Complex hybrid management of severe aortic stenosis and aortic arch disease in a nonagenarian: a case report
Mirko Muretti, Maria Antonella Ruffino, Giovanni Pedrazzini, Stefanos Demertzis, Enrico Ferrari

TL;DR
A 90-year-old man with severe aortic issues underwent a complex hybrid procedure that reduced surgical risks compared to traditional open surgery.
Contribution
A successful hybrid approach combining transcatheter and surgical techniques for complex aortic disease in a nonagenarian is presented.
Findings
The hybrid procedure was performed safely in a 90-year-old with aortic arch dilatation and severe aortic stenosis.
The patient had an uneventful recovery and was discharged 15 days post-surgery.
Hybrid approaches may reduce risks compared to conventional open surgery in high-risk nonagenarians.
Abstract
Nonagenarians represent a cohort of patients at high or prohibitive risk in case of complex aortic procedures. A hybrid approach could reduce the surgical risk compared with a conventional surgery when performed at the age of 90. We reported the case of a 90-year-old man who presented with a progressive aortic arch dilatation due to a persistent type-1A endoleak following previous thoracic endovascular aortic repair due to type-B aortic dissection. The aortic computed tomography scan confirmed a 65 × 67 mm aortic arch dilatation due to a type-1A endoleak and a transthoracic echocardiogram showed a severe aortic valve stenosis. On full sternotomy and partial cardiopulmonary bypass assistance, the patient underwent transcatheter aortic valve replacement combined with surgical brachiocephalic trunk and left common carotid artery debranching and thoracic endovascular aortic repair of the…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
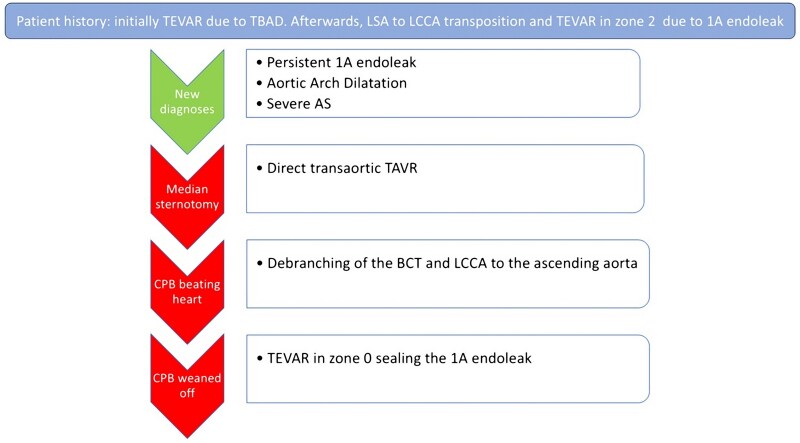 Figure 1
Figure 1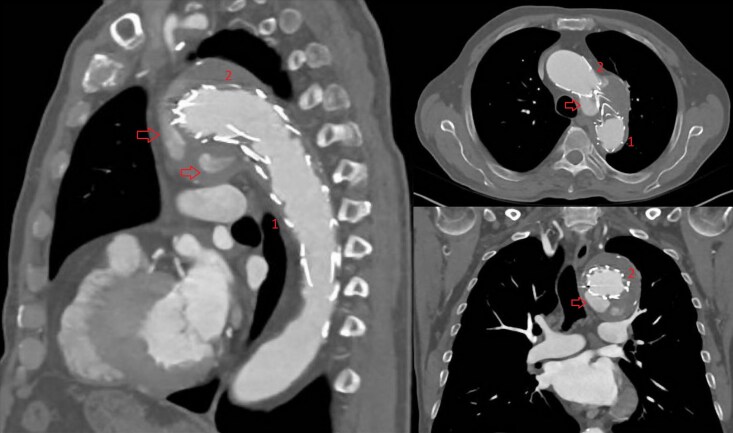 Figure 1
Figure 1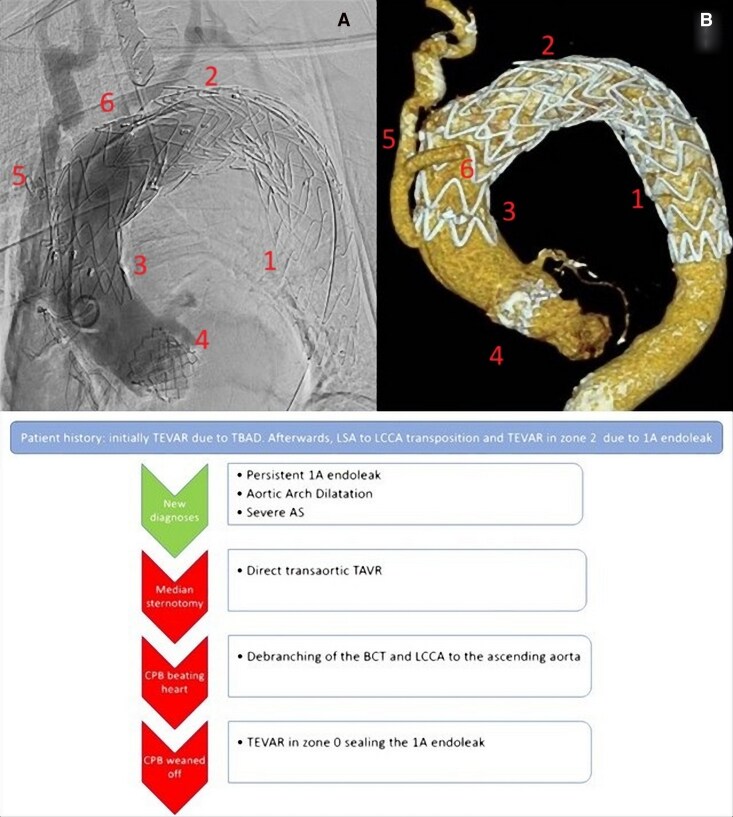 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAortic Disease and Treatment Approaches · Tracheal and airway disorders · Congenital Heart Disease Studies
Introduction
The number of nonagenarians is constantly growing and they represent a cohort of patients at high or prohibitive risk in case of complex aortic procedures. The use of combined transcatheter and surgical techniques can help reducing the surgical risk and postoperative complications.
Summary figure
**
Case presentation
We describe a case of a 90-year-old man admitted with a diagnosis of severe aortic stenosis and persistent type-1A endoleak post-thoracic endovascular aortic repair (TEVAR). Previously, the patient underwent TEVAR due to a complicated type-B aortic dissection (Medtronic Valiant Captivia 36 × 32 × 150 mm). Afterwards, he experienced a type-1A endoleak and progressive dilatation of the proximal descending thoracic aorta. Therefore, he was scheduled for concomitant left-subclavian to the left-carotid artery transposition and TEVAR. A Medtronic Valiant Captivia 38 × 38 × 100 mm endoprosthesis was implanted with the proximal landing zone in zone 2. Unfortunately, a persistent type-1A endoleak was associated with a further dilatation of the aortic arch. A computed tomography (CT) scan showed a dilated aortic arch of 65 × 67 mm diameter (Figure 1). In addition, a known aortic valve stenosis progressed until a severe degree. A pre-operative transthoracic echocardiogram showed a normal functioning left ventricle with mild hypertrophy, calcified tricuspid aortic valve with aortic valve area at 0.94 cm^2^ and mean gradient at 39 mmHg, ascending aorta at 37 mm diameter. Considering the age of the patient and his comorbidities (Euroscore II 13.70%), after discussion in a multidisciplinary meeting, it was agreed for a hybrid approach combining a transcatheter aortic valve replacement (TAVR) with a brachiocephalic trunk and left common carotid artery debranching and TEVAR of the ascending aorta and arch.
CT-scan showing a dilated aortic arch 65 × 67 mm due to persistent type 1A endoleak in zone 2, arrows. First TEVAR Medtronic Valiant Captivia 36 × 32 × 150 mm with proximal landing in zone 3, number 1; Second TEVAR Medtronic Valiant Captivia 38 × 38 × 100 mm with proximal landing in zone 2, number 2.
A median sternotomy was performed and the cardiopulmonary bypass (CPB) was instituted through the right-subclavian artery and the right atrium. A direct transaortic TAVR was performed with a 26 mm Sapiens 3 Ultra. Then, a debranching of the brachiocephalic trunk and the left common carotid artery was performed under CPB assistance on a beating heart. A side clamp was applied at the ascending aorta and the anastomosis of a 10 mm vascular prosthesis was performed with Prolene 4-0. An end-to-end anastomosis of a 8 mm vascular prosthesis to the left common carotid artery was performed with Prolene 4-0. Then, an end-to-side anastomosis of the 8 mm to the 10 mm vascular prosthesis was performed with Prolene 4-0. Finally, an end-to-end anastomosis of the 10 mm vascular graft was performed to the brachiocephalic trunk. The CPB was weaned and the arterial and venous cannula removed. The procedure was completed performing a TEVAR through the right common femoral artery. An endoprosthesis, Medtronic Captivia 40 × 40 × 200 mm, was delivered in the arch landing in zone 0 and overlapped with the previous endoprosthesis in zone 2 in order to seal the type-1A endoleak achieving a good angiographic result (Figure 2A).
(A) angiography and (B) CT-scan 3D reconstruction post procedure and below a diagram with a step by step procedure description; 1: first TEVAR landing in zone 3; 2: second TEVAR landing in zone 2; 3: third TEVAR landing in zone 0; 4: TAVR; 5: 10 mm vascular prosthesis from the ascending aorta to the brachiocephalic trunk; 6: 8 mm vascular prosthesis from the previous 10 mm prosthesis to the left common carotid artery.
The postoperative recovery was uneventful and the patient was discharged to an inpatient rehabilitation facility at postoperative day 15. A pre-discharge CT scan confirmed the successful procedure without residual endoleak (Figure 2B).
Discussion
Complex aortic surgery carries higher operative risk when performed in nonagenarians and evidence in literature is scarce and based on case reports or small series. A recent multicentre retrospective observational study identified 18 nonagenarians who underwent valve surgery, CABG or a combination of them via a median sternotomy over an 8-year period. The median EuroSCORE-II predicted in-hospital mortality was 6.1% and at 6 months after surgery all patients were alive showing that a multidisciplinary patient selection and dedicated peri-operative care can lead to acceptable outcomes.^1^ Nasso et al. compared their results operating on nonagenarians with ‘open’ cardiac surgery (‘on’ or ‘off’ pump for coronary surgery; conventional or minimally invasive for valve surgery) from 2009 to 2021 (101 patients) and from 1998 to 2008 (127 patients). Their 30-day mortality improved from 13.4% to 5.9% in the more recent cohort of patients demonstrating acceptable risks in elderly patients.^2^ Elsisy et al. operated on 134 patients at 90 years of age or older that underwent isolated CABG, combined CABG and valve replacement or repair and isolated valve replacement or repair between 1993 and 2019. Their operative mortality rate was 6%.^3^ The experience of Ikeno et al. operating on 139 patients aged 80 and more of total arch replacement (72.7% elective surgery, 27.3% urgent or emergency surgery) showed an operative mortality at 8.6% and 1-year mortality at 27.2%. The authors concluded that total arch replacement was performed with acceptable survival. However, concomitant procedures significantly increased late-term mortality.^4^ Yamamoto et al. performed a successful combined arch debranching and TEVAR due to an aortic arch aneurysm in a 94-year-old woman.^5^
We described for the first time a scenario of a nonagenarian with complex history of aortic disease who presented a concomitant dilated aortic arch at 67 mm and a severe aortic stenosis. We thought that a conventional open aortic arch surgery with hypothermic cardiac arrest and concomitant aortic valve replacement would have increased the operative risk excessively. The meaningful preoperative multidisciplinary discussion with cardiac surgeons, interventional cardiologists and interventional radiologists was in favour of a hybrid strategy to reduce the overall procedural risk.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Weinberg L, Walpole D, Lee DK, D'Silva M, Chan JW, Miles LF, et al Modern cardiac surgical outcomes in nonagenarians: a multicentre retrospective observational study. Front Cardiovasc Med 2022;9:865008.35911518 10.3389/fcvm.2022.865008 PMC 9330044 · doi ↗ · pubmed ↗
- 2Nasso G, Santarpino G, Di Bari N, Fattouch K, Condello I, Moscarelli M, et al Cardiac surgery in nonagenarians following the TAVI/TMVI era: a multicenter 23-year comparative analysis. J Clin Med 2023;12:2177.36983179 10.3390/jcm 12062177 PMC 10054800 · doi ↗ · pubmed ↗
- 3Elsisy MF, Schaff HV, Crestanello JA, Alkhouli MA, Stulak JM, Stephens EH. Outcomes of cardiac surgery in nonagenarians. J Card Surg 2022;37:1664–1670.35285545 10.1111/jocs.16396 · doi ↗ · pubmed ↗
- 4Ikeno Y, Yokawa K, Yamanaka K, Inoue T, Tanaka H, Okada K, et al Total arch replacement in octogenarians and nonagenarians: a single-center 18-year experience. J Thorac Cardiovasc Surg 2020;160:346–356.e 1.31562010 10.1016/j.jtcvs.2019.07.092 · doi ↗ · pubmed ↗
- 5Yamamoto Y, Uchiyama H, Oonuki M. Total arch debranching thoracic endovascular aortic repair using femoral artery inflow. Int Heart J 2022;63:995–998.36104236 10.1536/ihj.22-153 · doi ↗ · pubmed ↗