Fluorescence-guided ureter mapping in colorectal surgery: a systematic review of intraureteral ICG and emerging renal fluorophores
Alexis Litchinko, Quentin Denost, Barbara Noiret, Frederic Ris, Michel Adamina

TL;DR
This paper reviews how fluorescence imaging using dyes like ICG can help surgeons better see the ureters during colorectal surgery, reducing injury risks.
Contribution
The study systematically evaluates the effectiveness of ICG and new fluorophores for ureter identification in colorectal surgery.
Findings
ICG fluorescence achieved ureter visualization rates of 95.3% to 100% with no major complications.
Cystoscopy for ICG administration added 7 to 29 minutes to procedure time.
Emerging renally excreted fluorophores may eliminate the need for ureteral catheterization.
Abstract
Ureteral injury is a severe complication in colorectal surgery, with an incidence up to 2.5%. Despite meticulous surgical technique, intraoperative ureter identification can be challenging, particularly in cases involving prior operations or extensive inflammation. Indocyanine green (ICG) fluorescence imaging has emerged as a promising adjunct to enhance ureter visualization. In parallel, novel fluorophores with renal excretion properties (e.g., CW800-CA, ZW800-1) are undergoing investigation to avoid routine ureteral catheterization. This systematic review evaluates the efficacy, safety, and clinical impact of ICG-based and emerging fluorescence approaches for ureter identification in colorectal surgery. A systematic literature search was performed in PubMed and Embase, up to March 2025, following PRISMA 2020 guidelines. Studies assessing intraoperative ureter identification via ICG…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
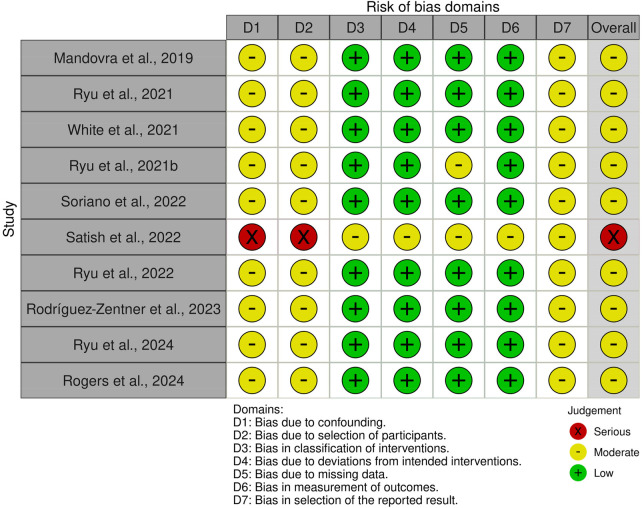 Figure 1
Figure 1|
|
| Reference | Year | Country | Study type | Number of patients with ICG | ICG administration method | wUreteral stent use |
|---|---|---|---|---|---|---|
| Mandovra et al. ( | 2019 | India | Retrospective cohort | 30 | Intra-ureteral injection of 5 mg ICG diluted in 2 ml of distilled water | No |
| Ryu et al. ( | 2021 | Japan | Retrospective case series | 11 | Intravenous & intra-ureteral injection of ICG for ureter and vessel navigation | Yes |
| White et al. ( | 2021 | USA | Retrospective case series | 16 | Direct intra-ureteral injection of 4 mg ICG in 4 ml NaCl | No |
| Ryu et al. ( | 2021 | Japan | Pilot study | 20 | Near-Infrared Fluorescent Ureteral Catheter (NIRFUC) | Yes |
| Soriano et al. ( | 2022 | USA | Prospective cohort | 83 | Intra-ureteral injection of 5 ml ICG (2.5 mg/ml) | 20 with stent |
| Satish et al. ( | 2022 | India | Case reports | 2 | Cystoscopic retrograde injection of 2.5 mg ICG per ureter | Yes |
| Ryu et al. ( | 2022 | Japan | Cohort comparative study | 122 | Near-Infrared Fluorescent Ureteral Catheter (NIRFUC) | Yes |
| Rodriguez-Zentner et al. ( | 2023 | Panama | Case series | 30 | Intra-ureteral injection of ICG | Yes |
| Ryu et al. ( | 2024 | Japan | Retrospective study | 141 | Near-Infrared Fluorescent Ureteral Catheter (NIRFUC) | Yes |
| Rogers et al. ( | 2024 | USA | Retrospective comparative cohort | 312 | Injection of 5 ml ICG solution (2.5 mg/ml) per ureter | Yes |
| Reference | Year | Surgical Indications (included/studied) | Surgical Procedures | Vizualisation Success rate | Mean Cystoscopic Procedure Duration (minutes) | ICG-Related Complications |
|---|---|---|---|---|---|---|
| Mandovra et al. ( | 2019 | Various colorectal indications (30/30) | Laparoscopic colorectal procedures (30) | 100% | 7 | None |
| Ryu et al. ( | 2021 | Various colorectal indications (11/14) | Laparoscopic colorectal procedures (11) | 100% | 14 | None |
| White et al. ( | 2021 | Various colorectal indications (16/16) | Laparoscopic colorectal surgery (16) | 94% | 11.5 | None |
| Ryu et al. ( | 2021 | Various colorectal indications (20/20) | Laparoscopic colorectal surgery (20) | 100% | Unknow | None |
| Soriano et al. ( | 2022 | Diverticulitis (43), Colorectal cancer (30), Other (10) | Robot-assisted left colectomy (45), Sigmoidectomy (38) | 97% right ureter | 4 without stent place-Ment | None |
| Satish et al. ( | 2022 | Rectal cancer (2) | Low anterior resection (1), Hartmann's procedure (1) | 100% | Unknowm | None |
| Ryu et al. ( | 2022 | T4 colorectal cancers (122/122) | Laparoscopic colorectal resection (122) | 100% | Unknown | None |
| Rodriguez-Zentner et al. ( | 2023 | Colorectal cancer cases (30/30) | Laparoscopic colorectal procedures (30) | 100% | 22.4 | None |
| Ryu et al. ( | 2024 | Colorectal cancer and colorectal cancer recurrence (141/141) | Laparoscopic colorectal procedures (141) | 100% | 12 | None |
| Rogers et al. ( | 2024 | Colorectal cancer and Diverticulitis (556/312) | Laparoscopic colectomy (100), Robot-assisted (456) | 95.3% | 29 | None |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsUreteral procedures and complications · Bladder and Urothelial Cancer Treatments · Pediatric Urology and Nephrology Studies
Introduction
1
Ureteral injury is a rare but serious complication of colorectal surgery, particularly during pelvic resections, with an incidence reaching up to 2.5% (1–3). These injuries are often missed intraoperatively and can lead to significant postoperative morbidity, including renal dysfunction, ureteral strictures, reinterventions, and, in severe cases, nephrectomy (4). Accurate intraoperative identification of the ureters is therefore essential to prevent iatrogenic damage, especially in anatomically complex cases such as inflammatory bowel disease, extensive adhesions, or locally advanced malignancies.
Traditional strategies, such as preoperative ureteral stenting or intraoperative palpation, have been widely used to aid in ureter identification. While effective in open procedures, these methods are limited in minimally invasive surgery, where tactile feedback is reduced. Routine ureteral catheterization also adds procedural time and carries its own risks, including mucosal trauma, urinary tract infections, and transient hematuria (5, 6). Despite these precautions, ureteral injuries may still occur, underscoring the need for more reliable, real-time visualization tools.
Fluorescence-guided imaging has emerged as a novel adjunct to improve intraoperative navigation. Indocyanine green (ICG) fluorescence, in particular, has demonstrated clinical utility across multiple surgical disciplines, including hepatobiliary, vascular, and colorectal surgery. When administered intraureterally, ICG binds to the urothelium and enables real-time visualization of the ureters under near-infrared fluorescence (NIRF) imaging systems (7, 8). This technique offers a potential alternative to prophylactic stenting by enhancing anatomical delineation without the drawbacks associated with prolonged ureteral catheterization.
Despite increasing clinical adoption, the efficacy and utility of ICG fluorescence for ureter identification in colorectal surgery remain subjects of debate. The available evidence is largely derived from small, heterogeneous studies, often with variations in administration technique, imaging platforms, and outcome measures. Additionally, concerns have been raised regarding the procedural complexity of intraureteral dye instillation and its impact on operative workflow (1, 7). Intravenous ICG delivery has been proposed as a simpler method, though its renal clearance is minimal, limiting its effectiveness for direct ureter visualization. Meanwhile, newer renally excreted fluorophores such as CW800-CA and ZW800-1 are being explored in preclinical models and early clinical trials, offering the promise of ureter mapping without the need for catheterization (9–11).
This systematic review aims to synthesize current clinical evidence regarding ICG fluorescence imaging for intraoperative ureteral identification in colorectal surgery. By evaluating efficacy, safety, and procedural considerations, this review seeks to determine whether fluorescence guidance constitutes a viable alternative to traditional techniques and to highlight directions for future research and technological innovation.
Materials and methods
2
Study design and registration
2.1
This systematic review was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2020 guidelines to ensure methodological rigor and transparency. The study protocol was registered in PROSPERO (Registration ID: CRD420250653992) before the initiation of the literature search (12).
Search strategy
2.2
A systematic literature search was conducted in PubMed and Embase, library to identify studies evaluating the use of indocyanine green (ICG) fluorescence imaging for intraoperative ureter identification in colorectal surgery. The search strategy incorporated a combination of Medical Subject Headings (MeSH), Emtree terms, and free-text keywords related to ICG fluorescence, ureter identification, and colorectal surgery. Boolean operators were used to optimize sensitivity and specificity. The search was restricted to studies published between 2015 and February 2025, with language filters applied to include only articles in English and French. Additional relevant studies were identified by manually screening the reference lists of included articles.
Eligibility criteria
2.3
Studies were selected according to predefined inclusion and exclusion criteria based on the Population, Intervention, Comparison, Outcome, and Study Design (PICOS) framework (13). Eligible studies included those involving adult (>18 yo) patients undergoing colorectal surgery in which ICG fluorescence was used for intraoperative ureter visualization and iatrogenic prevention. Primary outcomes assessed were the efficacy of ICG in ureteral identification and the incidence of intraoperative ureteral injuries. Secondary outcomes included operative time, procedure-related complications, adverse events, and exploratory preliminary cost considerations related to ureteral catheterization and operative workflow, when reported. Studies focusing on pediatric populations, non-colorectal procedures, animal models, or experimental techniques not yet applied in clinical practice were excluded. Review articles, editorials, conference abstracts without full-text availability, and opinion pieces were also excluded.
Study selection and data extraction
2.4
Two independent reviewers screened and selected the studies according to the predefined eligibility criteria (A.L. & B.N.). Titles and abstracts were first reviewed to exclude irrelevant studies, followed by a full-text assessment of potentially eligible articles. Disagreements between reviewers were resolved by discussion or, if necessary, by consulting a third reviewer. Data extraction was performed using a standardized collection form, including study characteristics, patient demographics, surgical indications, ICG administration protocols, fluorescence detection techniques, and reported outcomes.
Quality assessment and data synthesis
2.5
The quality of included studies was assessed using the ROBINS-I tool for non-randomized studies (14). The level of evidence was evaluated using the Grading of Recommendations, Assessment, Development, and Evaluations (GRADE) approach (15). Due to the heterogeneity of study designs, patient populations, and ICG administration protocols, a narrative synthesis was performed instead of a meta-analysis. This approach allows for a qualitative assessment of trends and clinical implications across different studies.
Ethical considerations
2.6
This study is a secondary analysis of previously published data and did not require institutional review board approval. No external funding was received, and no conflicts of interest were reported by the authors.
Results
3
Study selection
3.1
The systematic search yielded 318 studies after duplicate removal. Following title and abstract screening, 45 full-text articles were assessed for eligibility. Among them, 10 studies met the inclusion criteria and were included in the final qualitative synthesis. The PRISMA flow diagram (Table 1) illustrates the study selection process.
Study characteristics
3.2
The 10 included studies were published between 2019 and 2024. Study populations ranged from 2 to 312 patients. Indocyanine green (ICG) was administered intraureterally in most studies, primarily via cystoscopic retrograde injection or direct intraureteral instillation. Three studies used Near-Infrared Fluorescent Ureteral Catheters (NIRFUC), which rely on catheter-based fluorescence rather than dye instillation. Most studies reported bilateral intraureteral ICG administration to ensure symmetrical visualization, particularly in complex pelvic dissections. Ureteral stents were systematically used in 60% of the studies, selectively used in 10%, and not used in 30%. Most procedures were minimally invasive with laparoscopic (58%), followed by robot-assisted colorectal surgery (42%).
Primary outcomes
3.3
Ureteral visualization rate
3.3.1
Fluorescence imaging was predominantly performed using near-infrared platforms. The ureteral visualization success rate with ICG fluorescence was consistently high across studies, ranging from 95.3% to 100%. Overall, 80% of the included studies reported complete visualization of both ureters. Indocyanine green was predominantly administered via intraureteral injection, in association with high visualization rates. Comparative effectiveness based on surgical approaches (laparoscopic vs. robot-assisted) was not clearly quantified; however, robotic procedures benefited from enhanced NIR imaging capabilities provided by technologies such as Firefly®. A detailed summary of study characteristics and ICG administration protocols is presented in Table 2.
Ureteral injury rate
3.3.2
The incidence of intraoperative ureteral injury was low across studies using ICG fluorescence, although comparative data were limited. In studies reporting comparative outcomes, lower ureteral injury rates were observed with ICG fluorescence compared with conventional visualization in high-risk surgical settings (3.2% vs. 7.8%, p < 0.05). No ICG-related adverse events were reported. Lower ureteral injury rates were primarily reported in cohorts including patients with prior pelvic surgery, advanced malignancy, or inflammatory bowel disease.
Secondary outcomes
3.4
Procedure-related complications & operative time
3.4.1
The most frequently reported complications were related to cystoscopy itself. Indeed, transient hematuria, occurring in 5.4% of patients receiving intraureteral ICG administration. Other minor complications included dysuria (2.5%) and urinary tract infections (1.8%). No adverse events related to ICG administration were reported across the studies. Intraureteral administration of ICG via cystoscopic catheterization increased operative time by an average of 7–29 min across studies. No studies evaluating intravenous ICG administration were included. Thus, no comparison of operative time or visualization rates between intraureteral and intravenous ICG routes or simple ureteral stent could be performed. None of the included studies specifically investigated the use of renally excreted fluorophores (CW800-CA, ZW800-1, or ICG derivatives). Therefore, no conclusions can currently be drawn regarding their efficacy or safety in colorectal surgery. Further studies are required to evaluate the potential of these fluorophores for intraoperative ureter visualization without catheterization (Table 3).
Quality assessment and risk of bias
3.5
The risk of bias for the included studies was assessed using the ROBINS-I tool for observational studies. Among the 10 studies evaluated, 9 were observational studies (retrospective or prospective cohorts and case series), and 1 was a pilot study (16). Most of these studies (7 out of 10) were classified as having a moderate risk of bias, primarily due to heterogeneity in the fluorescence imaging protocols, variability in patient selection criteria, and the absence of comparator groups. No randomized controlled trials were included in this review. According to the GRADE approach, the level of evidence supporting the efficacy of ICG fluorescence for ureter identification in colorectal surgery was moderate. Evidence regarding cost-effectiveness was insufficient and remains very limited. All included studies were observational, and none were randomized; most had a moderate risk of bias based on ROBINS-I assessment (Figure 1).
Quality assessment and risk of bias (ROBINS-I).
Discussion
4
Clinical benefits of ICG fluorescence
4.1
Ureteral injury, though rare in colorectal surgery, carries significant morbidity, particularly in complex pelvic dissections. Indocyanine green (ICG) fluorescence provides real-time, high-contrast ureter visualization, especially valuable in minimally invasive procedures where tactile feedback is absent. Across 10 studies (716 patients), intraureteral ICG achieved visualization rates of 95.3%–100% (pooled mean 98.4%), with 80% of studies reporting complete bilateral delineation. Comparative data suggest lower ureteral injury rates with ICG (3.2% vs. 7.8%, p < 0.05) in high-risk cases, although derived from observational comparative data. Protocol heterogeneity—dose, timing, stenting strategy, and imaging platform—limits comparability, but safety was consistently high, with no ICG-specific toxicity and only minor cystoscopy-related events (e.g., transient hematuria, 5.4%). The main drawback is the additional 7–29 min required for catheter placement.
Limitations and barriers
4.2
Catheter-based intraureteral instillation remains the standard delivery method, prolonging surgery and requiring cystoscopic access. Protocol variation (ICG 0.25–5 mg, pre- vs. intraoperative) and differences in surgical approach and imaging systems complicate pooled interpretation. All studies were observational with moderate risk of bias, as no randomized controlled trials exist (5). While robotic platforms (e.g., Firefly®) may enhance imaging, they are not universally available, particularly in lower-resource settings. Also, routine bilateral catheterization may expose the contralateral ureter, sometimes not directly involved in the dissection, to unnecessary manipulation, with a theoretical risk of ureteral injury or urinary complications. This aspect should be addressed in future protocols.
Future directions and emerging technologies
4.3
Renally excreted near-infrared (NIR) fluorophores constitute a major technological advancement, designed to enable real-time ureteral mapping following intravenous administration, thereby overcoming the logistical limitations of catheter-based delivery. Unlike ICG, which is hepatically cleared, agents such as CW800-CA, ZW800-1, and IRDye 800BK are eliminated via the kidneys, allowing intravenous administration and passive urinary tract accumulation (9–11, 17–19).
ZW800-1: A zwitterionic dye with minimal non-specific binding, providing a high signal-to-background ratio. Detectable in ureters within 10 min of injection, with signal persisting up to 60 min. CW800-CA: PEGylated cyanine dye with excellent renal clearance and stable fluorescence; shows greater signal stability but slower onset than ZW800-1.
In terms of kinetic, ZW800-1 peaks faster but fades sooner, whereas CW800-CA provides prolonged stability—properties that may guide selection based on operative duration. These agents could eliminate cystoscopy, streamline workflow, and reduce complications. However, they remain investigational, with no large-scale RCTs, incomplete dosing standardization, and pending regulatory approval. Importantly, dual-agent fluorescence—for example, ICG for bowel perfusion plus ZW800-1 for ureter mapping—offers the possibility of simultaneous vascular and urinary tract visualization without procedural delays (18, 20).
Economic considerations
4.4
Future cost-effectiveness analyses integrating both direct expenditures and potential savings from injury prevention will be essential to support reimbursement and guideline integration (21–23). Contemporary ICG-based protocols frequently rely on cystoscopy-guided ureteral catheterization, entailing direct procedural expenditures ranging from approximately 300–800 CHF per case. Beyond these immediate costs, such approaches necessitate additional anesthesia and urology team involvement, thereby increasing operative time and resource utilization. Moreover, potential downstream expenses may arise from cystoscopy-related adverse events, further challenging the overall cost-effectiveness of the technique. The 7–29 min procedural delay may reduce operating room throughput, particularly in high-volume centers. IV-administered renally excreted fluorophores could remove these bottlenecks, but their cost-effectiveness remains unproven without formal economic modeling. Importantly, cost data were heterogeneous, indirect, and not derived from formal economic evaluations, precluding definitive cost-effectiveness conclusions.
Future studies should evaluate direct expenditures (dye, equipment, OR time) alongside indirect savings from prevented injuries, shorter hospital stays, and avoidance of litigation. This evidence will be essential to inform reimbursement, purchasing decisions, and guideline integration.
Conclusion
5
ICG fluorescence represents a safe and effective adjunct for intraoperative ureteral identification, achieving visualization rates above 95% across studies with negligible dye-related complications. Its main limitations—catheter dependence, protocol heterogeneity, and lack of randomized evidence—currently restrict widespread adoption. Emerging intravenously administered, renally excreted NIR fluorophores hold the potential to simplify workflow and expand access to fluorescence-guided surgery. Multicenter randomized trials integrating clinical, economic, and workflow outcomes are warranted to define the optimal strategy for intraoperative ureter mapping in colorectal surgery.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Halabi WJ Jafari MD Nguyen VQ Carmichael JC Mills S Pigazzi A Ureteral injuries in colorectal surgery: an analysis of trends, outcomes, and risk factors over a 10-year period in the United States. Dis Colon Rectum. (2014) 57(2):179–86. 10.1097/DCR.000000000000003324401879 · doi ↗ · pubmed ↗
- 2Mc Carus S Alexandre AF Kimura T Feng Q Han W Shortridge EF Abdominopelvic surgery: intraoperative ureteral injury and prophylaxis in the United States, 2015–2019. Adv Ther. (2023) 40(7):3169–85. 10.1007/s 12325-023-02515-z 37227585 PMC 10272259 · doi ↗ · pubmed ↗
- 3Souli A Alves A Tillou X Menahem B. Iatrogenic ureteral injury: what should the digestive surgeon know? J Visc Surg. (2024) 161(1):6–14. 10.1016/j.jviscsurg.2023.04.00138242812 · doi ↗ · pubmed ↗
- 4de'Angelis N Schena CA Marchegiani F Reitano E De Simone B Wong GYM 2023 WSES guidelines for the prevention, detection, and management of iatrogenic urinary tract injuries (IUT Is) during emergency digestive surgery. World J Emerg Surg. (2023) 18(1):45. 10.1186/s 13017-023-00513-837689688 PMC 10492308 · doi ↗ · pubmed ↗
- 5Hird AE Nica A Coburn NG Kulkarni GS Nam RK Gien LT. Does prophylactic ureteric stenting at the time of colorectal surgery reduce the risk of ureteric injury? A systematic review and meta-analysis. Colorectal Dis. (2021) 23(5):1060–70. 10.1111/codi.1549833340227 · doi ↗ · pubmed ↗
- 6Coakley KM Kasten KR Sims SM Prasad T Heniford BT Davis BR. Prophylactic ureteral catheters for colectomy: a national surgical quality improvement program-based analysis. Dis Colon Rectum. (2018) 61(1):84–8. 10.1097/DCR.000000000000097629215477 · doi ↗ · pubmed ↗
- 7Garoufalia Z Wexner SD. Indocyanine green fluorescence guided surgery in colorectal surgery. J Clin Med. (2023) 12(2):494. 10.3390/jcm 1202049436675423 PMC 9865296 · doi ↗ · pubmed ↗
- 8Rogers P Dourado J Wignakumar A Weiss B Aeschbacher P Garoufalia Z The role of ureteric indocyanine green fluorescence in colorectal surgery: a retrospective cohort study. Tech Coloproctol. (2024) 28(1):83. 10.1007/s 10151-024-02955-x 38985353 PMC 11236861 · doi ↗ · pubmed ↗