, when the needle position was not optimal ( Fig. 1 a ), the injection was immediately stopped ( Fig. 1 b ), and the needle was repositioned before continuing ( Fig. 1 c ), aiming to both prevent adverse events and improve efficacy by ensuring true intramuscular deposition ( Fig. 1 d ).
EUS-guided targeting and real-time needle repositioning for botulinum toxin injection. a Initial needle insertion into the submucosal layer. b Identification of a misdirected injection site located extramurally, posterior to the muscularis propria. c Real-time ultrasound-guided repositioning of the sclerotherapy needle into the muscularis propria. d Successful intramuscular deposition of the botulinum toxin. EUS, endoscopic ultrasound.
Endoscopic ultrasound-guided botulinum toxin injection to prevent mis-injection in spastic esophageal disorders.Video 1
No immediate adverse event occurred. The patient was discharged with 3 days of amoxicillin–clavulanate. At a 2-month follow-up, the patient reported complete resolution of painful dysphagia crises with significant clinical improvement. EUS-guided targeting may represent a safer and potentially more efficient approach by preventing mis-injection and reducing the risk of rare but serious complications.
Endoscopy_UCTN_Code_CCL_1AB_2AC_3AH Endoscopy_UCTN_Code_TTT_1AO_2AP
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Weusten BLAM Barret M Bredenoord AJ Endoscopic management of gastrointestinal motility disorders – part 2: European Society of Gastrointestinal Endoscopy (ESGE) Guideline Endoscopy 20205260061410.1055/a-1171-317432462649 · doi ↗ · pubmed ↗
- 2Marjoux S Pioche M Benet T Fatal mediastinitis following botulinum toxin injection for esophageal spasm Endoscopy 201345 E 405E 40610.1055/s-0033-134490824285073 · doi ↗ · pubmed ↗
- 3Hoffman BJ Treatment of achalasia by injection of botulinum toxin under endoscopic ultrasound guidance Gastrointest Endoscopy 202645777910.1016/s 0016-5107(97)70306-79013174 · doi ↗ · pubmed ↗