Severe paravalvular detachment of a bioprosthetic aortic valve in atypical infective endocarditis
David Füller, Oliver Ritter, Vadim Tchaikovski

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
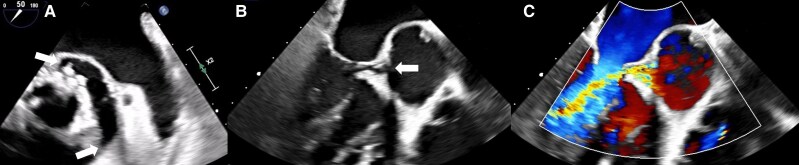 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsInfective Endocarditis Diagnosis and Management · Infectious Aortic and Vascular Conditions · Orthopedic Infections and Treatments
Case description
A 68-year-old man, 16 years after biological aortic valve replacement, presented in the Emergency Department with progressive exertional dyspnoea, currently on minimal exertion (NYHA III), and progressive lower leg oedema since 1 week. Prior to recent events, the patient has been in good functional status. He has just returned from a trip to Hawaii. N-terminal proBNP was significantly elevated (3926 pg/mL, reference value <125 pg/mL). C-reactive protein was moderately elevated (36.5 mg/L, reference value <5 mg/L). Transthoracic echocardiography revealed at least moderate aortic valve prosthesis insufficiency with a large eccentric insufficiency jet.
Transthoracic and transoesophageal echocardiography confirmed an extremely hypermobile prosthesis with detachment of about 120° of its circumference (Figure 1A and B) and hypermobility of about 50–60° (see Supplementary material online, Video S1), leading to severe paravalvular insufficiency (Figure 1C; Supplementary material online, Video S2). The patient was transferred for urgent replacement of the valve prosthesis.
(A) Severe paravalvular detachment of about 120° of the circumference of the bioprosthetic aortic valve, short axis. (B) Valve dehiscence, three-chamber view, long axis. (C) Severe paravalvular insufficiency, colour Doppler, three-chamber view, long axis.
Intraoperative findings confirmed endocarditis. Multiple blood cultures have remained negative. Polymerase chain reaction on intraoperative tissue samples identified Cutibacterium acnes, a relatively rare cause of endocarditis in general (approximately 3%), predominantly affecting men and prosthetic valve recipients.^1^ Its clinical presentation often involves mild or even absent inflammatory signs and negative blood cultures.^2^ C. acnes is an anaerobic Gram-positive bacterium. It is the most abundant bacterium of the human skin microbiome since adolescence, participating in skin homeostasis, but it can act as an opportunistic pathogen. An important virulence factor is the formation of a biofilm. Late-onset bioprosthetic valve endocarditis from C. acnes 5 years after composite aortic root and valve replacement has previously been reported by others,^3^ but no case of as long as 16 years between bioprosthetic valve implantation and endocarditis has been reported in the literature. This case also highlights a rare differential diagnosis for pulmonary embolism for a patient presenting with acute-onset dyspnoea following a long-haul flight.
Supplementary Material
ytag182_Supplementary_Data
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Saha S, Joskowiak D, Marin-Cuartas M, De La Cuesta M, Weber C, Luehr M, et al Cutibacterium acnes infective endocarditis-an emerging pathogen. Eur J Cardiothorac Surg 2024;66:ezae 422.39585651 10.1093/ejcts/ezae 422 · doi ↗ · pubmed ↗
- 2Heinen FJ, Arregle F, van den Brink FS, Marsan NA, Bernts L, Houthuizen P, et al Clinical characteristics and outcomes of patients with Cutibacterium acnes endocarditis. JAMA Netw Open 2023;6:e 2323112.37436747 10.1001/jamanetworkopen.2023.23112 PMC 10339155 · doi ↗ · pubmed ↗
- 3Velollari O, Reinhardt CM, Knorr M, Schnitzler K, Graafen D, Miederer M, et al Late-onset prosthetic endocarditis with paraaortic abscess caused by cutibacterium acnes. Infect Dis Rep 2023;15:635–641.37888140 10.3390/idr 15050059 PMC 10606402 · doi ↗ · pubmed ↗