Combined use of drug-eluting stent and drug-coated balloon for tandem lesion with spontaneously recanalized coronary thrombus: insights from optical coherence tomography
Satoshi Terashima, Takashi Kataoka, Ken Harada

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
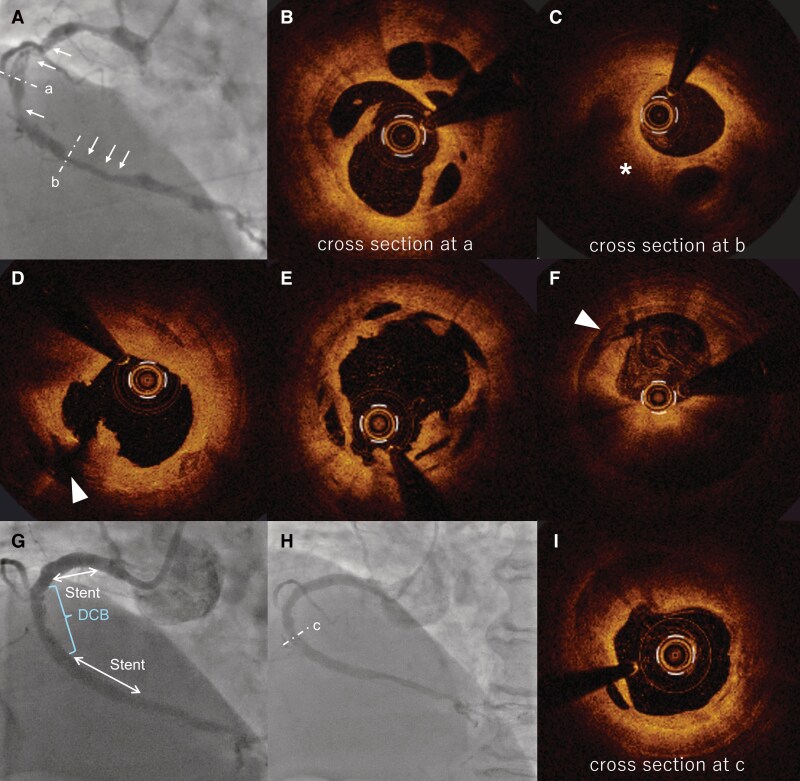 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCoronary Interventions and Diagnostics · Ultrasound and Hyperthermia Applications · Cerebrovascular and Carotid Artery Diseases
Case description
A 70-year-old woman with type 2 diabetes mellitus presented with progressive chest pain on exertion following an episode of sudden chest pain at rest two weeks earlier. Coronary angiography revealed a severe stenosis with a braid-like appearance extending from proximal to distal segments of the right coronary artery (RCA) (Figure 1A, arrows). Angiography suggested a spontaneously recanalized coronary thrombus (SRCT), which previous reports indicate is often physiologically significant.^1^
(A) Coronary angiography indicating tandem lesion (arrows) with a braid-like appearance in both the proximal and distal of RCA. (B) OCT imaging from cross section at (A) showing a lotus root-like appearance. (C) OCT imaging from cross section at (B) showing a lotus root-like appearance and mural thrombi (asterisk). (D) Cross-sectional OCT image of the proximal RCA after lesion preparation, demonstrating a major dissection extending into media (arrowhead). (E) Cross-sectional OCT image at (A) after preparation, showing well-controlled dilatation and an adequately enlarged lumen. (F) Cross-sectional OCT image at (B) after preparation, demonstrating a major dissection extending into the media (arrowhead) and residual plaque volume. (G) Final angiography of PCI showing lesions treated with DES and DCB. (H) Coronary angiography at the one-year follow-up. (I) OCT imaging from the cross-section at (C), which had been treated with DCB. DCB, drug-coated balloon; DES, drug-eluting stent; MLA, minimum lumen area; OCT, optical coherence tomography; PCI, percutaneous coronary intervention; RCA, right coronary artery.
Optical coherence tomography (OCT)-guided percutaneous coronary intervention (PCI), which is associated with favourable outcomes,^2^ was performed. OCT imaging revealed a tandem lesion with lotus root-like appearances and mural thrombi (Figure 1C, asterisk) extending over 100 mm (Figure 1B and C). Although optimal PCI strategy for SRCT is not well established, drug-eluting stents (DES) implantation has shown promising results, and drug-coated balloons (DCB) may offer an alternative.^3^ Following adequate lesion preparation with a cutting balloon, angiography showed residual stenosis greater than 50% in proximal and distal segments while mid segment had comparatively less stenosis. Additionally, OCT revealed that the proximal and distal lesions had developed major dissections extending to the media (Figure 1D and F, arrowheads), whereas the mid lesion demonstrated a well-controlled dissection with relatively less plaque volume (Figure 1E). To minimize risks associated with full coverage of RCA using multiple overlapping DES, a hybrid approach using DES and DCB was adopted (Figure 1G).
One year after treatment, she developed exertional dyspnoea with progression in the left anterior descending artery. OCT-guided PCI was performed for the de novo lesion, and RCA was examined. Angiography of RCA demonstrated sustained patency of the treated lesion (Figure 1H). OCT imaging at the DCB-treated site showed favourable expansion at minimum lumen area (Figure 1I). This case highlights the successful use of combined DES and DCB therapy for extensive SRCT, suggesting its potential as a viable treatment strategy.
Supplementary Material
ytag194_Supplementary_Data
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Xu T, Shrestha R, Pan T, Huang X, Xu H, Zhang JJ, et al Anatomical features and clinical outcome of a honeycomb-like structure in the coronary artery: Reports from 16 consecutive patients. Coron Artery Dis 2020;31:222–229.31658133 10.1097/MCA.0000000000000822 · doi ↗ · pubmed ↗
- 2Souteyrand G, Valladier M, Amabile N, Derimay F, Harbaoui B, Leddet P, et al Diagnosis and management of spontaneously recanalized coronary thrombus guided by optical coherence tomography- lessons from the French “Lotus root” registry. Circ J 2018;82:783–790.29199266 10.1253/circj.CJ-17-0810 · doi ↗ · pubmed ↗
- 3Yoshioka G, Nishihira K, Shibata Y, Node K. First report of lotus root-like appearance at the site of coronary spasm in a patient with acute coronary syndrome. Eur Heart J Case Rep 2020;4:1–2.