Nocturnal salivary cortisol and perceived stress in schoolteachers: a pilot study
Pablo A. Lizana, Leandro Gálvez-Ojeda, Alexies Dagnino-Subiabre, Lydia Lera, Ivanka Kuehnel-Carreño, Gerard Clarke, Javier A. Bravo, Marcela Julio-Pieper

TL;DR
This study explores the link between stress and cortisol levels in teachers, finding a connection between perceived stress and nighttime cortisol.
Contribution
The study introduces PM salivary cortisol as a potential objective biomarker for perceived stress in teachers.
Findings
40.7% of teachers showed symptoms of stress, with a significant positive correlation between PM cortisol and perceived stress.
No significant correlations were found between cortisol and depression or anxiety dimensions.
The study supports integrating psychological and physiological measures for teacher stress monitoring.
Abstract
Teaching is characterized by high exposure to occupational stressors that negatively impact the mental health of education professionals. In this context, the present cross-sectional study aimed to analyze the relationship between salivary cortisol levels and perceived stress in a sample of teachers. Subjective stress perception was assessed using the DASS-21 questionnaire, while salivary cortisol samples were collected by the participants themselves before bedtime (PM cortisol). To examine the relationship between cortisol concentrations and the DASS-21 dimensions (depression, anxiety, and stress), non-parametric correlation analyses were applied. Results showed that 18.5% of teachers exhibited symptoms of depression, 59.3% anxiety, and 40.7% stress. Moreover, a significant positive correlation was observed between PM salivary cortisol levels and the perceived stress dimension (Rho =…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
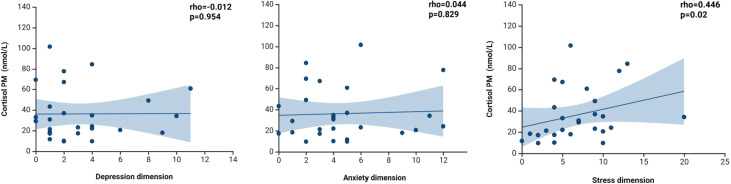 Figure 1
Figure 1| Variables | Mean | SD | Inferior CI95% | Inferior CI95% |
|---|---|---|---|---|
| Age (years) | 39.63 | 14.38 | 33.94 | 45.32 |
| Depression | 3.22 | 3.08 | 2.00 | 4.44 |
| Anxiety | 4.63 | 3.44 | 3.27 | 5.99 |
| Stress | 6.89 | 4.33 | 5.18 | 8.60 |
| Cortisol PM nmol/L | 36.2 | 25.1 | 26.2 | 46.1 |
| Dimension | Categories | n | % |
|---|---|---|---|
| Depression | None | 22 | 81.5 |
| Mild | 1 | 3.7 | |
| Moderate | 3 | 11.1 | |
| Severe | 1 | 3.7 | |
| Extremely severe | 0 | 0 | |
| Anxiety | None | 11 | 40.7 |
| Mild | 5 | 18.5 | |
| Moderate | 6 | 22.2 | |
| Severe | 1 | 3.7 | |
| Extremely severe | 4 | 14.8 | |
| Stress | None | 16 | 59.3 |
| Mild | 4 | 14.8 | |
| Moderate | 5 | 18.5 | |
| Severe | 1 | 3.7 | |
| Extremely severe | 1 | 3.7 |
- —Vicerrectoría de Investigación, Creación e Innovación10.13039/501100024579
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsStress Responses and Cortisol · Stress and Burnout Research · Psychological Treatments and Assessments
Introduction
Teaching has been reported as one of the most stressful professions worldwide (1, 2). Various studies have demonstrated that occupational stress is a common phenomenon in the educational field, affecting both the physical and mental health of teachers (3, 4) and often leading to burnout (5). This negative impact can manifest in the development of psychological disorders and the deterioration of professional performance (6). In this context, teacher health and well-being emerge as key factors that directly influence the quality of the teaching-learning process and job satisfaction (7, 8). Conceptually, occupational stress can be framed as a process that differentiates between exposure to work-related stressors (objective demands and contextual conditions) and the individual’s appraisal of those demands (perceived stress severity and controllability). This distinction is central because individuals facing similar objective demands may report markedly different perceived stress, with downstream consequences for health and functioning (9, 10).
From a biopsychosocial perspective, stress-related appraisals are expected to shape neuroendocrine activation, including hypothalamic–pituitary–adrenal (HPA) axis responding, thereby providing a rationale for integrating self-report measures with physiological indicators such as cortisol (11, 12). Chronic stress exposure can produce cumulative multisystem physiological strain, commonly conceptualized as allostatic load, and may progress to allostatic overload when adaptive systems are persistently challenged beyond regulatory capacity (13). Mechanistically, repeated activation of stress-response systems coupled with insufficient recovery can accumulate across time, increasing allostatic load; this is particularly relevant for teachers given the daily, recurring nature of classroom and administrative demands and the frequent extension of work into the evening (14–17). In educators, this type of stress represents a constant challenge that affects both professional performance and classroom climate (18). Teachers often experience high levels of stress due to multiple factors, including pressure to meet academic standards, classroom behavior management, administrative workload, lack of resources, and limited institutional support (19). Those reporting higher levels of occupational stress tend to exhibit lower job satisfaction and commitment, higher intention to leave the profession, and reduced capacity to provide emotional and academic support to their students (20). Accordingly, persistent occupational demands may contribute to allostatic load over time, a mechanism of “wear and tear” that is relevant for teachers given the sustained, repetitive nature of work stressors across the academic year (13, 21). Therefore, understanding the interaction between perceived stress and physiological responses is essential for designing effective monitoring and intervention strategies that promote teacher well-being. In this framework, salivary cortisol emerges as an objective and non-invasive biomarker that allows the assessment of hypothalamic–pituitary–adrenal (HPA) axis activity, the body’s main stress response system (22–24). Measuring cortisol levels in saliva is a valuable tool to understand how perceived stress relates to physiological stress-related activity, facilitating the identification of teachers at risk of developing health alterations associated with chronic stress (25). Moreover, nocturnal salivary cortisol has been proposed as a useful non-invasive marker for assessing hypercholesterolemia in different populations (26, 27).
Although associations between perceived stress and cortisol have been examined across multiple populations, less attention has been paid to nocturnal salivary cortisol (pre-bedtime), despite its relevance as an index of end-of-day HPA-axis downregulation and recovery (28). Importantly, perceived stress may be more proximally linked to end-of-day physiological activation than objective exposure alone, because it captures the subjective intensity and ongoing cognitive-emotional engagement with occupational demands, which can interfere with recovery processes (11, 12). Cortisol levels assessed near an individual’s habitual bedtime may capture sustained physiological activation during the transition to sleep, a period that is particularly sensitive to prolonged work-related demands and has been linked to sleep-related hyperarousal (29, 30). In schoolteachers, work often extends into the evening (e.g., grading and lesson preparation), making bedtime cortisol a theoretically meaningful and practically feasible biomarker for field-based occupational surveillance (31). Given these conceptual and methodological considerations, a pilot field design is appropriate to test the feasibility of bedtime sampling under real school conditions and to generate preliminary estimates of association that can guide adequately powered future studies. Therefore, the aim of the present study was to analyze the relationship between nocturnal salivary cortisol levels and perceived stress in teachers through a cross-sectional study conducted in school settings to evaluate the utility and feasibility of bedtime salivary cortisol as an end-of-day biomarker of stress-related HPA activity in schoolteachers.
Methodology
The study employed a pilot field and cross-sectional design in school settings to examine the association between perceived stress and pre-bedtime salivary cortisol under real-world conditions. Participant selection was conducted using a non-probabilistic sampling method, aiming to ensure sample representativeness in terms of gender. Two primary instruments were used for data collection: a perceived stress questionnaire and salivary cortisol measurement. The Depression, Anxiety, and Stress Scale (DASS-21) was applied to assess teachers’ subjective perception in the dimensions of depression, anxiety, and stress. This 21-item self-administered instrument has been validated in Chile (32) and previously used in Chilean schoolteacher populations (4). The DASS-21 comprises three subscales evaluating negative emotional states of depression, anxiety, and stress, each with seven items and four-point Likert response options (0 = “Did not apply to me at all” to 3 = “Applied to me very much or most of the time”). Symptom level classification used cut-off points proposed by Lovibond & Lovibond (33), defining the ranges as: no symptoms, mild, moderate, severe, and extremely severe (4, 34). Internal consistency of the DASS-21 dimensions was evaluated using Cronbach’s alpha coefficient, with values ≥ 0.70 considered acceptable (35).
Saliva samples were collected by participants themselves before bedtime using Salivette devices (Sarstedt, Germany). Participants were allowed to follow their normal bedtime patterns, however they were instructed to avoid eating or drinking during the 15 minutes prior to sample collection and not to brush their teeth at least one hour before. Once obtained, samples were immediately stored at 4 °C until collected by the research team. Saliva was then extracted by centrifugation at 1000 g for 5 minutes and stored at –20 °C. Salivary cortisol concentrations were determined by ELISA (ALPCO, USA), following the manufacturer’s instructions. The assay detection limit was 0.128 nmol/mL, with intra-assay and inter-assay coefficients of variation of 4.7% and 6.9%, respectively. Samples were diluted 1:2 in assay buffer and analyzed in duplicate; only results with variability below 10% between duplicates were considered. Analyses were repeated up to a third time when variability was higher than 10%. Results were expressed in nmol/L, using <6 nmol/L as the cut-off point for nocturnal salivary cortisol (36).
Statistical analysis was conducted using STATA 16 for Windows. Data normality was assessed using the Shapiro–Wilk test. To analyze the relationship between salivary cortisol levels and the DASS-21 dimensions (depression, anxiety, and stress), Spearman correlation was used due to non-normal distribution of the variables. In addition, a sensitivity analysis was performed for extreme data. For the stress dimension, the correlation analysis was performed without the extreme data point (DASS-21 stress score = 20).
Results
A total of 31 teachers were recruited, of whom 4 were excluded due to differences greater than 10% between duplicates in salivary cortisol measurement. Therefore, 27 participants were included in the analysis, of which 85.2% (n = 23) were women, with a mean age of 39.6 ± 14.4 years. The internal consistency of the DASS-21 was adequate, with Cronbach’s alpha values of 0.79 for depression, 0.78 for anxiety, and 0.85 for stress. The average scores of the DASS-21 dimensions (Table 1) indicated that teachers, on average, were classified in the “no symptoms” category for depression, “mild” for anxiety, and “no symptoms” for stress. However, analysis of individual category distribution (Table 2) showed that 18.5% of schoolteachers presented symptoms of possible depression, 59.3% anxiety, and 40.7% stress.
Regarding PM salivary cortisol, the mean level was 36.2 nmol/L, and no participant presented values within the normal range (<6 nmol/L). Spearman correlation between cortisol levels and DASS-21 dimensions is shown in Figure 1. Results revealed a significant positive correlation between PM salivary cortisol and perceived stress (Rho = 0.446, p < 0.05). In addition, an extreme value was observed in the stress dimension (DASS-21 stress score = 20). For the extreme value, a correlation analysis was performed without it, and the correlation remained statistically significant removal of the extreme value (ρ = 0.449, p = 0.021). No significant correlations were observed between cortisol levels and the dimensions of depression or anxiety.
Correlation between post meridiem salivary cortisol and depression, anxiety, and stress dimensions.
Discussion
Research on teacher stress and its relationship with biological markers such as cortisol is essential for understanding the underlying mechanisms of mental health problems affecting education professionals. The positive correlation observed between PM salivary cortisol levels and perceived stress suggests a direct connection between subjective stress perception and the activation of the hypothalamic–pituitary–adrenal (HPA) axis, the primary stress response system (37). On the other hand, the absence of significant correlations between cortisol and the depression and anxiety dimensions indicates that perceived stress, measured through the DASS-21, captures a specific facet of teachers’ emotional experience, more closely related to the physiological stress response (38). This reinforces the utility of the DASS-21 as a monitoring tool for stress in this population (39, 40) although we acknowledge it is not a clinical instrument for diagnoses.
It is noteworthy that all teachers in the study presented PM cortisol levels above the established cutoff and although there is currently no consensus on the clinical relevance of this salivary analyte, the results do highlight that occupational stressors in the educational setting manifest in abnormal stress physiology and suggest that strategies to mitigate this adverse impact should be considered (41). The unusually high cortisol levels shown by the participants in the present study could represent a regional characteristic of Chilean schoolteachers, but we cannot confirm this without a description of baseline salivary cortisol levels at bedtime in the general Chilean population. Although the sample is small, these results align with previous research reporting a high prevalence of stress among teachers (4, 42, 43). The nature of teaching, characterized by high demands and multiple roles, explains why this population experiences elevated occupational stress levels (44). Recent studies also indicate that a considerable proportion of teachers report chronic stress, associated with physical and mental health problems (3, 45). In Chile, teachers’ mental health has systematically deteriorated in recent years (4, 46).
The DASS-21 scale is a reliable tool for assessing mental health in diverse contexts (4, 47). While Its validity and reliability in non-clinical samples and among teachers have been widely demonstrated, it is not a diagnostic clinical instrument (48, 49). Although average scores indicated mild or absent symptoms, individual analysis revealed a significant prevalence of depression, anxiety, and stress, highlighting the need for a detailed analysis of clinical categories. Early recognition of stress and the development of coping skills are essential to promote teachers’ health and well-being, positively impacting their performance and educational quality (50). Conversely, chronic exposure to stress and elevated cortisol levels has been associated with cardiovascular deterioration and neurodegeneration (51, 52).
Our results suggest that the stress dimension of the DASS-21 is a promising instrument for detecting and monitoring teacher stress, facilitating the implementation of timely intervention strategies. Study limitations include its cross-sectional design, which prevents establishing definitive causal relationships, and the non-probabilistic sampling, which could limit the generalizability of the findings. Additionally, the relatively small effective sample size for correlation analyses (n = 27) may have limited statistical power, increasing the risk of type II errors for small-to-moderate correlations. Therefore, the observed association between bedtime salivatory cortisol and perceived stress (Spearman’s ρ = 0.45; p < 0.05) should be interpreted as exploratory and warrants replication in larger samples. In this sense, as a pilot field study, a wide age range, and an uneven sex distribution, we were unable to formally assess the influence of age and sex on pre-bedtime salivary cortisol variability; therefore, residual confounding or effect modification by these factors cannot be ruled out and should be addressed in the future, adequately powered and sex-balanced studies. Moreover, the collection of cortisol at a single time point (before bedtime) does not capture the full circadian dynamics of the HPA axis. Furthermore, the exclusive use of the DASS-21 may not encompass all specific occupational stressors, such as workload or organizational climate (6, 7). Despite these limitations, the study contributes significantly to understanding the relationship between perceived stress and physiological biomarkers in the educational context.
Conclusion
The present study demonstrates a significant association between perceived stress and PM salivary cortisol levels in teachers, indicating that the subjective perception of stress is reflected in a measurable physiological response. These findings highlight the need to address teacher stress through prevention, monitoring, and intervention strategies that consider both psychological and physiological aspects, in order to promote health and well-being within the educational setting.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Smith A Brice C Collins A Matthews V Mc Namara R . The scale of occupational stress: a further analysis of the impact of demographic factors and type of job. London: HSE Books (2000). Contract Research Report 311/2000.
- 2Nwoko JC Emeto TI Malau-Aduli AEO Malau-Aduli BS . A systematic review of the factors that influence teachers’ occupational wellbeing. Int J Environ Res Public Health. (2023) 20:6070. doi: 10.3390/ijerph 20126070, PMID: 37372657 PMC 10298565 · doi ↗ · pubmed ↗
- 3Lizana PA Vega-Fernández G Gómez-Bruton A Leyton B Lera L . Impact of the COVID-19 pandemic on teacher quality of life: a longitudinal study from before and during the health crisis. Int J Environ Res Public Health. (2021) 18:3764. doi: 10.3390/ijerph 18073764, PMID: 33916544 PMC 8038473 · doi ↗ · pubmed ↗
- 4Lizana PA Lera L . Depression, anxiety, and stress among teachers during the second COVID-19 wave. Int J Environ Res Public Health. (2022) 19:5968. doi: 10.3390/ijerph 19105968, PMID: 35627505 PMC 9140393 · doi ↗ · pubmed ↗
- 5Sohail MM Baghdady A Choi J Huynh HV Whetten K Proeschold-Bell RJ . Factors influencing teacher wellbeing and burnout in schools: a scoping review. Work. (2023) 76:1317–31. doi: 10.3233/WOR-220234, PMID: 37393465 · doi ↗ · pubmed ↗
- 6Mijakoski D Cheptea D Marca SC Shoman Y ÇağlayanÇ Bugge M . Determinants of burnout among teachers: a systematic review of longitudinal studies. Int J Environ Res Public Health. (2022) 19:5776. doi: 10.3390/ijerph 19095776, PMID: 35565168 PMC 9104901 · doi ↗ · pubmed ↗
- 7Lazcano C Galilea S Wenderoth S Solares Rojas A Ortúzar MS . Exploring teacher job satisfaction in five Latin American countries: a multi-level analysis using TALIS 2018. Int J Educ Res Open. (2025) 9:100516. doi: 10.1016/j.ijedro.2025.100516, PMID: 41783259 · doi ↗
- 8Castells RR Lumbierres C Boix J-L Martínez Cano S de Andres C Jové Monclús G . Study on teaching staff’s welfare indicators in secondary school teachers. Cult Educ. (2008) 20:347–56. doi: 10.1174/113564008785826376, PMID: 25131292 · doi ↗