Sexual Dimorphism in Renal Progenitors: Do Immunosuppressants Erase the Female Advantage?
Zeynep Ural

Abstract
Click any figure to enlarge with its caption.
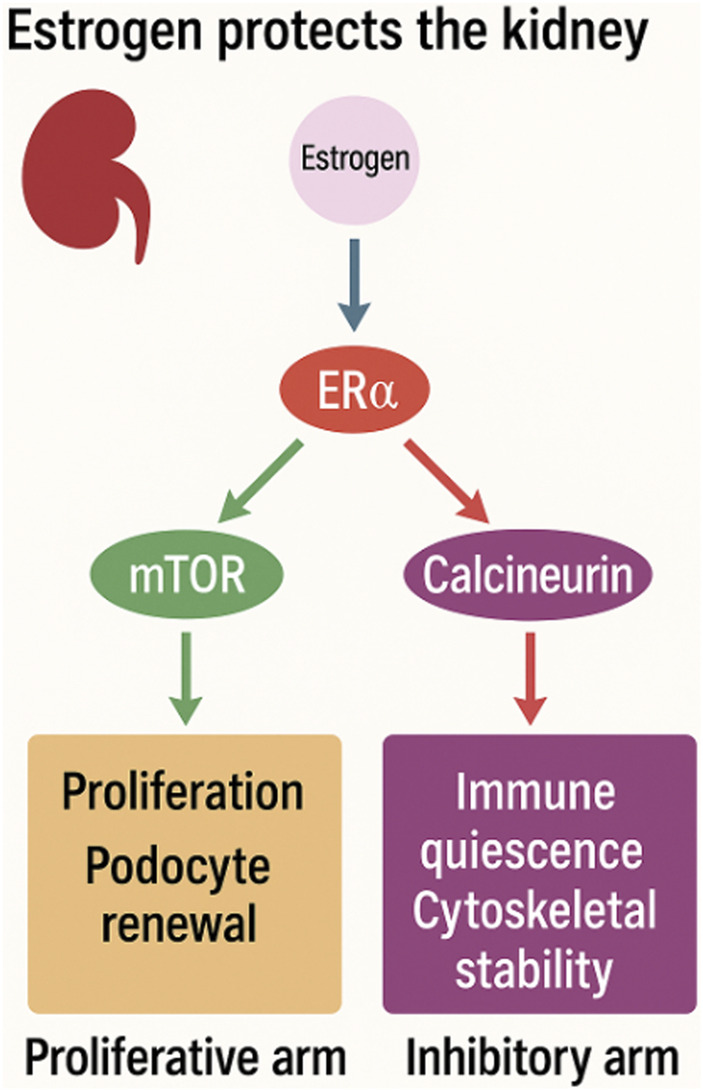 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPregnancy and Medication Impact · Renal Transplantation Outcomes and Treatments · Reproductive System and Pregnancy
Dear Editors,
Sex-based differences in chronic kidney disease (CKD) progression are well recognized: women generally experience slower renal function decline and greater resistance to podocyte injury than men. Paradoxically, this biological advantage largely disappears after kidney transplantation, where graft outcomes become broadly comparable between sexes [1]. The mechanisms underlying this loss of sexual dimorphism remain poorly understood.
Recent mechanistic studies on estrogen-regulated renal progenitors offer a unifying explanation [2]. Estrogen exerts renal protection through two complementary molecular axes. First, estrogen activates the ERα–PI3K/AKT–mTOR pathway, promoting renal progenitor proliferation and podocyte renewal, counterbalancing podocyte loss and preserving glomerular integrity. Elegant lineage-tracing and functional studies demonstrate that estrogen-dependent progenitor activation contributes directly to female renal resilience and adaptive capacity [3–6]. Second, estrogen physiologically suppresses calcineurin–NFAT signaling, limiting pro-inflammatory transcription, cytoskeletal destabilization, and maladaptive hypertrophy in podocytes [7, 8]. Together, these pathways establish a coordinated balance between regeneration and immune restraint, forming the biological basis of female renal advantage (Figure 1).
Testosterone, by contrast, drives these same pathways toward maladaptive outcomes. It stimulates mTORC1/S6K1 activity, but rather than sustaining progenitor renewal, the result is glomerular hypertrophy and fibrotic signaling. Simultaneously, testosterone enhances calcineurin/NFAT activation, amplifying pro-inflammatory transcription and accelerating glomerulosclerosis [9, 10]. This dual effect helps explain the well-documented male disadvantage in CKD progression.
Kidney transplantation introduces a pharmacologic environment that inadvertently neutralizes both estrogen-mediated protective axes. Calcineurin inhibitors (CNIs), the backbone of transplant immunosuppression, uniformly suppress NFAT signaling. In men, this mimics estrogen’s inhibitory effect; in women, it represents a redundant blockade that abolishes a uniquely protective pathway. Simultaneously, mTOR inhibitors directly counteract estrogen-driven progenitor proliferation, eliminating the regenerative advantage observed in female kidneys. Thus, transplantation creates an artificial biological equivalence not by enhancing male resilience, but by pharmacologically suppressing female resilience.
This framework suggests that sexual dimorphism in transplant outcomes is not inherently absent but rather masked by immunosuppressive strategies that converge on hormone-sensitive pathways. Importantly, registry studies increasingly suggest sex-specific differences in transplant benefit and long-term outcomes, supporting the biological plausibility of this interaction.
We propose that future transplant studies should systematically stratify outcomes by sex, hormonal status, and immunosuppressive regimen. Tailoring mTOR inhibition or adjusting its timing may preserve regenerative capacity in women without compromising graft protection. By recognizing that women may lose their intrinsic regenerative advantage under current regimens, the field can move toward truly individualized and sex-specific immunosuppression strategies that protect graft survival without disrupting inherent biological strengths.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Geroldinger A Strohmaier S Kammer M Schilhart-Wallisch C Heinze G Oberbauer R Sex Differences in the Survival Benefit of Kidney Transplantation: A Retrospective Cohort Study Using Target Trial Emulation. Nephrol Dial Transplant (2024) 39(1):36–44. 10.1093/ndt/gfad 137 37403325 PMC 10730810 · doi ↗ · pubmed ↗
- 2Conte C Angelotti ML Mazzinghi B Melica ME Antonelli G Carangelo G Estrogen-Regulated Renal Progenitors Determine Pregnancy Adaptation and Preeclampsia. Science (2025) 389(6764):1016–23. 10.1126/science.adp 4629 40906846 · doi ↗ · pubmed ↗
- 3Ma HY Chen S Du Y . Estrogen and Estrogen Receptors in Kidney Diseases. Ren Fail (2021) 43(1):619–42. 10.1080/0886022 X.2021.1901739 33784950 PMC 8018493 · doi ↗ · pubmed ↗
- 4Puelles VG van der Wolde JW Wanner N Scheppach MW Cullen-Mc Ewen LA Bork T m TOR-mediated Podocyte Hypertrophy Regulates Glomerular Integrity in Mice and Humans. JCI Insight (2019) 4(18):e 99271. 10.1172/jci.insight.99271 31534053 PMC 6795295 · doi ↗ · pubmed ↗
- 5Gui Y Dai C . Mtor Signaling in Kidney Diseases. Kidney 360 (2020) 1(11):1319–27. 10.34067/KID.0003782020 35372878 PMC 8815517 · doi ↗ · pubmed ↗
- 6Huber TB Walz G Kuehn EW . Mtor and Rapamycin in the Kidney: Signaling and Therapeutic Implications Beyond Immunosuppression. Kidney Int (2011) 79(5):502–11. 10.1038/ki.2010.457 21085109 · doi ↗ · pubmed ↗
- 7Wang Y Jarad G Tripathi P Pan M Cunningham J Martin DR Activation of NFAT Signaling in Podocytes Causes Glomerulosclerosis. J Am Soc Nephrol (2010) 21(10):1657–66. 10.1681/ASN.2009121253 20651158 PMC 3013542 · doi ↗ · pubmed ↗
- 8Shen X Jiang H Ying M Xie Z Li X Wang H Calcineurin Inhibitors Cyclosporin A and Tacrolimus Protect Against Podocyte Injury Induced by Puromycin Aminonucleoside in Rodent Models. Sci Rep (2016) 6:32087. 10.1038/srep 32087 27580845 PMC 5007516 · doi ↗ · pubmed ↗