Distinct neuroinflammatory profiles in progressive supranuclear palsy associated with HLA haplotypes
Shelley L Forrest, Sarah S Zaheer, Ain Kim, Hidetomo Tanaka, Helen Chasiotis, Jun Li, Susan H Fox, Jinguo Wang, M Carmela Tartaglia, Anthony E Lang, Gabor G Kovacs

TL;DR
This study shows that different HLA gene variations are linked to unique immune and brain changes in a type of brain disease called progressive supranuclear palsy.
Contribution
The study identifies distinct neuroinflammatory profiles associated with specific HLA haplotypes in progressive supranuclear palsy.
Findings
HLA haplotypes correlate with differences in microglia, T cells, and p-Tau pathology in progressive supranuclear palsy.
Machine learning identified specific neuroinflammatory marker ratios that distinguish HLA-defined groups.
Symptom progression sequences vary by HLA haplotype, suggesting a role of immune profiles in disease trajectory.
Abstract
Progressive supranuclear palsy is a neurodegenerative four-repeat tauopathy characterized by atypical parkinsonism and cognitive behavioural changes and a relatively uniform neuropathology. Building on prior identification of rare HLA (human leukocyte antigen) haplotypes in progressive supranuclear palsy, this study investigates whether these haplotypes correlate with distinct clinical and immunopathological phenotypes. In addition to retrospective collection of clinical data, we evaluated T and B cells, microglia and phosphorylated-tau (p-Tau) cytopathologies in 32 progressive supranuclear palsy cases. Machine learning was used to analyse whether pathological variables and their ratios, or the sequence of clinical symptoms are different HLA-defined groups, including one linked to narcolepsy (DRB1*15:01-DQB1*06:02). Neuropathology revealed regional differences in the severity of…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1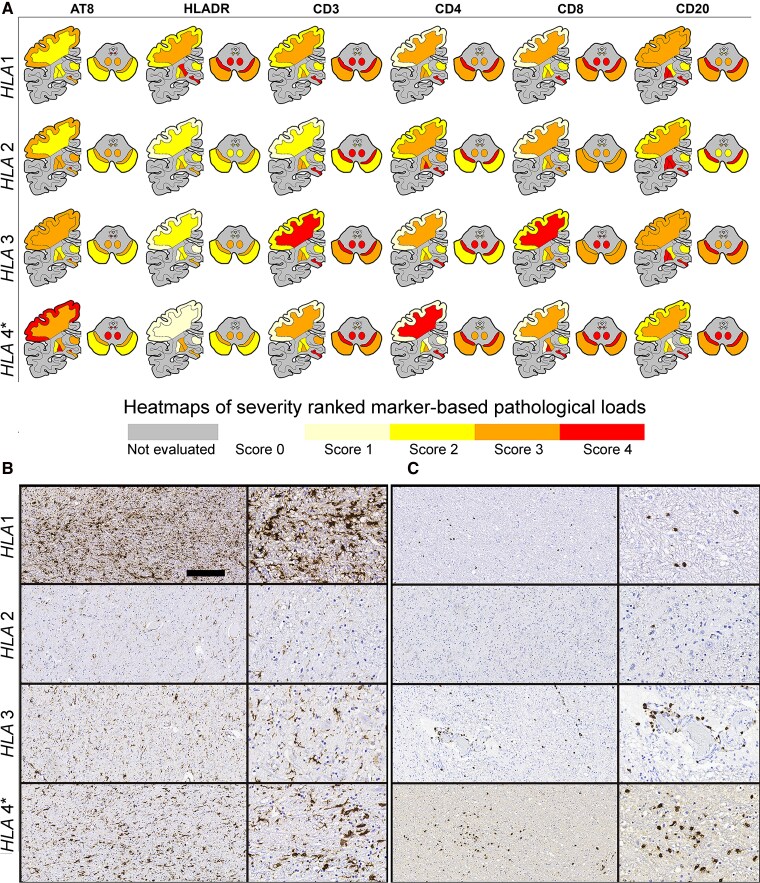 Figure 2
Figure 2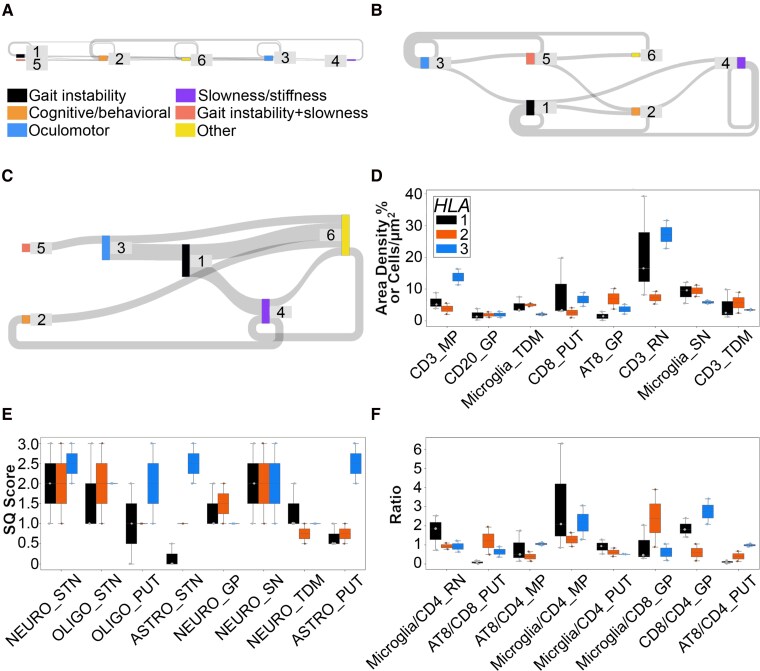 Figure 3
Figure 3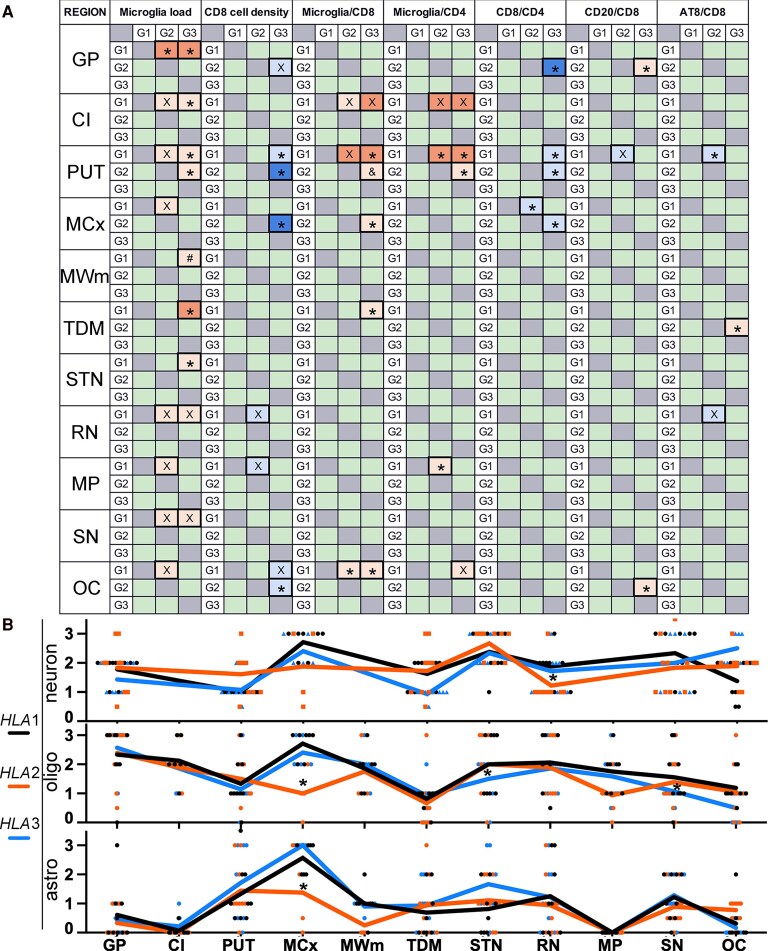 Figure 4
Figure 4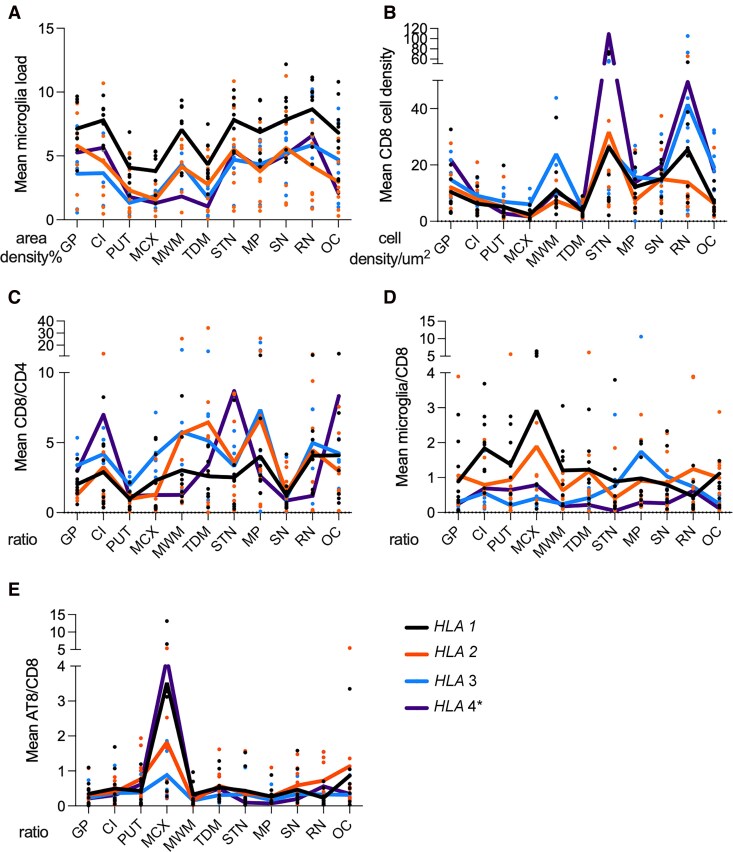 Figure 5
Figure 5- —Rossy Family Foundation
- —National Institute on Aging10.13039/100000049
- —National Institutes of Health10.13039/100000002
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsParkinson's Disease Mechanisms and Treatments · Genetic Neurodegenerative Diseases · Alzheimer's disease research and treatments
Introduction
Progressive supranuclear palsy is a neurodegenerative four-repeat (4R) tauopathy associated with the accumulation of phosphorylated-tau (p-tau) in neurons, oligodendrocytes and astrocytes.^1^ Progressive supranuclear palsy is considered a homogeneous disorder based on hallmark neuropathological features^1^ and similar filament structure of misfolded tau reported in six progressive supranuclear palsy cases examined to date.^2^ However, clinical phenotypes associated with progressive supranuclear palsy pathology vary and include syndromes in the spectrum of atypical parkinsonism and cognitive behavioural changes.^3^ Clinical variability is associated with differences in the distribution patterns of p-tau cytopathologies^4^ and in cases with Richardson syndrome, a six-tiered neuropathological staging system was introduced.^4^
Traditionally, neurodegenerative diseases are defined by neuronal loss not explained by infection, neoplasia or toxins.^5^ However, neuroinflammation, defined as microglial and astrocytic activation and leukocyte infiltration, is increasingly recognized as a key component in disease progression and therapeutic targeting.^6^ Progressive supranuclear palsy-type pathology overlaps with some neuropathological features described in IgLON5 autoimmune encephalitis-related tauopathy^7^ and the 3R and 4R tauopathy, postencephalitic parkinsonism.^8^ Interestingly, recent studies using immunostainings for lymphocytes have shown that CD8 cytotoxic T cells are consistently present in the midbrain in progressive supranuclear palsy and are more prominent than observed in other neurogenerative parkinsonisms.^9,10^ These autopsy studies were complemented by bodily fluid studies such as cytokine profiles^11,12^ or shift in peripheral CD4- and CD8-positive T-cell populations.^12^
Despite these insights, variability in neuroinflammatory markers across progressive supranuclear palsy cases remains unexplained. Given the role of the human leukocyte antigen (HLA) locus in autoimmune diseases,^13^ we hypothesized that HLA haplotypes might be associated with distinct neuroinflammatory responses in progressive supranuclear palsy. Our recent study identified the DRB115:01-DQB106:02 haplotype and DQB1*06:01/06:02 alleles as strongly associated with progressive supranuclear palsy.^14^ In the present study, we mapped p-tau pathology and inflammatory markers in progressive supranuclear palsy brains stratified by HLA haplotype to explore our hypothesis.
Material and methods
Clinical information
Clinical data was analysed from a cohort of 32 patients clinically diagnosed with progressive supranuclear palsy, comprising 11 retrospective cases and 21 prospective cases obtained from the Rossy PSP Centre at the University Health Network (UHN). Demographic variables included sex and age at death. Disease duration was calculated from the time of onset of the first reported symptom to the time of death. We focused on symptoms explicitly documented in the clinical records; for details, see online Supplementary file Methods.
Neuropathology and immunohistochemistry
The brain autopsy tissue was collected with informed consent according to the Declaration of Helsinki and with approval from the UHN Research Ethics Board (Protocol Nr. 20-5258). A systematic neuropathological examination was conducted following established diagnostic criteria, including assessment of vascular pathology.^15-17^ For all cases, HLA genotyping was available as reported.^14^ To evaluate inflammatory markers, we focused on brain regions typically affected in early to moderate stages of progressive supranuclear palsy; details on these and on antibodies and procedures used for digital pathology and morphometry analysis are provided in the online Supplementary file Methods and Tables S1 and S2 and Figs. S1–S3.
Statistical analysis
Chi^2^ test was used to compare the frequency of presenting clinical symptoms and the level of vascular pathology using the vascular cognitive impairment neuropathology guidelines (VCING).^17^ Kruskal–Wallis and Mann–Whitney U tests were performed to compare total p-tau load; microglia load and CD8, CD4, CD3 and CD20 cell densities; semiquantitative p-tau cytopathology scores; grades of small vessel pathology; ratios of neuropathological variables; duration of illness; and age at death between groups and between regions in the same groups. The Spearman correlation test was used to compare the association between pathological variables, duration of illness and age at death. To correct for the effect of progressive supranuclear palsy neuropathological stage,^4^ Alzheimer’s disease neuropathologic change (ADNC) level,^18^ Lewy body disease (LDB) stage,^19^ duration of illness and age at death on the differences between groups, we used the non-parametric analysis of covariance (ANCOVA) and linear regression for cases with progressive supranuclear palsy stage ≥3.
Machine learning analysis
Four separate datasets were analysed: quantification of inflammatory marker-based pathology, cytopathology, sequence of clinical symptoms and the ratios of the inflammatory marker-based pathology. For all datasets except the sequence of clinical symptoms, permutation importance and treeSHapley Additive exPlanations (SHAP) were analysed following random forest classifier with train-test split on normalized, raw data; for details see online Supplementary file Methods.
Supplementary Material
fcag084_Supplementary_Data
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Roemer SF, Grinberg LT, Crary JF, et al Rainwater Charitable Foundation criteria for the neuropathologic diagnosis of progressive supranuclear palsy. Acta Neuropathol. 2022;144(4):603–614.35947184 10.1007/s 00401-022-02479-4PMC 9468104 · doi ↗ · pubmed ↗
- 2Shi Y, Zhang W, Yang Y, et al Structure-based classification of tauopathies. Nature. 2021;598(7880):359–363.34588692 10.1038/s 41586-021-03911-7PMC 7611841 · doi ↗ · pubmed ↗
- 3Höglinger GU, Respondek G, Stamelou M, et al Clinical diagnosis of progressive supranuclear palsy: The movement disorder society criteria. Mov Disord. 2017;32(6):853–864.28467028 10.1002/mds.26987 PMC 5516529 · doi ↗ · pubmed ↗
- 4Kovacs GG, Lukic MJ, Irwin DJ, et al Distribution patterns of tau pathology in progressive supranuclear palsy. Acta Neuropathol. 2020;140(2):99–119.32383020 10.1007/s 00401-020-02158-2PMC 7360645 · doi ↗ · pubmed ↗
- 5Forrest SL, Kovacs GG. Current concepts and molecular pathology of neurodegenerative diseases. Pathology. 2025;57(2):178–190.39672768 10.1016/j.pathol.2024.10.006 · doi ↗ · pubmed ↗
- 6Shi FD, Yong VW. Neuroinflammation across neurological diseases. Science. 2025;388(6753):eadx 0043.40536983 10.1126/science.adx 0043 · doi ↗ · pubmed ↗
- 7Gelpi E, Reinecke R, Gaig C, et al Neuropathological spectrum of anti-Ig LON 5 disease and stages of brainstem tau pathology: Updated neuropathological research criteria of the disease-related tauopathy. Acta Neuropathol. 2024;148(1):53.39400557 10.1007/s 00401-024-02805-y PMC 11473580 · doi ↗ · pubmed ↗
- 8Jellinger KA . Absence of alpha-synuclein pathology in postencephalitic parkinsonism. Acta Neuropathol. 2009;118(3):371–379.19404653 10.1007/s 00401-009-0537-9 · doi ↗ · pubmed ↗