Impact of fertility treatments on headache disorders: a systematic review with an overview of treatment modalities
Carolin Luisa Hoehne, Alina Lohner, Yones Salim, Maria Terhart, Wiebke Andersen, Cornelius Angerhöfer, Rüdiger Moltrecht, Florian Scheuerecker, Antoinette Maassen van den Brink, Bianca Raffaelli

TL;DR
Fertility treatments may cause headaches, but their impact is not well understood, requiring better clinical guidance and reporting.
Contribution
This systematic review identifies headache as a common but underreported side effect of fertility treatments.
Findings
Headache rates during fertility treatments range from rare (<1%) to nearly 50%, depending on the medication.
Migraine history is linked to increased risk of complications like ovarian hyperstimulation syndrome.
Current reporting lacks detail on headache type, severity, and timing relative to treatment phases.
Abstract
Infertility represents a global health concern and assisted reproductive technologies expose an increasing number of women and men to intensive hormonal interventions. At the same time, migraine and other headache disorders are highly prevalent in the reproductive age group and hormonal fluctuations are well-established headache triggers. The impact of fertility treatments on headache remains unclear and guidance for clinical management is lacking. This systematic review followed PRISMA guidelines and was pre-registered in PROSPERO. PubMed and Embase were searched up to 1st of August 2025 using predefined strategies combining “migraine” or “headache” with fertility-related terms. Original human studies reporting on common fertility treatments and headache were included. Data were synthesized qualitatively due to heterogeneity in design and outcomes. In parallel, headache-related…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
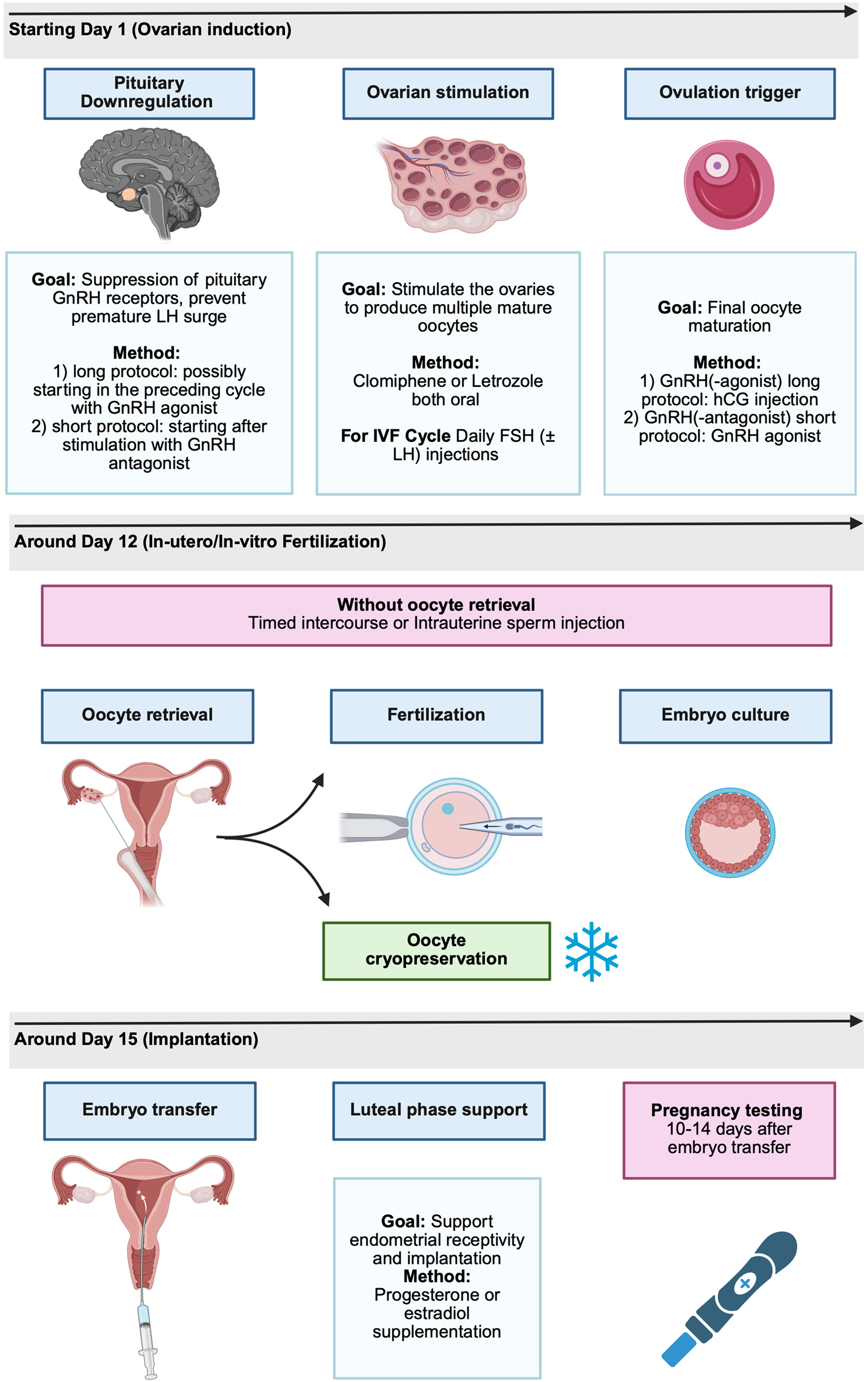 Figure 1
Figure 1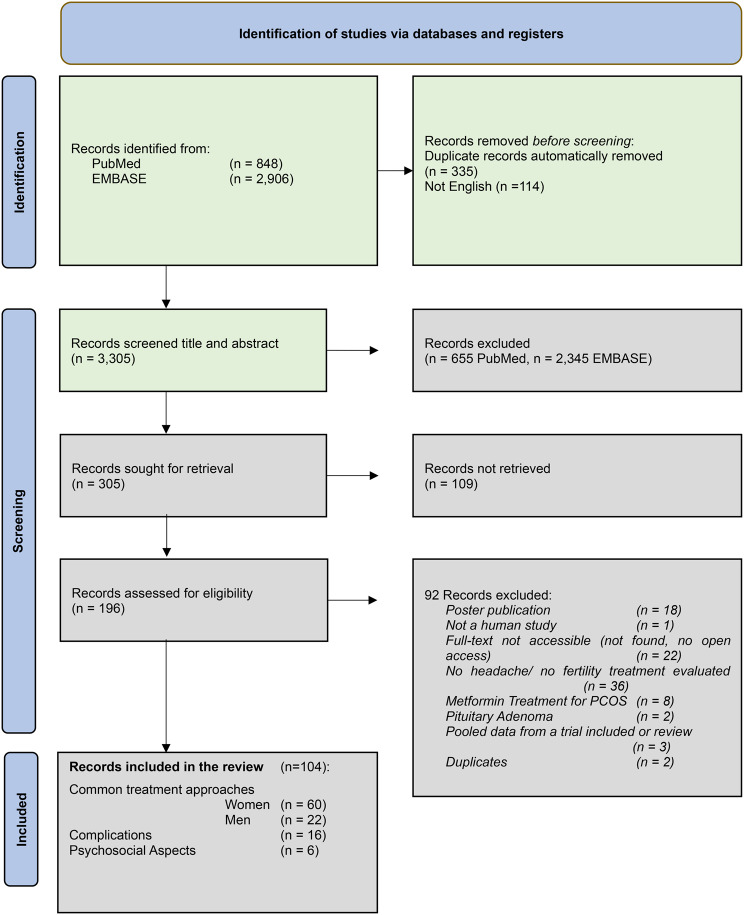 Figure 2
Figure 2|
|
|
|
|
| |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Selective Estrogen Receptor Modulator | Clomiphene | Headache 1.3% | Migraine headache, paresthesia, seizure, stroke, syncope |
| |||||||
| Tamoxifen | n/a | less frequently reported headaches |
| ||||||||
| Raloxifene | Headache 9.2% | Migraine headache, vertigo, neuralgia, hypesthesia |
| ||||||||
| Aromatase Inhibitor | Letrozole (Femara) | Headache 8% | Headache, dizziness, insomnia |
| |||||||
| Anastrozole | Headache 8–10% | Headache, dizziness,insomnia, anxiety, paresthesia, depression |
| ||||||||
|
| |||||||||||
|
|
|
|
|
|
|
|
|
|
|
| |
| (Tredway et al. 2004) [ | Phase I clinical trial | Healthy, premenopausal female volunteers | Anastrozole (single dose vs. five daily doses) | 26 | 20 | 6 | n/a | 36.0% of all subjects (no dose dependency, not specified) | |||
| (Li et al. 2025) [ | Open-label, randomized trial | PCOS | Letrozole (2.5 mg vs 5 mg) | 174 | 87 | 87 | n/a | 18% | 18% | n/a | |
| (Jahan et al. 2022) [ | Open-label, randomized trial | PCOS | Letrozole (low-dose extended vs double-dose short protocol, each 3 cycles) | 66 | 34 | 32 | n/a | 10% | 5% | n/a | |
| (Amer et al. 2017) [ | Double-blind randomized trial | PCOS | Letrozole vs Clomiphene | 159 | 79 | 80 | n/a | Headache in letrozole group, migraine in clomiphen group (no specification) | |||
| (Thomas et al. 2019) [ | Retrospective cohort study | PCOS | Letrozole vs Clomiphene | 92 | 49 | 43 | n/a | “A larger proportion of women in the CC group reported having experienced any side effects associated with treatment than the Letrozole group (41.9% vs 8.2%, | |||
| (Al-Thuwaynee & Swadi, 2023) [ | Open-label, randomized trial | PCOS | Letrozole vs Clomiphene | 100 | 50 | 50 | n/a | 4% | 6% | n/a | |
| (Chera-Aree et al. 2023) [ | Randomized, controlled trial | Ovulation Dysfunction | Letrozole + Clomiphene vs Clomiphene | 100 | 50 | 50 | n/a | 13% | 5% | n/a | |
| (Mejia et al. 2019) [ | Open-label, randomized trial | PCOS | Letrozole + Clomiphene vs Letrozole | 70 | 35 | 35 | n/a | 28% | 41% | n/a | |
| (Panda et al. 2023) [ | Triple-blind, placebo-controlled trial | PCOS | Letrozole + Clomiphene vs Letrozole | 80 | 40 | 40 | n/a | 26% | 29% | n/a | |
| (Von Wolff et al. 2014) [ | direct comparitive trial | Different reasons | HCG vs HCG + clomiphene | 112 | 108 | 103 | n/a | 0% | 5% | n/a | |
| (Jones et al. 2018) [ | Retrospective cohort study | PCOS | Clomiphene (two different protocols) | 109 | 66 | 43 | n/a | 6% | 7% | n/a | |
| (Legro et al. 2014) [ | Open-label, randomized trial | PCOS | Lifestyle vs oral contraceptive pills vs Combined before ovulation induction with clomiphene | 149 | 50 | 49 | 50 | 14% | 9% | 28% | |
| (De Paula Guedes Neto et al. 2011) [ | Double-blind randomized trial | PCOS | Raloxifen vs Placebo | 82 | 42 | 40 | n/a | 2% | 3% | n/a | |
| (Zahran et al. 2018) [ | Open-label, randomized trial | PCOS | Clomiphene + Cabergolin vs Clomiphene | 130 | 65 | 65 | n/a | 20% | 12% | n/a | |
|
| |||||||||||
|
|
|
|
|
|
|
|
|
| |||
| (Shuling et al. 2019) [ | Prospective clinical trial | Idiopathic Oligozoospermia | Letrozole | 15 | n/a | n/a | 25% | n/a | |||
| (Ullur et al. 2025) [ | Double-blind randomized trial | Oligoasthenoteratozoospermia | Letrozole vs Placebo | 54 | 28 | 26 | 21% | n/a | |||
| (Shah et al. 2015) [ | Retrospective cohort study | Hypogonadism and with a BMI ≥ 25 kg/m2 | Anastrozole | 30 | n/a | n/a | 3% | n/a | |||
| (Shah et al. 2021) [ | Retrospective, observational study | Hypogonadism | Anastrozole | 30 | n/a | n/a | 3% | n/a | |||
| (Jones et al. 2023) [ | Double-blind randomized trial | Obesity-associated hypogonadotropic hypogonadism | Leflutozole (low dose or medium dose vs high dose) | 271 | 199 | 71 | 5% | 6% | |||
| (Alder et al. 2018) [ | Retrospective, observational study | Hypoandrogenia, hyperestrogenemia | Clomiphene citrate and Anastrazol | 51 | n/a | n/a | 2% | n/a | |||
| (WHO, 1992) [ | Double-blind randomized trial | Idiopathic impairment of semen quality | Clomiphene citrate vs Placebo | 141 | 70 | 71 | "Two men who were on clomiphene treatment, complained of visual disturbances, dizziness and headaches after 30 and 120 days of treatment respectively." | ||||
| (Chandrapal et al. 2016) [ | Retrospective, observational study | Hypogonadism, Azoospermia or severe oligoospermia | Clomiphene citrate | 77 | n/a | n/a | 1% | n/a | |||
| (Soares et al. 2018) [ | Double-blind randomized trial | Obesity-associated hypogonadism | Clomiphene citrate vs Placebo | 78 | 39 | 39 | 0% | 2% | |||
|
|
|
|
|
| |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Gonadotropin Recombinant FSH | Gonal-f | Headache 10.2% | Headache |
| |||||||
| Puregon (Follistim) | Headache 7.3% | Headache |
| ||||||||
| Bemfola | Headache very common | Headache |
| ||||||||
| Ovaleap | Headache very common | Headache |
| ||||||||
| Gonadotropin Urinary FSH | Menopur | Headache 34.1% | Headache, dizziness |
| |||||||
| Bravelle | Headache 8.1–12.7% (IVF) | Headache |
| ||||||||
| Gonadotropin hMG (FSH + LH) | Repronex | Headache 5.2% (s.c.) to 6.0% (i.m.) | Headache |
| |||||||
| Gonadotropin LH Preparation | Luveris | Headache 9.9–10.2% (up do dosage) | Headache, fatigue |
| |||||||
| hCG (urinary) | Pregnyl | n/a | Headache, depression, fatigue |
| |||||||
| hCG (recombinant) | Ovitrelle/ Ovidrel (Choriogonadodropin alfa) | n/a | Headache |
| |||||||
| Novarel | n/a | Headache, depression, fatigue |
| ||||||||
|
| |||||||||||
|
|
|
|
|
|
|
|
|
|
|
| |
| (Diamond et al. 2015) [ | Randomized, controlled trial | Unexplained infertility | Gonatropin vs Clomiphene vs Letrozole | 900 | 301 | 300 | 299 | 30.0% | 34.9% | 41.9% | |
| (Norman et al. 2011) [ | Phase III uncontrolled trial | Different reasons | FSH (rFSH) | 682 | 682 | 9.1% | |||||
| (Recombinant Human FSH Study Group 1998) [ | Open-label, randomized trial | Different reasons | FSH (rFSH vs uFSH) | 127 | 60 | 63 | n/a | 15.0% | 7.0% | n/a | |
| (Dickey et al. 2002) [ | Open-label, randomized trial | Different reasons | FSH (Urofollitropin s.c. vs. Urofollitropin i.m. vs Follitropin B) | 177 | 60 | 59 | 58 | 8.3% | 16.9% | 10.2% | |
| (Boostanfar et al. 2016) [ | Double-blind, randomized,active-controlled trial | Different reasons | FSH (Corifollitropin alfa vs rFSH) | 298 | 151 | 147 | n/a | 5.3% | 3.4% | n/a | |
| (Pasqualini et al. 2021) [ | Randomized, single-blind trial | Different reasons | FSH (Folitime vs rFSH) | 93 | 49 | 44 | n/a | 14.0% | 4.5% | n/a | |
| (Balen et al. 2007) [ | Open-label, randomized trial | Anovulatory infertility and resistance to clomiphene citrate | FSH (rFSH vs FSH) | 151 | 73 | 78 | n/a | 14.1% | 13.7% | n/a | |
| (Leader & Monofollicular Ovulation Induction Study, 2006) [ | Randomized, group-comparative study | Anovulation or oligoovulation | FSH (Follitropin beta 25 IU vs 50 IU) | 158 | 80 | 78 | n/a | 11.3% | 9.0% | n/a | |
| (Baldini et al. 2023) [ | Case Series | Different reasons | FSH (Follitropin delta) | 4 | n/a | n/a | n/a | 25.0% | n/a | n/a | |
| (Boostanfar et al. 2015) [ | Double-blind, randomized trial | Different reasons | FSH (Corifollitropin alpha vs rFSH) | 1,390 | 695 | 696 | n/a | 6.1% | 5.7% | n/a | |
| (Strowitzki et al. 1995) [ | Open-lable trial | Different reasons | FSH (rFSH vs FSH) | 58 | 15 | 43 | n/a | Headache as a side-effect (not specified) | |||
| (Blockeel et al. 2022) [ | Prospective observational study | Different reasons | FSH (Follitropin dellta) | 944 | 893 | n/a | n/a | 0.2% | n/a | n/a | |
| (Taketani et al. 2010) [ | Single-blind, randomized trial | Oligo- or anovulatory infertility | FSH (Follitropin alpha vs urofollitropin) | 261 | 129 | 132 | n/a | 4.7% | 6.1% | n/a | |
| (Humaidan et al. 2017) [ | Randomized, single-blind trial | Poor ovarian responders | FSH (rFSH + LH vs rFSH) | 939 | 477 | 462 | n/a | 6.1% | 5.9% | n/a | |
| (Marrs et al. 2004) [ | Open-label, randomized trial | Male-factor (not specified) | FSH (rFSH vs rFSH +LH) | 431 | 212 | 219 | n/a | “The most common adverse events were headache and OHSS, each occurring in 18 patients.” | |||
| (Nichols et al. 2001) [ | Open-label, randomized trial | Premenopausal anovulatory and oligoovulatory infertility | FSH + LH s.c. vs FSH + LH i.m. vs hMG | 108 | 36 | 36 | 36 | 6.0% | 8.0% | 19.0% | |
| (Keye et al. 2004) [ | Open-label, randomized trial | Different reasons | hMG (FSH vs hMG) | 228 | 76 | 79 | 73 | 2.6% | 8.9% | 11.0% | |
| (Witz et al. 2020) [ | Single-blind, randomized trial | Different reasons | hMG vs FSH | 619 | 310 | 309 | n/a | 9.4% | 7.0% | n/a | |
| (Platteau et al. 2006) [ | Single-blind, randomized trial | Anovulatory infertility | hMG vs FSH | 184 | 91 | 93 | n/a | 5.4% | 6.5% | n/a | |
| (Alviggi et al. 2007) [ | Open-label, randomized trial | Unknown | hMG (s.c. vs i.m.) | 168 | 85 | 83 | n/a | “The recorded incidence of adverse effects was overall very low and similar in the two subgroups (2.4% vs. 3.7% of patients in the s.c. and i.m. subgroups, respectively); these adverse effects were headache, or aspecific abdominal pain, both not clearly related to the drug's intake." | |||
| (European and Australian Multicenter Studygroup, 1995) [ | Randomzied, placebo-controlled trial | Hypogonadotropic hypogonadism | GH (hMG+ GH vs hMG + Placebo) | 64 | 48 | 16 | n/a | 2.0% | 0.0% | n/a | |
| (Dai et al. 2023) [ | Open-label, randomized trial | PCOS | Letrozole vs Letrozole + hMG | 174 | 87 | 87 | n/a | 31.0% | 25.3% | n/a | |
|
| |||||||||||
|
|
|
|
|
|
|
|
|
| |||
| (Nieschlag et al. 2017) [ | Open-label trial | Hypogonadotropic hypogonadism | hCG | 23 | n/a | n/a | 16.7% | n/a | |||
| (Babak et al. 2018) [ | Randomized, group-comparative study | Infertile patients with varicocele and an abnormal semen analysis | Varicocelectomy + hCG vs Varicocelectomy | 193 | 94 | 99 | 1.0% | 0.0% | |||
| (Burgues & Calderon, 1997) [ | Open-label trial | Hypogonadotropic hypogonadism | FSH + hCG | 60 | n/a | n/a | 0.0% | n/a | |||
|
|
|
|
|
| |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| GnRH Agonist | Leuprorelin (Lupron) | n/a | n/a |
| |||||||
| Buserelin | Headache 63–75% | Headache, dizziness, nervousness, migraine (4–7%) |
| ||||||||
| Nafarelin | n/a | Headache |
| ||||||||
| GnRH Antagonist | Cetrorelix (Cetrotide) | Headache 1.1% | Headache |
| |||||||
| Ganirelix (Orgalutran) | Headache 24% | Headache |
| ||||||||
|
| |||||||||||
|
|
|
|
|
|
|
|
|
|
|
| |
| (Prajapati et al. 2017) [ | Prospective, observational study | PCOS | Clomiphene vs GnRH agonist (long and short) vs GnRH Antagonist | 95 | 38 | 51 | 6 | 0.0% | 11.8% | 33.3% | |
| (Cozzolino et al. 2023) [ | Prospective observational study/case reports | Adenomyosis | GnRH-Agonist and Letrozole | 4 | n/a | n/a | n/a | one case presented with migraine (not specified whether they were pre-existing) | |||
| (El-Nemr et al. 2002) [ | Comparative cohort study | Different reasons | Buserelin vs Leuprorelin vs Nafarelin | 157 | 51 | 53 | 53 | 37.3% | 45.3% | 60.4% | |
| (J.A. Huirne et al. 2006) [ | Randomized study | Different reasons | Cetrorelix vs Buserelin | 182 | 91 | 91 | n/a | 17.6% | 40.7% | n/a | |
| (Amir et al. 2005) [ | Retrospective study | Different reasons | different | 98 | 98 | n/a | n/a | 28.6% | |||
| (Huirne et al. 2004) [ | Double-blind, randomized trial with open-label treatment phase | Different reasons | GnRH Antide | 144 | 144 | n/a | n/a | “most frequently recorded side effects were general disorders (especially fatigue and headache)” | |||
| (Judith Af Huirne et al. 2006) [ | Randomized trial | Different reasons | GnRH Antide | 63 | 31 | 32 | n/a | 37.0% | 45.0% | n/a | |
| (Tapanainen et al. 1993) [ | Open-label, randomized trial | Different reasons | Goserelin vs Buserelin | 100 | 49 | 51 | n/a | “ … patients in the buserelin group suffered more from headache than those given s.c. goserelin.” | |||
| (Sauer et al. 2004) [ | Open-label, randomized trial | Different reasons | Leuprolide vs Certorelix | 74 | 74 | n/a | n/a | “ … 17 (23.0%) reported adverse event” (not specified) | |||
| (Goldman et al. 1994) [ | Randomized trial | Different reasons | Nafarelin vs Buserelin | 108 | 53 | 55 | n/a | 18.9% | 12.7% | n/a | |
| (Lockwood 1995) [ | Randomized, single-blind trial | Different reasons | Nafarelin vs Buserelin | 342 | 172 | 170 | n/a | 19.0% | 50.0% | n/a | |
| (Komiya et al. 2022) [ | Open-label, case–control trial | Different reasons | Relugolix vs Ganirelix | 785 | 127 | 658 | n/a | 0.0% | 1.6% | n/a | |
| (Simons et al. 2005) [ | Double-blind, randomized trial | Different reasons | Triptorelin (different protocol length: short medium and long) | 178 | 58 | 62 | 58 | 3.4% | 4.8% | 0.0% | |
| (Lobo et al. 2024) [ | Open-label, randomized trial | Different reasons | Triptorelin vs Cetrorelix | 437 | 221 | 216 | n/a | 13.4% | 14.2% | n/a | |
|
| |||||||||||
|
|
|
|
|
|
|
|
|
|
|
| |
| (Foresta et al. 2004) [ | Randomized, group-comparative study | Oligozoospermia | Leuprolide + r-hFSH vs r-hFSH | 97 | n/a | n/a | n/a | 16.0% | 0.0% | n/a | |
|
|
|
|
|
| |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Progesterone (vaginal) | Crinone gel | Headache 13–17% | Headache, dizziness,depression, nervousness |
| |||||||
| Progesterone (oral) | Dydrogesterone (Duphaston) | Common | Migrane/headaches, dizziness, Somnolence |
| |||||||
| Progesterone (IM) | Progesterone in oil | n/a | Headache, fatigue, nervousness, dizziness |
| |||||||
| Estrogen | Estradiol valerate (Delestrogen) | n/a | Headache, migraine, dizziness, depression, nervousness |
| |||||||
| Estrogen | Estrogen (oral/transdermal) | Headache 13–14% depending on dose | Headache, migraine, dizziness, depression, nervousness |
| |||||||
|
| |||||||||||
|
|
|
|
|
|
|
|
|
|
|
| |
| (Garimella et al. 2021) [ | Prospective, observational trial | Different reasons | Estradiol (oral vs transdermal) | 294 | 156 | 138 | 17.3% | 3.6% | |||
| (Tran et al. 2024) [ | Open-label, randomized trial | Different reasons | Estradiol (oral vs transdermal) | 380 | 190 | 190 | 5.5% | 0.6% | |||
| (Satirapod et al. 2014) [ | Double-blind, cross-over, placebo-controlled trial | Healthy women | Estradiol (oral) + Clomiphene vs Clomiphene + Placebo | 34 | 30 | 30 | 0.0% | 10.0% | |||
| (Colombo et al. 2023) [ | Randomized controlled trial | Different reasons | Progesterone vs placebo | 470 | 235 | 235 | 44.3% | 45.6% | |||
| (Karadeniz et al. 2023) [ | Randomized controlled trial | Different reasons | Progesterone (intramuscular vs vaginal vs oral) | 195 | 50 | 94 | 51 | 2% | 0% | 15.7% | |
| (Ozer et al. 2021) [ | Open-label, randomized trial | Different reasons | Progesterone (oral vs trans vaginal) | 134 | 67 | 67 | 13.8% | 0.0% | |||
| (Lockwood et al. 2014) [ | Open-label, randomized trial | Different reasons | Progesteron (subcutaneous vs. Gel) | 683 | 339 | 344 | 5.3% | 4.9% | |||
| (Stadtmauer et al. 2013) [ | Prospective, randomized, single-blind, phase III clinical trial | Different reasons | Progesterone (vaginal ring vs vaginal gel) | 1,297 | 646 | 651 | 20.0% | 26.0% | |||
| (Bergh et al. 2012) [ | Assessor-blinded, randomized trial | Different reasons | Progesterone (Gel bs tablets) | 2,057 | 991 | 992 | 1/6 cases of adverse events was due to headache (no specification) | ||||
| (Ng et al. 2003) [ | Open-label, randomized trial | Different reasons | Progesterone (Tablet vs gel) | 60 | 30 | 30 | “No significant differences were demonstrated in ( …)headache.” | ||||
| Author, Year | Titel | Study Design | Reason for Infertility | Fertility treatment | Phase | Category |
|---|---|---|---|---|---|---|
| (Man & Hui, 2011) [ | Cerebral venous thrombosis secondary to ovarian hyperstimulation syndrome | Case Report | Unknown | Full Protocol | Ovarian hyperstimulation | vascular |
| (Akinci & Anash, 2025) [ | Cytotoxic Lesion of the Corpus Callosum Related to Migraine With Aura Triggered by In Vitro Fertilization and Embryo Transfer: A Case Report. | Case Report | PCOS | Full Protocol | 10 days after fertility treatment and no pregnancy | vascular |
| (Zahid et al. 2016) [ | Intracranial venous thrombosis in a man taking clomiphene citrate. | Case Report | Oligospermia | SERM (Clomiphene) | Male infertility | vascular |
| (Koh et al. 2021) [ | Ischemic Stroke Associated With Ovarian Hyperstimulation Syndrome | Case Report | Unknown | Full Protocol | Ovarian hyperstimulation | vascular |
| (Tehraninejad et al. 2010) [ | Late onset fasting triggered thrombosis of internal carotid artery after ovarian stimulation | Case Report | PCOS | Full Protocol | Ovarian stimulation | vascular |
| (Akça & Özdemir, 2022) [ | Postpartum intracerebral hematoma following in vitro fertilization | Case Report | Unknown | Full Protocol | Post-partum | vascular |
| (Shmorgun et al. 2009) [ | Renal artery dissection during an in vitro fertilization/intracytoplasmic sperm injection cycle | Case Report | Secondary infertility (not specified) | Full Protocol | Ovarian stimulation | vascular |
| (Freilinger et al. 2010) [ | Reversible cerebral vasoconstriction syndrome associated with hormone therapy for intrauterine insemination | Case Report | Unexplained infertility | Full Protocol | After insemination | vascular |
| (Kobak et al. 2014) [ | Scleroderma renal crisis and ovarian hyperstimulation syndrome related to the use of clomiphene in a patient with scleroderma | Case Report | Unknown | SERM (Clomiphene) | Ovarian hyperstimulation | vascular |
| (Edris et al. 2007) [ | Successful management of an extensive intracranial sinus thrombosis in a patient undergoing IVF: case report and review of literature. | Case Report | Multiple uterine fibroid | Full Protocol | Ovarian hyperstimulation | vascular |
| (Motegi et al. 2012) [ | Hemorrhagic onset of rhabdoid meningioma after initiating treatment for infertility. | Case Report | Unknown | SERM (Clomiphene) | Ovarian stimulation | tumor |
| (Ramos et al. 2022) [ | Meningeal Melanomatosis with a Spinal Meningeal Melanocytoma Trigger by an in vitro Fertilization | Case Report | Unknown | Full Protocol | Unspecific “after IVF” Treatment | tumor |
| (Alnahas et al. 2025) [ | Pituitary Mimic: Sellar Meningioma in a Patient Undergoing Fertility Therapy. | Case Report | Hypertension, prediabetes, hypothyroidism, and mild hyperprolactinemia | GNRH-Agonist (unspecific) | Ovarian stimulation | tumor |
| (Gaul et al. 2007) [ | Cluster headache triggered by high-dose gestagens in the context of in vitro fertilization: a case report. | Case Report | Endometriosis and male subfertility | Full Protocol | Luteal support | primary headache |
| (Rollene et al. 2011) [ | Migraines and ovarian hyperstimulation syndrome: a dopamine connection. | Retrospective case-control study | Unknown | Full Protocol | Ovarian hyperstimulation syndrom | primary headache |
| (Rodrigues et al. 2014) [ | Psychotic episode secondary to gonadotrophins | Case Report | Secondary infertility (not specified) | Full Protocol | Ovarian stimulation | other |
- —Charité - Universitätsmedizin Berlin (3093)
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMigraine and Headache Studies · Reproductive Health and Technologies · Assisted Reproductive Technology and Twin Pregnancy
Introduction
Infertility is a significant and growing global health concern, affecting an estimated 110 million women and 55 million men worldwide as of 2021 [1, 2]. The burden of infertility is highest among women aged 35–39 years, and the prevalence has increased by over 80% since 1990, with projections indicating a continuing rise through 2040 [1, 2]. Infertility is associated with substantial psychological distress, including increased rates of depression and anxiety, and can have profound social and economic consequences for affected individuals and couples [3]. The etiology of infertility is multifactorial, encompassing endocrine, anatomical, genetic, and environmental factors, and remains unexplained in a significant proportion of cases [4].
In response to the rising prevalence and impact of infertility, the use of assisted reproductive technologies (ART), particularly in vitro fertilization (IVF), has expanded rapidly worldwide. Globally, more than 3.5 million ART cycles are performed each year, resulting in almost one million born infants [5, 6]. While ART has improved reproductive outcomes for many, it also introduces new physiological and psychosocial challenges, including the potential for adverse effects on neurological health [7, 8]. In addition to fertility treatment, ART is increasingly used for fertility preservation through oocyte or embryo freezing, both in medical contexts, such as prior to gonadotoxic cancer therapy, and for social reasons, contributing to a broader and growing population undergoing hormonal stimulation [9]. The complexity of ART regimens, the emotional burden of infertility, and the uncertainty of outcomes can contribute to psychological distress and may impact quality of life.
The relationship between headache disorders, most notably migraine, and fertility is increasingly recognized as bidirectional [10]. Women with migraine are more likely to avoid or delay pregnancy due to concerns about symptom exacerbation, medication teratogenicity, and disability during gestation, with up to 20% of women reporting avoidance of pregnancy for these reasons [11]. Notably, these concerns contrast with clinical observations showing that migraine improves during pregnancy in approximately 60–80% of women [12]. In addition, pre-existing migraine is associated with a higher prevalence of endocrine comorbidities such as endometriosis or thyroid disorders, which may impair fertility [13, 14]. Within the spectrum of endocrine disorders affecting fertility, polycystic ovary syndrome (PCOS) occupies a central role, as it is a leading cause of anovulatory subfertility and a frequent indication for fertility treatment [15]. In women with PCOS, the relationship with migraine is complex and characterized by heterogeneous findings. While some studies report an increased prevalence of migraine in women with PCOS, others found no association or even suggested a reduced prevalence, potentially related to attenuated cyclical hormonal fluctuations [13, 16, 17].
Fertility treatments themselves may provoke or worsen headache, particularly in women with a prior history of migraine. Despite the clinical relevance and growing use of fertility treatments, evidence on the occurrence, characteristics, and clinical context of headache during fertility treatment remains limited and heterogeneous. To address this gap, we present a systematic review of the available literature on whether fertility treatments may trigger or exacerbate headache.
Methods
This review was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines.
The review protocol was pre-registered in PROSPERO 2025 (CRD420251119054). After the abstract screening stage, the scope of the review was refined to focus exclusively on studies examining common fertility treatments and headache.
The primary objective of this systematic review was to examine whether fertility treatments have an impact on headache, both in individuals with pre-existing headache disorders and in those without a prior headache history.
Given the heterogeneity of study designs, populations, treatments and outcome measures, a quantitative meta-analysis was not feasible, and findings were synthesized in a systematic review.
Screening and Selection
A comprehensive literature search was performed in PubMed and Embase from database inception up to August 2025. The PubMed search (conducted on August 1, 2025) used the terms (migraine OR headache) AND (fertil* OR infertil*). The Embase search was performed on August 15, 2025, using the following strategy:
exp migraine/OR migraine.ti,ab. OR exp headache/OR headache*.ti,ab.; exp fertility/OR fertil.ti,ab. OR exp infertility/OR infertil.ti,ab.*; 1 AND 2.
In response to peer-review comments and to improve sensitivity, the PubMed search strategy was subsequently expanded on the 8th of February 2026 to include commonly used treatment-related terms referring to assisted reproductive technologies. We used the following terms “IVF”, “ICSI”, “ovarian stimulation”, “OHSS”, embryo transfer”, “luteal support”, “cryopreservation”, “agents, fertility[MeSH Terms]”, each combined with “migraine OR headache”. Duplicates were removed using EndNote 2025.
All retrieved records underwent a two-stage screening process. In the first stage, titles and abstracts were screened by independent reviewers. Six reviewers (CLH, CA, MT, WA, YS, BR) participated in this process, and each record was evaluated by two reviewers randomly assigned within this pool. Any record judged as potentially eligible by either reviewer proceeded to full-text screening. In the second stage, full-text articles were reviewed independently by two reviewers (CLH, BR) against predefined inclusion and exclusion criteria. Discrepancies at either stage were resolved through discussion, and a third reviewer was consulted if consensus could not be reached.
Inclusion and Exclusion Criteria
Studies were considered eligible for inclusion if they were original research articles that reported on common fertility treatment (such as selective estrogen receptor modulator (SERM)), aromatase inhibitors, gonadotropins, gonadotropin-releasing hormone(GnRH)-analogue and luteal support with estrogens or progesterone) and headache, either pre-existing or newly developed. Only full-text articles published in English were included. Eligible study designs comprised randomized controlled trials, prospective or retrospective observational studies, and registry-based analyses.
We excluded publications (1) that were not original research, such as reviews, conference abstracts, posters or letters. (2) Studies that did not involve human participants or (3) that lacked relevant outcome data on headache in the context of fertility treatment were also excluded. (4) Fertility treatment with other substances (like metformin), adjunctive or additive treatment, was also excluded. (5) We excluded articles focusing solely on hyperprolactinemia, which is often caused by pituitary tumors, even though both can cause headaches, contribute to infertility, or the tumor can enlarge during fertility treatment [18]. Given the extensive literature on this topic and its classification as a secondary headache, we did not include it in our analysis [19, 20].
Data Extraction and Analysis
Data from eligible studies were extracted into a standardized table, including study design, type of fertility treatment, reason for fertility treatment, number of study population and headache outcomes. We grouped fertility treatments by drug class and sex.
Drug-Label
In addition to the systematic literature review, information on reported headache as an adverse event was extracted from the official U.S. Food and Drug Administration (FDA) drug labeling database. For all pharmacological agents used in fertility treatment identified in this review, the most recent FDA-approved prescribing information was accessed via the FDA website on October 29, 2025. Data were extracted for each drug regarding the presence, frequency, and classification of headache within the adverse reactions or postmarketing experience sections.
When FDA labeling was unavailable, data were retrieved from the European Medicines Agency (EMA) product information database.
Overview of Fertility Treatments
Infertility is defined as the inability to achieve pregnancy after 12 months of regular, unprotected sexual intercourse [4]. Fertility evaluation and treatment is indicated after this time, even earlier in certain cases (for example, in advanced maternal age, or with known risk factors). Around 30–40% of cases are attributed to female factors, 30–40% to male factors, and in 20–30% both partners contribute [21].
To contextualize the findings of this systematic review and support the interpretation of the included studies, we provide a brief overview of fertility treatment strategies (Fig. 1). These include ovulation induction alone or in combination with intrauterine insemination (IUI), as well as more advanced techniques such as IVF and intracytoplasmic sperm injection (ICSI). This section is intended solely as clinical background information to aid interpretation of the results and does not represent part of the systematic review methodology.Fig. 1. Overview of fertility treatment. Overview of a standard fertility treatments, illustrating key hormonal intervention phases from ovarian induction and stimulation to fertilization, embryo transfer, and luteal phase support. Created with BioRender.com
Ovulation Induction and Ovarian Stimulation
Ovulation induction and ovarian stimulation are among the main treatment approaches in fertility treatment, with the first aiming to trigger ovulation in anovulatory women, and the second helping to stimulate the development of multiple follicles, also in normally ovulating women [22].
Two main oral agents are mostly used: clomiphene (or clomiphene citrate) and letrozole [4]. Clomiphene is a SERM that blocks estrogen receptors in the hypothalamus, thereby disrupting the normal negative feedback mechanism [23]. This leads to an increased release of GnRH, which subsequently stimulates follicle-stimulating hormone (FSH) and luteinizing hormone (LH), promoting follicular growth and ovulation. Clomiphene has been the first-line treatment for anovulatory infertility, with ovulation rates of up to 80% and pregnancy rates of approximately 30–40% over multiple cycles [22].
Letrozole inhibits the aromatase enzyme responsible for converting androgens to estrogens, thereby reducing circulating estrogen levels. The resulting decrease in negative feedback to the hypothalamus enhances GnRH secretion and promotes FSH release. Recent trials show that letrozole achieves higher live birth rates than clomiphene, especially in overweight or clomiphene-resistant women, and is now the preferred first-line therapy for PCOS [24].
In cases where oral treatments are ineffective, or when higher follicular recruitment is desired such as in IVF and ICSI cycles, exogenous gonadotropins (recombinant FSH, with or without LH, or human menopausal gonadotropin (hMG) can be administered for ovarian stimulation [25]. These injectables directly stimulate follicular development and are more potent than oral medications. However, they carry a significantly higher risk of multiple gestation and ovarian hyperstimulation syndrome (OHSS), a potentially serious iatrogenic complication characterized by increased vascular permeability, ascites, and thromboembolic risk [4]. Gonadotropin protocols require careful monitoring with serial transvaginal ultrasound and serum estradiol levels measurements to optimize response and minimize complications.
Ovulation induction and ovarian stimulation can be used in combination with timed intercourse, IUI, IVF or ICSI.
Intrauterine Insemination
IUI involves the direct injection of motile sperm into the uterine cavity, bypassing the cervical barrier and increasing the chances of fertilization. IUI is usually timed 24 to 36 hours after administration of an ovulation trigger. IUI solely and without ovulation induction is not recommended because it does not improve pregnancy rates in uncertain infertility [4].
In-Vitro Fertilization, Intracytoplasmic Sperm Injection and Cryopreservation
When less invasive treatments are unsuccessful, or in the presence of specific indications such as severe male factor infertility or tubal obstruction, ovarian stimulation followed by transvaginal oocyte retrieval is performed for IVF or ICSI. Oocyte retrieval is also carried out for fertility preservation, either for medical reasons (e.g., prior to gonadotoxic therapy) or increasingly for elective purposes to preserve reproductive potential with advancing age [26, 27].
This process involves multiple coordinated phases [28]. Ovarian stimulation is preceded or accompanied by pituitary downregulation, which can be achieved using either a long GnRH agonist protocol or a short GnRH antagonist protocol [29].
In the long GnRH agonist protocol, treatment is initiated in the preceding menstrual cycle, prior to the stimulation cycle. Administration of a GnRH agonist initially induces a transient flare effect, characterized by a short-term increase in LH secretion [29]. With continued administration, pituitary GnRH receptors become downregulated, leading to suppression of endogenous gonadotropin release and reduced estradiol levels. This establishes a stable hormonal baseline prior to controlled ovarian stimulation with exogenous gonadotropins.
In contrast, the short (antagonist) protocol involves the administration of a GnRH antagonist during the mid-follicular phase of ovarian stimulation, providing immediate suppression of endogenous LH secretion and preventing a premature LH surge without an initial flare effect [29].
Follicular development is monitored through serial transvaginal ultrasound examinations and hormonal assays. Once the leading follicles reach an appropriate diameter, final oocyte maturation is induced by a trigger injection using either human chorionic gonadotropin (hCG) in the long protocol or a short-acting GnRH agonist in the short protocol. This trigger mimics the natural LH surge and is precisely timed to allow oocyte retrieval approximately 34–36 hours later, before spontaneous ovulation occurs.
Transvaginal oocyte retrieval is performed under ultrasound guidance and light sedation or general anesthesia. A needle is inserted into each follicle to aspirate follicular fluid, from which mature oocytes are isolated in the embryology laboratory. On the same day, sperm cells are collected and fertilization is performed. In conventional IVF, thousands of sperm cells are co-incubated with each mature oocyte. Alternatively, ICSI may be used, especially in cases of severe male factor infertility. ICSI involves the direct injection of a single sperm cell into the oocyte cytoplasm, significantly increasing the chance of fertilization [30].
Fertilized embryos are cultured in-vitro for several days, normally for 2–6 days. At this point, one or more embryos are selected for transvaginal embryo transfer into the uterine cavity using a thin catheter. The luteal phase is supported with progesterone or estogene supplementation to enhance the implantation potential [31].
Approximately 10–14 days after embryo transfer, a serum β-hCG test is performed to confirm pregnancy. If positive, a transvaginal ultrasound is scheduled at around 6–7 weeks of gestation to confirm intrauterine implantation and detect fetal cardiac activity.
For oocyte cryopreservation, oocytes are retrieved following ovarian stimulation, either as part of elective fertility preservation or when oocytes obtained during IVF or ICSI cycles are not used in the cycle. They are then preserved via vitrification, a rapid-freezing technique that maintains oocyte integrity by minimizing ice crystal formation.
Male Infertility
Depending on the underlying etiology, male infertility may be managed with medical therapy, surgical interventions, or assisted reproductive technologies [32]. Many infertile men present with primary testicular dysfunction, characterized by impaired spermatogenesis and reduced sperm output. These conditions are typically associated with hypergonadotropic hypogonadism, reflecting a lack of negative feedback from the testes despite increased pituitary gonadotropin secretion. As the target organ, the testes, does not respond adequately, causal treatment options are limited, and most affected men require assisted reproductive technologies such as IVF or ICSI to achieve conception [32]. In a small subset of men, primarily those with hypogonadotropic hypogonadism, infertility can be treated causally, as the hypothalamic–pituitary–testicular axis is intact and spermatogenesis can be stimulated through gonadotropin therapy [33]. In these cases, treatment with hCG with or without FSH represents the established first-line approach.
For idiopathic infertility or oligozoospermia with low testosterone, SERMs such as clomiphene or aromatase inhibitors may be used off-label, although supporting evidence remains limited [34]. Importantly, exogenous testosterone is contraindicated, as it suppresses spermatogenesis [35].
Results: Does Fertility Treatment Have an Impact on Headache?
This systematic review identified studies addressing the relationship between fertility treatment and headache, both in individuals with and without pre-existing headache disorders. The initial literature search retrieved 848 records from PubMed and 2,906 from Embase, published up to August 2025 (Fig. 2). After removal of duplicates, 3,305 records remained for title and abstract screening. Of these, 196 articles were selected for full-text review, and 92 were excluded based on predefined criteria. To provide a structured overview, results are organized into thematic areas: (1) common fertility treatment approaches for both women and men (Tables 1, 2, 3 and 4), (2) treatment-related complications (Table 5), and (3) psychosocial aspects. To contextualize the literature findings, we first summarize the reported rates of headache and migraine in the FDA and/or EMA labels of key medications used in fertility treatment. We then present the results of the included studies identified through our systematic search.Fig. 2PRISMA flow diagram of study selection
Common Fertility Treatment Approaches
Selective Estrogen Receptor Modulators and Aromatase Inhibitors
According to FDA labeling, SERM show a lower incidence of headache (1.3–9.2%) compared with aromatase inhibitors (8–13.1%) [36–40]. Migraine as a side effect is explicitly mentioned for the SERMs clomiphene and raloxifene.
Consistent with these safety data, many studies retrieved in our search have also reported headache as a frequent adverse event during oral fertility treatment (Table 1). However, the included studies varied in design and size, comprising 17 randomized controlled trials and 6 observational studies, with sample sizes ranging from n = 15 to n = 271. Reporting of headache was inconsistent across studies, and there was no information about intensity or type of headache. Migraine was only once mentioned as a side effect of clomiphene [41].
Across studies, letrozole shows inconsistent rates of headache, ranging from 1% to 41%, yet no consistent pattern emerges with dose or duration [41, 43, 44, 46, 48, 49, 63, 64]. For example, in a trial of 66 women comparing an extended low-dose protocol with a short double-dose regimen, headache was the most frequent but non-severe adverse event, occurring in 10% vs. 5% of participants [44]. Similarly, a study of 174 participants reported identical headache rates (18% in both arms) for 2.5 mg versus 5 mg letrozole used together with human menopausal gonadotropin (hMG) [43].
Anastrozole, another aromatase inhibitor, showed comparably high headache frequency: in a phase I dose-comparison study, 36% of participants experienced headaches [42].
In contrast, clomiphene-based protocols consistently demonstrated lower headache frequencies. A retrospective study of 109 women with PCOS found headache rates of 6% and 7% across two clomiphene regimens [51]. Another study evaluating 112 cycles reported similarly low rates (5% with clomiphene vs. 0% without) in an hCG-based protocol [50].
In a randomized trial of 82 women with PCOS, raloxifene also showed minimal headache incidence, with headache rates comparable to placebo (2% vs. 3%) [52].
Three comparative studies of letrozole versus clomiphene produced inconsistent findings. A double-blind randomized trial including 159 women reported similar overall rates of adverse events but did not specify headache frequencies. It was noted only that headache occurred in the letrozole group, whereas migraine was reported in the clomiphene group, with no more details [41]. A retrospective cohort of 92 participants found that clomiphene was associated with more frequent adverse events, including headache, than letrozole (41.9% vs 8.2%) [45]. Finally, an open-label trial with 100 participants observed only minimal differences in reported headaches in the clomiphene compared to the letrozole group (6% vs 4% respectively) [46].
Combination regimens also showed mixed results. Two additional trials comparing letrozole alone with letrozole plus clomiphene in women with PCOS found higher headache rates in the letrozole-alone arm (28% vs 41%, and 26% vs 29%) [48, 49]. In contrast, a randomized trial of 100 participants reported higher headache rates with the combination of letrozole and clomiphene compared with clomiphene alone (13% vs 5%) [47].
Among other add-on therapies, the combination of cabergoline and clomiphene nearly doubled headache frequency compared with clomiphene alone in a study of 130 women with PCOS [53].
Interestingly, six studies reported headaches in association with aromatase inhibitors in men [54–59]. In a randomized dose-comparison study of 271 men, letrozole caused headaches in 5% of participants, without evidence of a dose–response relationship [58]. Two trials evaluating letrozole for male factor infertility, including oligozoospermia (low sperm concentration) and oligoasthenoteratozoospermia (combined impairment of sperm concentration, motility, and morphology) reported headache among the most common adverse effects, affecting 25% [54] and 21% of participants [55], respectively.
Anastrozole, by contrast, was associated with a much lower headache incidence: in two retrospective studies, each evaluating 30 men, only 3% reported a minor headache [56, 57] and its combination with clomiphene showed low incidence (2%) [59].
In the three studies reporting about clomiphene in men as a therapy for infertility related to low testosterone, headache was reported at low rates in randomized, double-blind, controlled trials, ranging from 0% in a study on obesity-associated hypogonadism to 3% in a trial of idiopathic male infertility [60–62].
Gonadotropins
Based on regulatory labeling from the FDA and EMA, headache is commonly reported as an adverse effect across all gonadotropin preparations, including recombinant and urinary-derived FSH, hMG, LH, and hCG formulations [65–75].
In our systematic review, however, the 21 trials with gonadotropins in women reported variable headache rates between 0 and 15% (Table 2). In women, the literature comprised many interventional studies, including randomized controlled and open-label trials, as well as one small case series. Study populations were heterogeneous and included women with PCOS, unexplained infertility, clomiphene resistance, anovulatory infertility, and mixed infertility indications. Sample sizes ranged widely, from n = 4 to n = 1,390. In men, evidence was limited to three interventional studies, primarily evaluating hCG with or without FSH in the context of hypogonadotropic hypogonadism or impaired spermatogenesis.
One study compared fertility treatment across clomiphene, letrozole, and gonadotropins. This large randomized trial of 900 women with unexplained infertility observed higher and more comparable rates: 35% in the clomiphene group, 42% in the letrozole group, and 35% among those treated with gonadotropins [76].
In trials of recombinant FSH formulations, including follitropin delta and corifollitropin alfa (a long-acting recombinant FSH analogue), headache occurred in 0.2%–15% of participants [77–88]. Studies comparing highly purified or urinary-derived FSH, such as urofollitropin, showed similar rates between 4% and 14% [79, 82, 88].
In a randomized trial including 939 participants, comparing FSH plus LH with FSH alone, headache was reported in 6% in each group. Another study with 431 participants comparing FSH plus LH with FSH alone identified headache as the most frequently reported adverse event, although the authors did not specify differences between treatment groups [89, 90].
In hMG-based regimens, either alone or in combination with recombinant FSH, headache occurred in 2%–10% of cases [91–96].
In contrast, a study of 174 women with PCOS comparing letrozole alone with letrozole plus hMG reported high headache rates (31% and 25%, respectively) suggesting that protocols involving aromatase inhibitors may be associated with more frequent headache than gonadotropin-add on regimens [63].
Among three studies involving men treated with hCG either combined with varicocelectomy or alongside FSH, headache occurred in isolated cases, though in one study the intensity was severe enough to prompt withdrawal [97–99].
GnRH Analogues
FDA-labeling identifies headache as one of the most frequently reported central nervous system adverse effects of both GnRH agonists and antagonists, with migraine explicitly noted in some post-marketing data [100–104]. In alignment with these data, 14 studies identified in this review likewise reported headache as a common adverse event during GnRH analogues treatment in women (Table 3) [64, 105–115]. Reported frequencies varied widely, ranging up to 45%, with a mean incidence of approximately 24%. Comparisons between GnRH agonists (buserelin, leuprorelin, triptorelin, goserelin, nafarelin) and antagonists (cetrorelix, ganirelix, relugolix, antide) revealed no consistent differences in headache occurrence. In a study of 95 women with PCOS randomized to three treatment groups, headache was reported in 0% of those receiving clomiphene, 12% across two GnRH agonist protocols, and 33% in the GnRH antagonist group [116].
In a trial of 97 men treated with either a combination of the GnRH agonist leuprolide acetate plus FSH or FSH alone, headaches were only reported during the GnRH-agonist phase, affecting 16% of participants [118].
Luteal Phase Support
FDA-Drug label data indicate that estrogen and progesterone formulations used for luteal support frequently list headache and migraine among central nervous system–related adverse effects [119–123].
Compared to the FDA-Data, we found in ten studies evaluating estradiol and progesterone preparations for luteal support that headache was reported inconsistently (Table 4). In studies using estradiol (oral, transdermal, or gel formulations), headache occurred in 0.6%–17.3% of participants [124–126]. Comparisons between oral and transdermal estradiol indicated a slightly higher incidence of headache with oral administration, while also the plasma levels of estradiol are higher with oral administration. Interestingly, in a cross-over trial of 34 women comparing clomiphene plus placebo with clomiphene plus estradiol for effects on endometrial thickness, three headache events were reported in the placebo group, two of which led to discontinuation, whereas no headache occurred in the estradiol group [126].
Seven trials investigating progesterone (including vaginal, oral and injectable formulations) reported variable rates between 0% and 20% [127–133].
Systematic Assessment of Headache Data Across Common Fertility Treatments
The only study that systematically assessed headache patterns in the context of fertility treatment, a retrospective telephone-based survey of 98 women, found that headaches occurred significantly more often during the initial GnRH analogue treatment for pituitary downregulation phase of IVF, although the specific agent used was not reported [117]. Notably, 17.8% of non-migraine patients also reported IVF-related headaches.
Across all other fertility treatment studies included in this review, reporting of headache was markedly nonspecific. Only one study differentiated between migraine and headache, but also with no further specification and no incidence rate, and none documented whether participants had pre-existing headache or migraine [41]. Headache was only reported as a general adverse event, without details on severity, timing, or clinical phenotype.
Headache and Treatment-Related Complications
Complications arising during or after fertility treatment are of particular interest when evaluating the occurrence of headache (Table 5). Across 15 case reports and one retrospective case-control study [134–149] headache mostly preceded neurological deficits and often occurred in the context of OHSS. Vascular events were the most common, including cerebral venous thrombosis, ischemic stroke, and reversible cerebral vasoconstriction syndrome, typically arising during or shortly after ovarian stimulation. However, also one male patient developed intracranial venous thrombosis after clomiphene use [136].
Other rare complications included intracerebral hematoma after IVF and cesarean delivery [139] and tumor-related events such as meningioma or melanomatosis following gonadotropin or clomiphene therapy [144–146]. One case described a psychotic episode with severe headache secondary to gonadotropin administration [149].
While most cases described secondary headache due to identifiable complications, three publications focused on the onset or exacerbation of primary headache disorders in relation to hormonal therapy.
Rollene et al (2011) conducted a retrospective case–control study comparing women who developed OHSS after IVF with those who did not [148]. A prior history of migraine was a strong predictor for developing OHSS. In the univariate analysis (combined cohort of IVF and superovulation), the risk of OHSS was increased 4.8-fold in patients with a history of migraine (OR = 4.78, 95% CI 2.63–8.66, p < 0.001).
One report described a 26-year-old woman who developed migraine with aura 1.5 years before the reported complication, at the time she began fertility treatment for PCOS [135]. The onset of migraine with aura in early adulthood is common and does not necessarily indicate a causal relationship with the underlying reproductive condition. The most severe migraine attack occurred shortly after a failed embryo transfer, when MRI revealed a cytotoxic lesion of the corpus callosum. This lesion type is believed to result from inflammatory cascades leading to cytokine release and oxidative stress, ultimately causing cytotoxic edema.
Gaul et al (2007) reported the case of a woman with no prior headache history who developed a headache fulfilling the ICHD-II criteria for episodic cluster headache during luteal phase support with high-dose progesterone [147]. The attacks ceased upon discontinuation of the treatment.
Psychosocial Aspects and Headache During Fertility Treatment
Only six studies retrieved within our systematic search also assessed psychosocial aspects in the context of headache and fertility treatments, providing preliminary insights.
Five studies investigated pharmacological influence on mental well-being in women undergoing fertility treatment. Two observational studies reported that progesterone, particularly with oral administration [128] and menotropin [150] were associated not only with headache but also with mood-related effects, such as depression or mood changes. Similarly, a randomized comparative study found that intranasal GnRH agonists were linked to both higher rates of headache and depression than subcutaneous administration, despite comparable efficacy and higher plasma levels with subcutaneous administration [151]. In contrast, no differences in psychosocial wellbeing or headache were observed between immediate versus postponed modified natural cycle frozen-thawed embryo transfer, or between treatment with or without vaginal progesterone, although high baseline stress was common [127, 152].
A population-based survey further underscored the role of contextual influences: women in fertility clinics were more likely to live in urban areas, to have private insurance, and to undergo IVF, whereas community-based women often used hormonal treatment or none. Notably, clinic patients reported fewer headaches and less fatigue but higher rates of anxiety disorders [153].
Discussion
This systematic review demonstrates that headache is a frequent but inconsistently reported adverse event across fertility treatments. Available evidence is highly heterogeneous, with multiple treatment classes, dosing protocols, and study populations. Headache rates ranged from rare (<1%) to nearly 50%, depending on the agent and design. Although the FDA and EMA labeling of fertility drugs frequently lists headache, and in some cases migraine as a common adverse event, the clinical trial literature found in our search using the specific search term “headache” remains superficial and inconsistent in its reporting. Almost no study provided standardized or detailed reporting on headache type, severity, or temporal association with treatment phases. Given that headache and migraine are highly prevalent in reproductive-age women, the observed rates in clinical studies likely underestimate the true burden [154].
Several mechanisms may help explain why aromatase inhibitors and GnRH analogues show high headache frequencies in fertility treatment. The action of GnRH analogues is time-dependent: while an initial pulsed or short-term administration produces a transient rise in LH, FSH, and estrogen, continuous administration over several weeks leads to downregulation of pituitary GnRH receptors, resulting in a marked decline in LH, FSH, and ultimately estrogen levels [25]. This estrogen suppression parallels the pharmacological effect of aromatase inhibitors such as letrozole, which also induce rapid and profound reductions in circulating estrogen [155].
The retrospective study by Amir et al (2005) supports this mechanistic link, showing that headaches occurred most frequently during the initial GnRH analogue treatment for pituitary downregulation and again after unsuccessful cycles, another period characterized by estrogen decline [117]. Notably, even women without migraine reported headaches during these phases, suggesting that abrupt hormonal shifts can lower the threshold for headache initiation.
Estrogen withdrawal is a well-established trigger of migraine and may increase susceptibility by modulating trigeminovascular activation, altering serotonergic and CGRP pathways, and influencing vascular reactivity [156].
Gonadotropins have been shown to act directly on endothelial cells through their respective receptors, stimulating endothelial nitric oxide synthase activity and nitric oxide release, which promotes vasodilation. At elevated concentrations, however, FSH may impair endothelial barrier function by altering vascular endothelial cadherin distribution and increasing vascular permeability, potentially compromising vascular stability and contributing to vascular risk [157]. Theories linking endothelial dysfunction and vascular instability may also explain overlapping phenomena between headache and OHSS. Indeed, one retrospective study demonstrated a nearly fivefold increased risk of OHSS among women with a history of migraine, supporting a shared vascular susceptibility, thus underlying causality remains uncertain [148].
Although this review on headache reports in the context of fertility treatment is focused on women, assessing headache in men undergoing treatment is equally important. Male infertility cases involve hypogonadism, a condition characterized by low testosterone production or impaired spermatogenesis. Relative androgen deficiency, especially when accompanied by elevated estradiol levels, has been linked to increased migraine susceptibility in men [158]. Hormone-modulating treatments used in male infertility can shift androgen–estrogen balance and may further influence headache threshold.
Given these endocrine dynamics, men with underlying hypogonadism or altered sex-hormone profiles may be particularly vulnerable to headache or migraine exacerbation during treatment. Monitoring headache in this population is therefore critical, not only to recognize potential adverse effects but also to better understand how sex-hormone regulation influences migraine biology in men [159].
In this systematic review, reports of tumor-related events were limited to isolated case reports. In these cases, a temporal association with fertility treatment was described. However, information on treatment duration and baseline status, including the presence of pre-existing lesions prior to treatment initiation, was often incomplete or unavailable. Accordingly, a causal relationship between fertility treatment and tumor development cannot be established, and these findings should be interpreted with caution.
This review is limited by substantial heterogeneity among the included studies, particularly regarding study design, population characteristics, and treatment regimens. Definitions of headache and reporting standards varied widely, introducing potential reporting bias. Headache as adverse events were typically reported in a non-specific manner, without details regarding its frequency, intensity, or temporal relationship to treatment. The literature search was conducted in two major biomedical databases, PubMed and Embase, which together provide extensive and complementary coverage of clinical, epidemiological, and pharmacological research. Given the emerging nature of this research field, this database selection was considered sufficient to capture the core body of relevant literature. In addition, the FDA and/or EMA drug labelling were manually screened. Nevertheless, it cannot be excluded that relevant publications indexed exclusively in other databases may have been missed, and this should be considered when interpreting the findings.
Conclusion
Available evidence suggests that headache is a clinically relevant but inconsistently reported adverse outcome during fertility treatments. For clinicians, awareness of headache as a side effect of fertility treatment is crucial. Headache may occur in association with hormonal fluctuations, vasoactive effects, or as a manifestation of secondary complications such as OHSS or cerebrovascular events. Individuals with a pre-existing history of migraine may be at increased risk of severe headache during treatment. However, the current evidence is limited and heterogeneous.
The principal value of this systematic review lies in explicitly addressing an underexplored and frequently overlooked clinical outcome in assisted reproduction and in highlighting the paucity of standardized data on headache outcomes. Future trials should systematically evaluate headache, report timing, intensity, and headache type, and consider hormonal, vascular, and psychosocial mediators. Integrating patient-reported outcomes would enhance understanding of the clinical burden of headache in assisted reproduction.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Liu J, Qin Y, Liu H (2025) Global, regional, and national burden of female infertility and trends from 1990 to 2021 with projections to 2050 based on the GBD, 2021 analysis. Sci Rep 15.10.1038/s 41598-025-01498-x PMC 1209260540394053 · doi ↗ · pubmed ↗
- 2Nik Hazlina NH, Norhayati MN, Shaiful Bahari I, Nik Muhammad Arif NA (2022) Worldwide prevalence, risk factors and psychological impact of infertility among women: a systematic review and meta-analysis. BMJ Open 12:e 057132. 10.1136/bmjopen-2021-057132.10.1136/bmjopen-2021-057132 PMC 896864035354629 · doi ↗ · pubmed ↗
- 3Dyer S, Chambers GM, Jwa SC (2025) International Committee for Monitoring assisted reproductive technologies world report: assisted reproductive technology, 2019. Fertil Steril Steril.10.1016/j.fertnstert.2025.06.00340513636 · doi ↗ · pubmed ↗
- 4Mahabbat NA, Khan TA, Elyas MF et al (2024) Role of in vitro fertilization (IVF) in Unexplained infertility management: a systematic review. Cureus. 10.7759/cureus.72527.10.7759/cureus.72527 PMC 1160046439606509 · doi ↗ · pubmed ↗
- 5Siristatidis CS, Yong LN, Maheshwari A, Ray Chaudhuri Bhatta S (2025) Gonadotropin-releasing hormone agonist protocols for pituitary suppression in assisted reproduction. Cochrane Database Syst Rev , 2025. 10.1002/14651858.CD 006919.pub 5.10.1002/14651858.CD 006919.pub 5PMC 1204320139783453 · doi ↗ · pubmed ↗
- 6Cissen M, Bensdorp A, Cohlen BJ et al (2016) Assisted reproductive technologies for male subfertility. Cochrane Database Syst Rev 2016. 10.1002/14651858.CD 000360.pub 5.10.1002/14651858.CD 000360.pub 5PMC 1033536426915339 · doi ↗ · pubmed ↗
- 7U.S. Food and Drug Administration (2004) NOLVADEX® (tamoxifen citrate) Tablets. https://www.accessdata.fda.gov/drugsatfda_docs/label/2005/17970 s 053lbl.pdf. 29 Oct 2025.
- 8U.S. Food and Drug Administration (2007) EVISTA® (raloxifene hydrochloride) tablets. https://www.accessdata.fda.gov/drugsatfda_docs/label/2007/020815 s 018lbl.pdf. 29 Oct 2025.