The role of noninfectious comorbidities in the association between severe infections and risk of dementia in Finland: A nationwide registry study
Pyry N. Sipilä, Kaarina Korhonen, Joni V. Lindbohm, Mika Kivimäki, Pekka Martikainen, Suzanne De Bruijn, Alison Farrell, Suzanne De Bruijn, Suzanne De Bruijn, Suzanne De Bruijn

TL;DR
This study finds that severe infections are independently linked to higher dementia risk, even after accounting for other noninfectious diseases.
Contribution
The study demonstrates that severe infections remain significant dementia risk factors even after adjusting for 27 comorbid noninfectious diseases.
Findings
Severe infections like cystitis and bacterial infections remained independently associated with dementia risk after adjusting for 27 comorbid diseases.
29 hospital-treated diseases were found to be robustly associated with increased dementia risk.
The association between infections and dementia was consistent across subgroups and stronger for early-onset dementia cases.
Abstract
Severe infections have been linked to an increased risk of dementia, but both conditions often coexist with other illnesses that may confound this association. Using nationwide Finnish health registry data, we examined the role of noninfectious mental and physical illnesses in the association between severe infections and dementia. This register-based study included 62,555 individuals aged 65 or older in Finland in 2016 who were diagnosed with late-onset dementia between 2017 and 2020 and 312,772 dementia-free controls matched for year of birth, sex, and the follow-up period. Analyses were adjusted for education, marital status, employment, and area of residence, with age and sex accounted for through the matched conditional design and analysis. Applying a 1-year lag period, we identified 29 hospital-treated diseases that occurred 1–21 years before dementia diagnosis in cases (or index…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
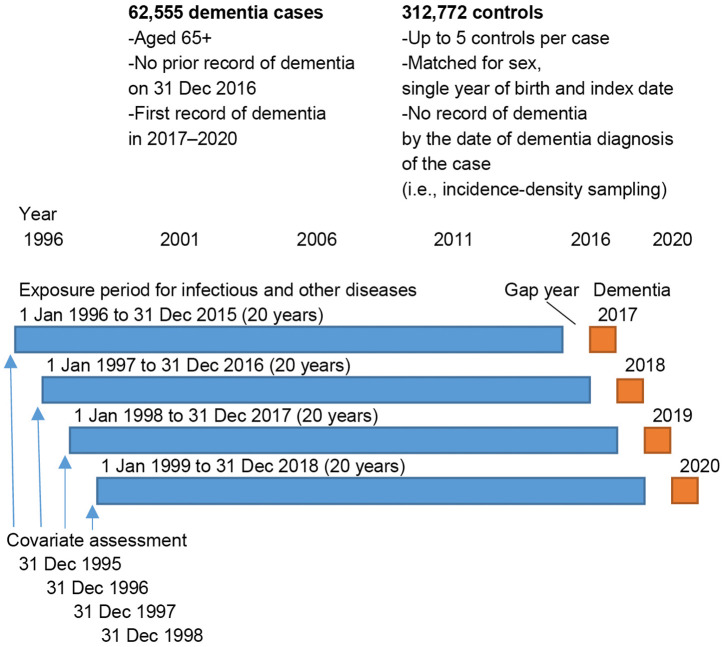 Fig 1
Fig 1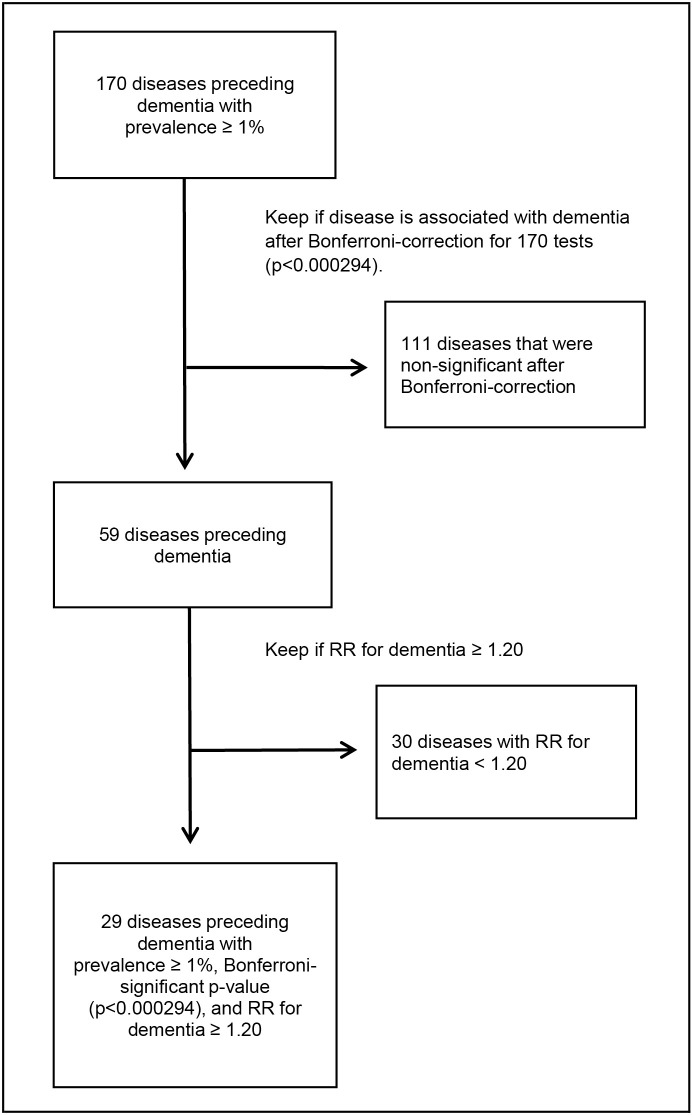 Fig 2
Fig 2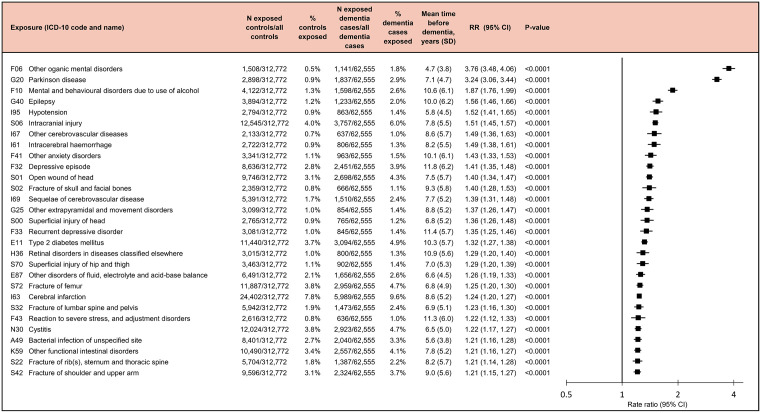 Fig 3
Fig 3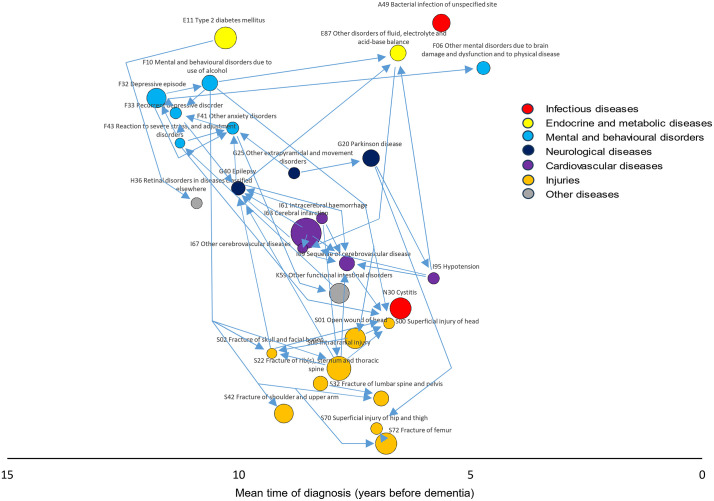 Fig 4
Fig 4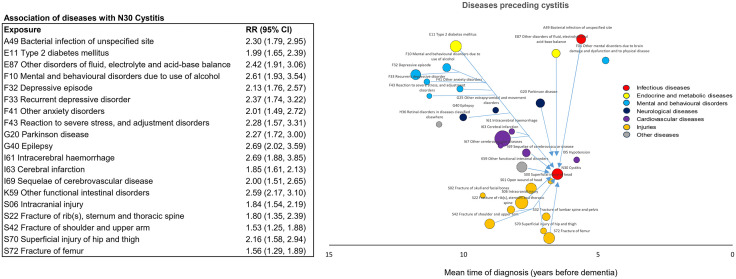 Fig 5
Fig 5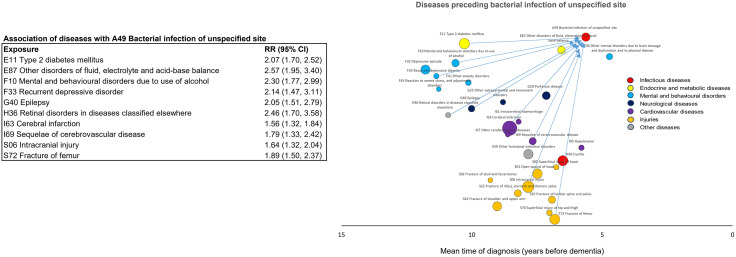 Fig 6
Fig 6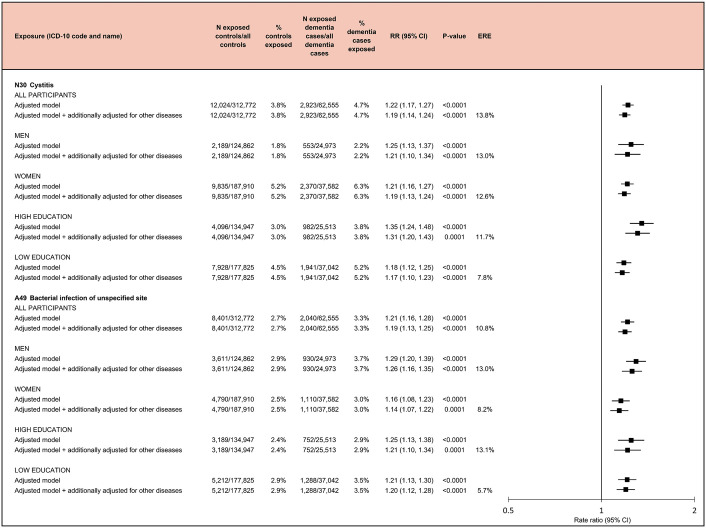 Fig 7
Fig 7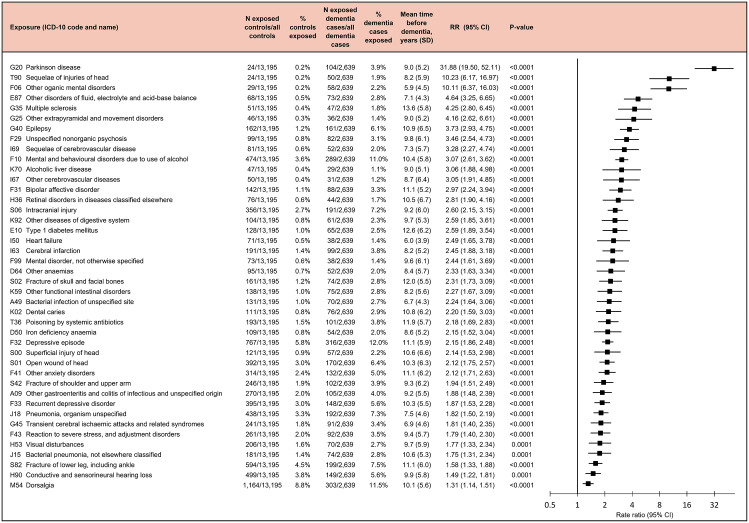 Fig 8
Fig 8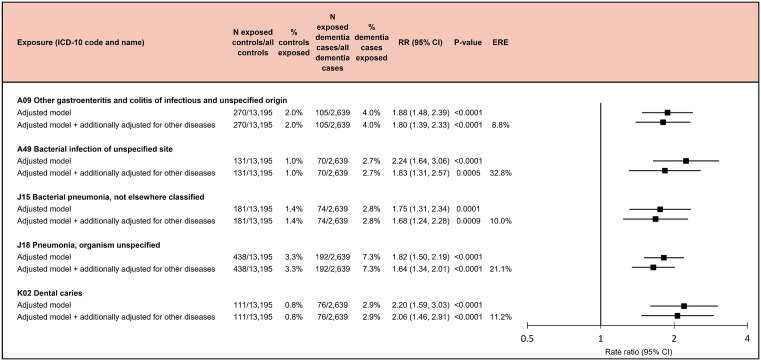 Fig 9
Fig 9- —http://dx.doi.org/10.13039/501100004756Emil Aaltosen Säätiö
- —http://dx.doi.org/10.13039/100008723Suomen Lääketieteen Säätiö
- —http://dx.doi.org/10.13039/501100004212Päivikki ja Sakari Sohlbergin Säätiö
- —Research Council of Finland
- —http://dx.doi.org/10.13039/100010269Wellcome Trust
- —http://dx.doi.org/10.13039/501100000265Medical Research Council
- —http://dx.doi.org/10.13039/100000049National Institute on Aging
- —http://dx.doi.org/10.13039/100000049National Institute on Aging
- —Research Council of Finland
- —http://dx.doi.org/10.13039/100010663H2020 European Research Council
- —http://dx.doi.org/10.13039/501100009047Strategic Research Council
- —http://dx.doi.org/10.13039/501100009047Strategic Research Council
- —Research Council of Finland
- —http://dx.doi.org/10.13039/501100004012Jane ja Aatos Erkon Säätiö
- —http://dx.doi.org/10.13039/501100004189Max-Planck-Gesellschaft
- —http://dx.doi.org/10.13039/100007797Helsingin Yliopisto
- —http://dx.doi.org/10.13039/501100020085Helsingin Kaupunki
- —Vantaan kaupunki
- —Espoon kaupunki
- —Helsinki University Library
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsUrinary Tract Infections Management · Dementia and Cognitive Impairment Research · Geriatric Care and Nursing Homes
Introduction
Growing evidence from observational cohort studies suggests that severe (hospital-treated) infections are associated with an increased risk of dementia [1–6]. Several plausible mechanisms have been proposed to explain this association, including disturbed peripheral-central immune crosstalk, which contributes to neuroinflammation [7,8]; inflammation-induced blood-brain barrier dysfunction and related entry of neurotoxic plasma components, blood cells and pathogens into the central nervous system [9]; and infection-related vascular mechanisms, such as platelet activation, inflammation-induced thrombosis, and endothelial dysfunction in the brain [10,11].
However, given its typical late-onset, clinically diagnosed dementia rarely occurs in isolation from other age-related diseases [12,13]. Longitudinal studies have identified cascades of physical and mental diseases that develop over several years before clinical dementia manifests [14,15]. Many of these diseases also increase the risk of infections [16–20]. To date, few studies have examined the extent to which comorbid conditions, such as diabetes, cardio- and cerebrovascular diseases, and depression, contribute to the excess dementia risk observed among individuals with severe infections. A major barrier for this research is the need for large population samples and extended follow-ups to track disease progression over time. As a result, it remains unclear whether severe infections independently increase the risk of dementia.
We addressed this knowledge gap in the following ways. First, to ensure comprehensive analysis, we applied a phenome-wide approach, including all hospital presenting diseases or disease groups as defined in the International Classification of Diseases, 10th revision (ICD-10), with a prevalence of 1% or higher among dementia cases. We assessed which of these diseases were associated with an increased risk of dementia among dementia cases and controls drawn from the total population of Finland. Second, to examine the sequence, timing, and inter-relatedness of the identified dementia-related diseases, we analysed disease trajectories and disease networks over 20 years preceding dementia onset, focussing on conditions that preceded both severe infections and dementia. Third, we assessed the extent to which the association between severe infections and dementia risk remains after accounting for other dementia-related diseases. We anticipated identifying several infectious and noninfectious diseases that are interrelated and associated with dementia risk in Finnish adults. We hypothesised that severe infections increase the likelihood of developing dementia at least partly independently of preceding noninfectious comorbidities.
Methods
Study population and register linkage
This study focussed on the Finnish population aged 65+ (born 1951 or earlier), free of dementia, and residing in Finland on 31 December 2016. A supplementary analysis of early onset dementia was conducted among the total Finnish population aged 18–64 during the study period (born 1953–1977). Statistics Finland provided demographic and mortality data. Using unique personal identification codes, Statistics Finland linked the study individuals to hospitalisation records from the Care Register of the Finnish Institute for Health and Welfare and to medication reimbursement and purchase data recorded by the Social Insurance Institution of Finland.
All the data were pseudonymised before release to researchers and data analysis was approved by Statistics Finland Board of Ethics (permit no. TK/1836/07.03.00/2024) and the Social and Health Data Permit Authority Findata (permit no. THL/6846/14.02.00/2024). Informed consent was not required for this study, because only administrative register data were used (the Finnish Personal Data Act and the Statistics Act).
Study design and sampling of controls
This observational study includes individuals aged 65 or older living in Finland in 2016 who were diagnosed with late-onset dementia between 2017 and 2020 and who also resided in Finland at the start of the exposure period on 1 January 1996–1 January 1999 (residence recorded on 31 December 1995–31 December 1998). Immigrants who arrived after the baseline of 1996–1999 were excluded. Using incidence-density sampling with replacement, we aimed to identify 5 controls for each dementia case, matching exactly for year of birth, sex, and follow-up period. Controls were required to be at risk (i.e., dementia-free) at the time of the matched case’s dementia diagnosis (the index date) but could later become cases if diagnosed with dementia after that date. Five suitable controls were found for almost all cases, resulting in a final sample of 62,555 dementia cases and 312,772 controls. Those who died were censored from the risk pool on the last day of the year of death. Emigration after 2016 was very rare (~0.05% annually) [21]. Therefore, we assumed that all study individuals at the end of 2016 continued living in Finland until the end of 2020 unless they died. The incidence-density sampling approach guarantees that controls are sampled from person-time at risk and, therefore, the resulting odds ratios from matched analysis represent rate ratios (RR) [22,23]. In additional analyses, we also examined early onset dementia (age of onset <65 years) using a similar sampling scheme.
Hospitalisations from severe infections or other nondementia illnesses (exposures)
Using hospital inpatient and outpatient records, we ascertained all diseases recorded as a primary diagnosis of the encounter during a two-decade exposure window 1–21 years before dementia diagnosis for dementia cases and the index date for matched controls (Fig 1). The exposure window was set at 21 years, corresponding the longest period for which ICD-10 data were available. A long exposure period was necessary because dementia typically develops over many years or even decades [24]. Diagnoses recorded <1 year before dementia onset or index date were not included to reduce bias from delays in the recording of the dementia diagnoses. Thus, depending on the year of dementia diagnosis or index date in 2017–2020, the timespan for disease ascertainment started between 1 January 1996 and 1 January 1999 and ended between 31 December 2015 and 31 December 2018, respectively. We analysed each 3-digit ICD-10 disease code as a separate entity and did not attempt to group codes that may refer to overlapping or clinically similar conditions, including ICD-10 chapters I–XIV, XIX, and XX, which contain diseases, injuries, and related conditions. Chapters XV, XVI, XVII, XVIII, XXI, and XXII were not included, because they mostly refer to nondisease events, such as pregnancy and childbirth, perinatal period, congenital malformations, unspecific symptoms, administration, and other special purposes.
Study design.The figure outlines the criteria used to select dementia cases and matched controls and illustrates the study design, including baseline covariate assessment, the 20-year exposure window for identifying infectious and noninfectious dementia-related diseases, the gap year before dementia diagnosis, and the dementia diagnosis year (2017–2020).
Ascertainment of all-cause dementia cases
We retrieved diagnoses of dementia from three sources: primary and secondary diagnoses in hospital inpatient and outpatient records; medication reimbursement entitlements for the treatment of dementia; and purchases of prescribed antidementia medications (the Anatomical Therapeutic Chemical [ATC] code N06D). We defined all-cause dementia using the ICD-10 codes F00–F03, F05.1, G30, G31.0, G31.1, and G31.8 [1]. Incident cases of dementia were recorded between 1 January 2017 and 31 December 2020. Individuals with a record of prevalent all-cause dementia between 1 January 1996 (the inception of ICD-10 in Finland) and 31 December 2016 were excluded. To further ensure that the individuals did not have prevalent dementia at the start of the exposure window (from 1 January 1996 to 1 January 1999), we also excluded individuals who had a record of any dementia-related 9th revision (ICD-9) codes (290, 2900A, 2941A, 3310A, 3311A, 3312X, 3318X, and 4378A) between 1 January 1987 and 31 December 1995, the time-period when ICD-9 was in use in Finland.
Hospital inpatient records were included from the beginning of the use of ICD-9 in Finland in 1987 and were available until 2020. Hospital outpatient records were available from 1998 to 2020, reimbursement data for antidementia medications from 1999 to 2018, and prescribed medication purchase data for antidementia medications from 2000 to 2019.
Covariates
We considered sex, education, marital status, employment, and area of residence as covariates. These data were obtained from Statistics Finland registries. We used the first records immediately before the start of disease ascertainment in 1996–1999. Based on International Standard Classification of Education (ISCED) 2011, highest achieved education was categorised into three groups for adjustments (tertiary; secondary; basic or no qualifications) and dichotomised into high versus low for stratified analyses (tertiary or secondary versus basic or no qualifications). Marital status was recorded as married, never married, divorced, and widowed. Employment status was recorded as employed (aged<60); retired early (aged<60); other nonworking (aged<60); entitled to old-age retirement (aged 60+) [25]. In Finland, public healthcare covers a great majority of hospitalisations and is organised on a regional basis. To account for potential regional differences in healthcare, we adjusted our models for area of residence using 19 dummy variables which corresponded to the administrative regional division confirmed by the Finnish Government. The three largest regions by population were Uusimaa (comprising the capital Helsinki and surrounding areas), Pirkanmaa (Tampere and surrounding areas), and Southwest Finland (Turku and surrounding areas). In sensitivity analyses, we additionally examined household income quintiles as defined by Statistics Finland and use of medications for hypertension, diabetes, and coronary heart disease based on medication reimbursement entitlements from the Social Insurance Institution of Finland as covariates.
Statistical analysis
In the first part of the data analysis, we identified diseases that were associated with an increased risk of incident dementia. This was done through three steps. First, we identified all diseases that preceded dementia with a prevalence of at least 1% during the exposure window (1–21 years before dementia diagnosis). As in genetic studies of common versus rare variants, we chose the 1% threshold to focus on relatively common diseases that have relevance on the population health level [26]. Second, we analysed the associations between all these diseases and incident dementia using conditional logistic regression, adjusting for education, marital status, employment, and area of residence. Adjustment for age and sex was inherent to the matched conditional design and analysis, as matching was performed on year of birth, index date, and sex [27]. Third, diseases showing a statistically significant association with dementia after Bonferroni correction (p < 0.000294) and an RR of at least 1.20 were selected for further analysis. The RR threshold of 1.20 was chosen based on literature indicating that smaller effect sizes are often of limited public health relevance and more susceptible to bias, unless the disease incidence is very high [15,28,29].
In the second part of the data analysis, we constructed disease trajectories and networks across dementia-related diseases in four steps. First, we identified associations between all the possible pairs of dementia-related diseases identified in the first part of the data analysis. This was done among the dementia cases using the same 20-year exposure window as with the dementia analysis (from 1 January 1996–1 January 1999 to 31 December 2015–31 December 2018). Because any pair of diseases can occur in two temporal sequences (A → B or B → A), we first determined which sequence occurred more often in the data. That sequence was used in all primary trajectory analyses, while the alternative sequence was assessed in supplementary analyses. Second, as in the analysis for incident dementia, we used incidence-density sampling for each disease, identifying up to 5 controls per disease case, matched for year of birth, index date, and sex. For virtually all disease cases, five appropriate controls were identified, with incomplete matches only occurring in ≤0.4% of cases. Third, after establishing the analytic design in the previous steps, we examined the strength of the associations between disease pairs using conditional logistic regression adjusted for education, marital status, employment, and area of residence, and for age and sex inherently to the matched conditional design and analysis. P-values were adjusted for multiple testing using Bonferroni correction. Fourth, Bonferroni significant disease pairs in which the first disease had an RR of ≥1.20 for the occurrence of the second disease were retained in analysis. From these dementia-related disease pairs, we constructed disease trajectories in which diseases were represented as nodes and their interconnections as arrows preserving the predominant temporal sequence [15]. For example, an arrow from depression to alcohol use disorder indicates that depression diagnosis more commonly preceded the diagnosis of alcohol use disorder in the data and that a diagnosis of depression was associated with an increased subsequent risk of alcohol use disorder.
In the third part of the data analysis, we repeated the analyses on the associations between infections and incident dementia, additionally adjusting for any other dementia-related diseases. To minimise the risk of residual confounding, these additional adjustments included all noninfectious dementia-related diseases regardless of whether they were components of the disease trajectories leading to infections. We also assessed the associations of infections with dementia in subgroups defined by sex and education (tertiary or secondary [high] versus basic or no qualifications [low]). We conducted several sensitivity analyses to test the robustness of our findings; we 1) included additional adjustments for income and prior medication use, 2) excluded all controls who developed dementia after the index date, 3) used a year of birth, index year, and sex-adjusted mixed effects logistic regression model with random effects for area of residence instead of the conditional logistic regression used in the main analyses, 4) and used inverse-probability weighting to account for potential confounding by all the variables used in the most adjusted model (year of birth; index year; sex; education; marital status; employment; area of residence; income; medications for hypertension, diabetes, and coronary heart disease; noninfectious dementia-related diseases). We also conducted 5-year lag-analyses in which we ignored infections and other diseases that were diagnosed less than 5 years before dementia (or index date for controls).
From the adjusted analyses, we computed excess risk explained by comorbidities (ERE) as
Data were analysed using Stata MP 17 and 18. Statistical codes used in analysis are provided in S1 Stata Codes. Confidence intervals (CI) are reported at the 95% level. The analyses were based on a pre-specified analysis plan (S1 Study Plan). Amendments were later made to increase the comprehensiveness of disease identification (RR threshold changed from ≥ 1.50 to ≥ 1.20), to add analyses for early onset dementia, to add adjustments, to combine high and intermediate education in stratified analyses to gain power, and to add sensitivity analyses in response to peer review comments. This study is reported in accordance with the REporting of studies Conducted using Observational Routinely-collected health Data (RECORD) guideline (S1 RECORD Checklist).
Results
We identified 62,555 dementia cases and 312,772 control individuals matched for year of birth, sex, and follow-up period. The mean age was 81.0 (standard deviation [SD] 7.0) among both the cases and controls. 37,582 (60.1%) of the dementia cases were women, 37,042 (59.2%) had at most basic education, and 41,904 (67.0%) were married (Table 1). The corresponding numbers were 187,910 (60.1%), 177,825 (56.9%), and 217,375 (69.5%) among the controls.
Table 1: Characteristics of the study population in the main analyses of late-onset dementia.
In the first part of the analysis, we identified diseases robustly associated with incident dementia. Of the 170 diseases that preceded dementia with a prevalence of at least 1% during the 1–21-year exposure window, 59 showed statistically significant associations after Bonferroni correction for 170 tests (p < 0.000294, Fig 2). Of these, 29 had an RR of at least 1.20 for dementia (Fig 3). These included 9 injuries, 6 mental and behavioural disorders, 5 cardiovascular and 3 neurological diseases, 1 endocrine, 1 metabolic, 1 eye and 1 digestive disease, as well as 2 infections (cystitis [an infection of the genitourinary system] and bacterial infection of unspecified site). Overall, 29,376 (47.0%) of the 62,555 dementia cases had at least one of these diseases during the two-decade exposure period before dementia, and 12,896 (20.6%) had at least two (Table A in S1 Appendix). The most common were cerebral infarction (prevalence 9.6%), intracranial injury (6.0%), and type 2 diabetes mellitus (4.9%). Numbers of dementia cases and controls with infections by type of infection are shown in Table 2.
Table 2: Number of dementia cases and controls with dementia-related infections for late-onset dementia and early onset dementia.
Flow chart of disease selection.The figure shows the steps used to identify the 29 diseases robustly associated with incident dementia from 170 diseases with a prevalence of at least 1% before dementia. Abbreviation: RR, rate ratio.
Diseases associated with an increased risk of dementia.Rate ratios and p-values are based on incidence-density sampling and matched analysis (conditional logistic regression) and were adjusted for year of birth (matching variable), index date (matching variable), sex (matching variable), education, marital status, area of residence, and employment status. Abbreviations: CI, confidence interval; Other organic mental disorders, Other mental disorders due to brain damage and dysfunction and to physical disease. Abbreviation: RR, rate ratio.
The strongest associations with dementia were seen for mental disorders due to brain damage or physical disease (RR 3.76, 95% CI [3.48, 4.06]; p < 0.001), Parkinson’s disease (RR 3.24, 95% CI [3.06, 3.44]; p < 0.001), and alcohol-related mental and behavioural disorders (RR 1.87, 95% CI [1.76, 1.99]; p < 0.001) (Fig 3). The RRs between infections and dementia were lower: 1.22 (95% CI [1.17, 1.27]; p < 0.001) for cystitis and 1.21 (95% CI [1.16, 1.28]; p < 0.001) for bacterial infection of unspecified site. The diseases were diagnosed on average 4.7–11.8 years before dementia diagnosis, with depression diagnosed the earliest (mean 11.8 [SD 6.2] years before dementia) and organic mental disorder the latest (mean 4.7 [SD 3.8] years). Cystitis and bacterial infection of unspecified site occurred on average 6.5 (SD 5.0) years and 5.6 (SD 3.8) years before dementia, respectively.
In the second part of the analysis, we constructed disease trajectories from these 29 dementia-related diseases, forming 406 disease pairs. Considering the more commonly occurring temporal order in each disease pair, 153 pairs (37.7%) showed a RR ≥ 1.20 with a statistically significant p-value after Bonferroni correction (p < 0.00012). These were used to construct a network of disease trajectories. Fig 4 presents trajectories with particularly strong associations (RR ≥ 3.00); all 153 disease pairs are listed in the appendix (Table B in S1 Appendix). In supplementary analyses examining the less commonly occurring temporal order, 79 (19.5%) of the 406 pairs remained significant (RR ≥ 1.20, p < 0.00012) (Table C in S1 Appendix).
Associations between dementia-related diseases.The arrows indicate disease pairs in which the first-occurring diseases (tail of the arrow) is associated with a Bonferroni significant RR of at least 3.00 for the second-occurring disease (arrowhead). RRs and p-values are based on incidence-density sampling and matched analysis (conditional logistic regression) and were adjusted for year of birth (matching variable), index date (matching variable), sex (matching variable), education, marital status, area of residence, and employment status. Abbreviation: RR, rate ratio.
The third part of the analysis examined whether the associations between infections and dementia were explained by other dementia-related diseases. Of the 29 dementia-related diseases identified in the first part of the analysis, 19 (65.5%) were associated with an increased risk of cystitis (Fig 5), with the strongest associations for epilepsy (RR 2.69, 95% CI [2.02, 3.59]; p < 0.001), intracerebral haemorrhage (RR 2.69, 95% CI [1.88, 3.85]; p < 0.001), and alcohol-related mental and behavioural disorders (RR 2.61, 95% CI 1.93, 3.54]; p < 0.001). Ten diseases (34.5%) were associated with bacterial infections of unspecified site (Fig 6), most strongly other fluid, electrolyte and acid-base balance disorders (RR 2.57, 95% CI [1.95, 3.40]; p < 0.001), retinal disorders in diseases classified elsewhere (RR 2.46, 95% CI [1.70, 3.58]; p < 0.001), and alcohol-related mental and behavioural disorders (RR 2.30, 95% CI [1.77, 2.99]; p < 0.001).
Diseases associated with an increased risk of cystitis.The arrows indicate disease pairs in which the first-occurring diseases (tail of the arrow) are associated with a Bonferroni significant RR of at least 1.20 for cystitis (arrowhead). RRs and p-values are based on incidence-density sampling and matched analysis (conditional logistic regression) and were adjusted for year of birth (matching variable), index date (matching variable), sex (matching variable), education, marital status, area of residence, and employment status. Abbreviations: CI, confidence interval; RR, rate ratio.
Diseases associated with an increased risk of bacterial infection of an unspecified site.The arrows indicate disease pairs in which the first-occurring diseases (tail of the arrow) are associated with a Bonferroni significant RR of at least 1.20 for bacterial infection of an unspecified site (arrowhead). RRs and p-values are based on incidence-density sampling and matched analysis (conditional logistic regression) and were adjusted for year of birth (matching variable), index date (matching variable), sex (matching variable), education, marital status, area of residence, and employment status. Abbreviations: CI, confidence interval; RR, rate ratio.
The associations of infections with dementia risk remained robust after adjustment for all prior noninfectious dementia-related diseases. After these adjustments, the RR was 1.19 (95% CI [1.14, 1.24]; p < 0.001) for cystitis and 1.19 (95% CI [1.13, 1.25]; p < 0.001) for bacterial infections of unspecified site. Only 10.8% to 13.8% of the excess dementia risk among individuals with these infections was attributable to comorbidities. The findings were consistent across sex and education strata (Fig 7) and in all sensitivity analyses (Fig A in S1 Appendix). In lag-analyses for cystitis and bacterial infections of unspecified site, the associations with dementia attenuated but remained statistically significant (Fig B in S1 Appendix).
Association of infectious diseases with the risk of dementia in the whole study sample and in subsamples stratified by sex and education.Rate ratios and p-values are based on incidence-density sampling and matched analysis (conditional logistic regression) and were adjusted for year of birth (matching variable), index date (matching variable), sex (matching variable), education, marital status, area of residence, and employment status. Analyses stratified by education were not adjusted for education. Additionally, adjusted models were also adjusted for all noninfectious dementia-related diseases identified in this study. Abbreviations: CI, confidence interval; ERE, excess risk explained by comorbidities; RR, rate ratio.
In additional analyses, we considered early onset dementia (diagnosed before age 65). We identified 2,639 cases (mean age 57.5 [SD 5.2], 1,264 [47.9%] women) with early onset dementia and 13,195 control individuals (mean age 57.5 [SD 5.2], 6,320 [47.9%] women) matched for year of birth, sex, and follow-up period (Table D in S1 Appendix). Using a similar stepwise procedure than in the main analysis, we found that after Bonferroni correction for multiple testing (162 tested diseases, P < 0.000309), 42 diseases were associated with a RR of at least 1.20 for early onset dementia (Fig 8). 1,665 (63.1%) of the 2,639 cases with early onset dementia had at least one of these diseases during the two-decade exposure period before dementia (Table E in S1 Appendix). Strongest associations with early onset dementia were seen for Parkinson’s disease (RR 31.88, 95% CI [19.50, 52.11]; p < 0.001), sequalae of injuries of head (RR 10.23, 95% CI [6.17, 16.97]; p < 0.001), and other mental disorders due to brain damage and dysfunction and to physical disease (RR 10.11, 95% CI [6.37, 16.03]; p < 0.001).
Diseases associated with an increased risk of early onset dementia.Rate ratios and p-values are based on incidence-density sampling and matched analysis (conditional logistic regression) and were adjusted for year of birth (matching variable), index date (matching variable), sex (matching variable), education, marital status, area of residence, and employment status. Abbreviations: CI, confidence interval; Other organic mental disorders, Other mental disorders due to brain damage and dysfunction and to physical disease; RR, rate ratio.
Of infections, other gastroenteritis and colitis of infectious and unspecified origin had a RR of 1.88 (95% CI [1.48, 2.39]; p < 0.001), bacterial infection of unspecified site had a RR of 2.24 (95% CI [1.64, 3.06]; p < 0.001), bacterial pneumonia, not elsewhere classified a RR of 1.75 (95% CI [1.31, 2.34]; p < 0.001), pneumonia, organism unspecified a RR of 1.82 (95% CI [1.50, 2.19]; p < 0.001), and dental caries a RR of 2.20 (95% CI [1.59, 3.03]; p < 0.001) for early onset dementia. The associations of these infections with an increased risk of early onset dementia remained after adjustment for all prior noninfectious early onset dementia-related diseases (Fig 9). Of the excess risk of early onset dementia among individuals with these infections, 8.8% to 32.8% was attributable to comorbidities.
Infectious diseases associated with an increased risk of early onset dementia.Rate ratios and p-values are based on incidence-density sampling and matched analysis (conditional logistic regression) and were adjusted for year of birth (matching variable), index date (matching variable), sex (matching variable), education, marital status, area of residence, and employment status. Additionally, adjusted models were also adjusted for all noninfectious early onset dementia-related diseases identified in this study. Abbreviations: CI, confidence interval; ERE, excess risk explained by comorbidities; RR, rate ratio.
Discussion
In this analysis of electronic health records from nationwide registries, we examined 170 physical and mental diseases among more than 60,000 cases of late-onset dementia (age 65+) and over 300,000 matched controls. We identified 29 diseases that were robustly associated with an increased risk of dementia and identified disease trajectories in which the onset of one condition elevated the risk of developing another. Two of these diseases were severe infections––hospital-treated cystitis and bacterial infections of unspecified site––typically occurring late in the disease trajectories. Consequently, many other dementia-related diseases were also associated with an increased risk of these infections. However, as less than one-seventh of the excess dementia risk among individuals with hospital-treated cystitis or bacterial infections of unspecified site was attributable to comorbidities, the present study suggests that the associations between these infections and dementia are largely independent of prior conditions and thus supports the idea that severe infections are risk factors for dementia.
During the past few years, considerable research interest has focussed on the potential role of infectious diseases in the development of dementia [1–6,30–32]. Pre-existing comorbid conditions are potentially important contributors to this association, because the average age of dementia diagnosis is older than 80 years, and therefore people with dementia often have other illnesses [12,13], many of which also confer an increased risk for infections [16–18]. Supporting this reasoning, we found that of the 29 diseases associated with an increased risk of dementia, two-thirds were also linked to an increased risk of cystitis, and one third to an increased risk of bacterial infections of unspecified site. These included known infection risk factors, such as type 2 diabetes, alcohol abuse, cerebral infarction, Parkinson’s disease, epilepsy, and traumatic brain injury [16,17,19,20]. However, they also included conditions that are not typically considered risk factors for infections, such as nonbrain injuries and depression.
The modest contribution of pre-existing conditions to the association between infections and dementia supports the hypothesis that severe infections may directly influence dementia risk. In our study, the average time difference between infection diagnosis and dementia was relatively short, 5–6 years. This time frame suggests that the inflammatory insult resulting from infections severe enough to require hospital treatment may accelerate pre-existing preclinical stage of dementia rather than initiate neurodegeneration in a cognitively healthy person [31,33,34].
Evidence from cohort studies and natural experiments indicates that vaccination against infectious diseases might be an effective strategy for reducing or postponing the onset of dementia [35–38]. In these natural experiments, herpes zoster vaccination reduced dementia risk more effectively among women than men [37,38]. Conversely, in our data focussed on other infections, cystitis and bacterial infections of unspecified site both had slightly stronger associations with dementia among men. Urinary tract and bacterial infections are common infectious diseases that have been associated with increased dementia risk in several prospective studies [3–6,32], but findings stratified by sex have been mixed. In a large British study, the association between urinary tract infections and dementia was stronger among men [3], but in a large New Zealand study the association between bacterial infections and dementia was stronger among women [5]. Also, somewhat surprisingly, in our study, the associations of these infections with dementia were stronger among those with high education compared to those with low education. We speculate that the relative contribution of infections on dementia risk might be stronger among highly educated individuals because they have a lower prevalence of other dementia risk factors [39]. Consistent with previous findings, infections showed stronger associations with early onset than with late-onset dementia and we identified more dementia-associated infections in early onset dementia [4]. The mechanisms underlying these differences are unclear, but it is well-established that early and late-onset dementia differ in aetiology and genetic susceptibility [40,41].
As pertains to noninfectious diseases, our findings agree with previous studies suggesting increased risk of dementia among individuals with Parkinson’s disease, mental and behavioural disorders due to use of alcohol, epilepsy, intracranial injury, ischaemic and haemorrhagic stroke, depression, type 2 diabetes, or retinal disorders in diseases including diabetic retinopathy [42–51]. In contrast, evidence on the status of anxiety as a risk factor remains mixed [52–54]. Among the dementia-related diseases identified in our study, several were related to fractures and other injuries. Increased vulnerability to accidents may result from nervous system deterioration, frailty, or, in some cases, harmful alcohol use [55–59]. Additionally, head injuries are often accompanied by brain trauma [60,61].
We also found that disorders of the fluid, electrolyte and acid-base balance were associated with an increased risk of dementia. These disorders can indicate poor overall health and may also have direct adverse effects on brain health [62–68]. Furthermore, the disease trajectories formed by dementia-related conditions suggest that the cumulative burden of multiple diseases may contribute to dementia risk.
Our study has some important strengths. Combined with correction for multiple testing, the large sample drawn from the total population of Finland provides good statistical power and stable estimates, making chance findings unlikely. Our hypothesis-free approach, estimating associations of dementia with all nonrare diseases (prevalence ≥ 1%) recorded during a 20-year time window before dementia diagnosis, is also a strength, allowing us to identify all relevant diseases regardless of whether their importance has previously been appreciated. The register-based data do not suffer from self-report biases.
Our study also has some important limitations. As this is a population-wide register-based study, baseline cognitive assessments and clinical examination data leading to dementia and other disease diagnoses were not available. However, previous evidence indicates that electronic health record-based diagnoses have acceptable validity for examining disease risk factors; the Finnish Care Register for Health Care includes over 95% of all hospital discharges in Finland with high positive predictive values ranging from 75% to 99% for common diagnoses [69]. We assumed that all study individuals remained covered by the Finnish healthcare system throughout the observation period, thereby ignoring any bias arising from individuals who emigrated from Finland. However, this bias is unlikely to be major, as emigration among Finnish citizens aged 65 years and older is rare—~0.05% annually [21]. Infections were treated in hospitals, but no data on specific treatments were available from the electronic health records. We examined all-cause dementia as the outcome. Future work should investigate dementia subtypes, given that severe infections may be more strongly linked to vascular dementia than to Alzheimer’s disease [1,3]. We may have missed some true associations because we analysed each 3-digit diagnostic code separately, ignoring partial overlap between codes, and applied Bonferroni correction for multiple testing, which may be overly conservative when tests (i.e., diseases) are not fully independent. To reduce bias from delays in the recording of dementia in the registers, we used a 1-year gap in analyses, excluding any diagnoses recorded within 1 year before dementia diagnosis. Some dementia cases may have been misclassified as controls owing to delayed dementia diagnosis; this would likely attenuate the observed associations. Given the long preclinical phase of dementia, part of the observed associations might reflect preclinical dementia increasing susceptibility to infectious and other diseases, rather than the reverse, potentially leading to an overestimation of associations. We observed attenuation of the associations in lag-analyses, suggesting that reverse causation might be present or that severe infections may accelerate existing cognitive decline and neuropathological processes [33,34]. Furthermore, although we had access to relevant demographic data such as age, sex, education, employment, marital status, and area of residence, our data lacked information about other possibly relevant covariates such as smoking status and apolipoprotein E genotype. Nondisease events, such as symptoms without a specific diagnosis, were outside the scope of the study, but might still contribute to dementia risk [54].
In conclusion, findings from this nationwide population-based Finnish study indicate that multiple interconnected diseases are associated with an increased risk of dementia. Among them, severe infections, despite their relationships to several other dementia-related diseases, were independently associated with an increased dementia incidence. Overall, our findings support the possibility that severe infections increase dementia risk; however, intervention studies are required to establish whether preventing or effectively treating infections yields benefits for dementia prevention.
Supporting information
S1 Study PlanPre-specified study plan.(PDF)
S1 RECORD ChecklistThe Reporting of Studies Conducted using Observational Routinely-Collected Data (RECORD) guideline checklist.The checklist is protected under Creative Commons Attribution (CC BY) license.(PDF)
S1 AppendixSupplementary tables and figures.(XLSX)
S1 Stata CodesStatistical codes used in analysis.(TXT)
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1SipiläPN, HeikkiläN, Lindbohm JV, Hakulinen C, Vahtera J, Elovainio M, et al. Hospital-treated infectious diseases and the risk of dementia: a large, multicohort, observational study with a replication cohort. Lancet Infect Dis. 2021;21(11):1557–67. doi: 10.1016/S 1473-3099(21)00144-4 34166620 PMC 8592915 · doi ↗ · pubmed ↗
- 2Muzambi R, Bhaskaran K, Brayne C, Davidson JA, Smeeth L, Warren-Gash C. Common bacterial infections and risk of dementia or cognitive decline: a systematic review. J Alzheimers Dis. 2020;76(4):1609–26. doi: 10.3233/JAD-200303 32651320 PMC 7504996 · doi ↗ · pubmed ↗
- 3Muzambi R, Bhaskaran K, Smeeth L, Brayne C, Chaturvedi N, Warren-Gash C. Assessment of common infections and incident dementia using UK primary and secondary care data: a historical cohort study. Lancet Healthy Longev. 2021;2(7):e 426–35. doi: 10.1016/S 2666-7568(21)00118-5 34240064 PMC 8245326 · doi ↗ · pubmed ↗
- 4Sun J, Ludvigsson JF, Ingre C, Piehl F, Wirdefeldt K, Zagai U, et al. Hospital-treated infections in early- and mid-life and risk of Alzheimer’s disease, Parkinson’s disease, and amyotrophic lateral sclerosis: a nationwide nested case-control study in Sweden. P Lo S Med. 2022;19(9):e 1004092. doi: 10.1371/journal.pmed.1004092 36107840 PMC 9477309 · doi ↗ · pubmed ↗
- 5Richmond-Rakerd LS, Iyer MT, D’Souza S, Khalifeh L, Caspi A, Moffitt TE, et al. Associations of hospital-treated infections with subsequent dementia: nationwide 30-year analysis. Nat Aging. 2024;4(6):783–90. doi: 10.1038/s 43587-024-00621-3 38714911 PMC 12713650 · doi ↗ · pubmed ↗
- 6Mawanda F, Wallace RB, Mc Coy K, Abrams TE. Systemic and localized extra-central nervous system bacterial infections and the risk of dementia among US veterans: a retrospective cohort study. Alzheimers Dement (Amst). 2016;4:109–17. doi: 10.1016/j.dadm.2016.08.004 27752534 PMC 5061465 · doi ↗ · pubmed ↗
- 7Bettcher BM, Tansey MG, Dorothée G, Heneka MT. Peripheral and central immune system crosstalk in Alzheimer disease - a research prospectus. Nat Rev Neurol. 2021;17(11):689–701. doi: 10.1038/s 41582-021-00549-x 34522039 PMC 8439173 · doi ↗ · pubmed ↗
- 8Walker KA, Le Page LM, Terrando N, Duggan MR, Heneka MT, Bettcher BM. The role of peripheral inflammatory insults in Alzheimer’s disease: a review and research roadmap. Mol Neurodegener. 2023;18(1):37. doi: 10.1186/s 13024-023-00627-2 37277738 PMC 10240487 · doi ↗ · pubmed ↗