Kidney care at NICU discharge and follow-up recommendations for preterm infants<34 weeks
Cara L. Slagle, Jennifer L. Chmielewski, Jennifer A. Rumpel, Keia R. Sanderson, Meredith P. Schuh, Michelle C. Starr, Jeffrey L. Segar, Namasivayam Ambalavanan, David Askenazi, David Selewski, Jennifer R. Charlton, Matthew W. Harer

TL;DR
This paper outlines kidney health recommendations for preterm infants to reduce long-term risks like chronic kidney disease and hypertension.
Contribution
The paper introduces consensus-based guidelines for kidney evaluations and follow-up care for preterm infants born before 34 weeks.
Findings
A kidney evaluation before NICU discharge and at two years of age is recommended for preterm infants.
Comprehensive kidney assessments are advised for infants at highest risk, such as those born before 28 weeks.
Parental education at multiple timepoints is emphasized to support early detection and management of kidney issues.
Abstract
Preterm birth increases the risk of chronic kidney disease (CKD) and hypertension later in life. To address these risks, the National Institutes of Health sponsored the Neonatal Kidney Health Consensus Workshop in February 2024, where a multidisciplinary group of experts reviewed current evidence, identified knowledge gaps, and developed consensus-based recommendations for kidney health follow-up in infants born <34 weeks. Key recommendations include a kidney evaluation before NICU discharge and at two years of age, with comprehensive kidney assessment for those at highest risk (birth <28 weeks, with acute kidney injury, intrauterine growth restriction, or small for gestational age). Cohesive, evidence-based parental education at multiple timepoints was emphasized to support early CKD detection and long-term management. This consensus provides a framework to optimize follow up and…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
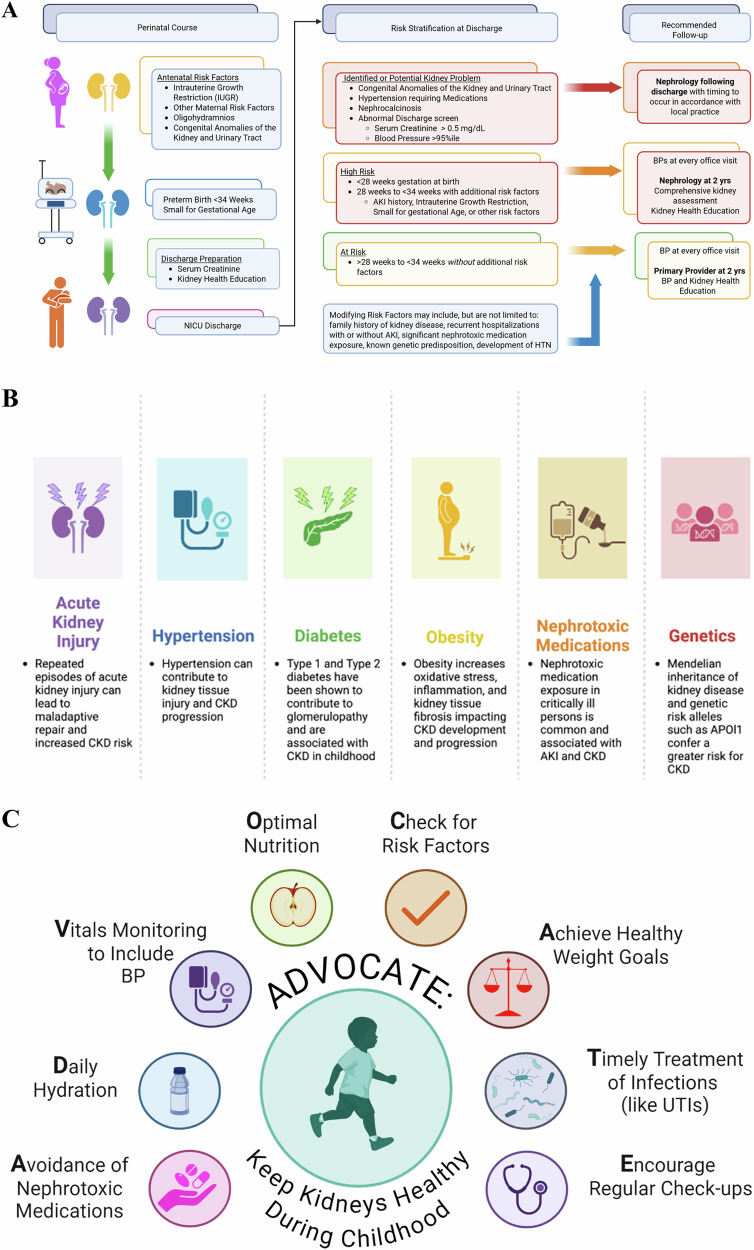 Figure 1
Figure 1- —https://doi.org/10.13039/100000062U.S. Department of Health & Human Services | NIH | National Institute of Diabetes and Digestive and Kidney Diseases (National Institute of Diabetes & Digestive & Kidn
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsBirth, Development, and Health · Chronic Kidney Disease and Diabetes · Acute Kidney Injury Research
Introduction
Although survival of preterm infants has dramatically improved, these children remain vulnerable to long-term complications [1–3], and kidney outcomes are now increasingly recognized as a critical concern [4–9]. As CKD is often silent, identification may be delayed until disease is advanced [10, 11]. While there are no comprehensive guidelines to evaluate for CKD and hypertension following a history of preterm birth, the American Academy of Pediatrics (AAP) recommended blood pressure (BP) monitoring for a variety of higher risk neonatal populations [12]. Additionally, Kidney Diseases Improving Global Outcomes (KDIGO) recognized preterm birth as a CKD risk factor [13]. Despite these recommendations, guidelines for the long-term monitoring of kidney disease in preterm neonates are lacking [10, 11, 14].
The first Neonatal Kidney Health Consensus workshop was convened in Indianapolis, Indiana, on February 27-28, 2024, to begin to address these pressing issues [15]. The preterm workgroup sought to address three questions on preterm birth and kidney health:
(1) What is the effect of preterm birth on kidney health over the life course?
(2) What is the effect of AKI in preterm infants on kidney health over the life course?
(3) What is the effect of other modifying factors in preterm infants on kidney health over the life course?
This manuscript details the work performed and conclusions drawn by the workgroup.
Methods
The preterm work group, one of three workgroups of the NIH-supported “Consensus Workshop to Address Kidney Health in NICU Graduates” was composed of a diverse group of experts in neonatology and nephrology from the United States [15]. Using current literature supplemented by expert opinion, this workgroup sought to (1) develop recommendations for preterm kidney health follow-up, (2) define gaps in knowledge, and (3) establish research priorities.
Pre-workshop activities included a comprehensive literature search performed with Covidence software (Supplement 1). Articles were screened for inclusion and full review (JRC and MWH). Each reviewer documented strength of evidence and key points from the assigned study.
The preterm workgroup used a modified Delphi method to review findings, develop recommendations, and identify research gaps and priorities [16, 17]. During the workshop, recommendations were presented to all in attendance, which included critical care, neonatology, cardiology, and nephrology specialists in addition to a primary care provider, an expert in equity and care delivery and a family representative [15]. Feedback was incorporated into final revisions before a formalized vote with 2/3 support required for adoption. SQUIRE guidelines were used to identify key elements for inclusion in the manuscript, though the project itself was not conducted as a formal quality improvement initiative [18].
Results
Why should preterm neonates have kidney health monitoring?
The impact of perinatal factors and preterm birth on kidney health over the life course has become increasingly clear [17]. Studies consistently indicate that preterm birth is a risk factor for the future development of CKD and hypertension (HTN) [5–7, 19–21]. Preterm infants experience disrupted nephrogenesis which typically does not conclude until 34–36 weeks GA [22, 23]. Following delivery, preterm infants are exposed to extrauterine environmental stressors, including high or low levels of oxygen, hypotension, inadequate nutrition, and nephrotoxic medications, that may further disrupt postnatal nephron formation [24–30].
Emerging preclinical studies provide mechanistic insights into the development and progression of CKD [31, 32]. Maternal co-morbidities such as gestational diabetes and hypertensive disorders, along with nutritional deficiencies during gestation, including low levels of vitamin A, protein, iron, zinc, and sodium, have been shown to have an effect on nephrogenesis and reduce nephron numbers in offspring [33]. Studies in preterm baboons raised in conditions resembling NICUs confirm disruptions in nephrogenesis [31, 32]. The long-term consequences of preterm birth on kidney health have been explored in other animal models, such as in rats and mice, in which nephrogenesis normally occurs postnatally. Single-nephron hyperfiltration increases GFR in context of nephron loss. This contributes to further nephron loss and subsequent CKD and HTN [4, 7].
Who should have kidney health monitoring after NICU discharge?
We define infants at-risk of CKD if they were <34 weeks GA. We defined infants at high-risk of CKD if they were <28 weeks GA, birthweight <1500 g, or were at-risk and had an additional risk factor (Table 1: Recommendations, Fig. 1A).Fig. 1. Consensus recommendations, risk modifiers, and education.A Consensus recommendations and Risk Stratification for outpatient kidney health follow-up for infants at risk of kidney disease during childhood. B Risk Modifiers for Kidney Disease Progression during childhood and adulthood. C Education related to Keeping Kidneys Healthy During Childhood.Table 1. Consensus recommendations for outpatient kidney health follow-up for preterm infants.Preterm infants (<34 week) recommendationsLevel of EvidenceOverall Recommendations**1Preterm infants (born <34 weeks’ gestation) should have a kidney health evaluation prior to NICU discharge that includes a properly obtained blood pressure (BP), and serum creatinine measurement, with parent(s)/guardian(s) provided kidney health education and resources. Infants identified with evidence of kidney disease at discharge (one or more of the following: serum creatinine >0.5 mg/dL, BP >95th percentile for age, hypertension treated with medications, nephrocalcinosis, or CAKUT), should receive follow-up with pediatric nephrology according to local guidance.32High-risk preterm infants ( < 28 weeks’ gestation, birthweight <1500 grams, or history of AKI or dialysis) should have a comprehensive kidney health assessment (BP, serum creatinine & Cystatin C, urine protein and/or urine microalbumin to urine creatinine ratio) in conjunction with standard care at two years of age, or sooner if there are significant exposures or events that modulate risk33At-risk preterm infants (28 to <34 weeks’ gestation) should have BP measurement and kidney health education at two years of age in conjunction with standard care. Providers should consider comprehensive kidney health assessment if there are significant exposures or events that modulate risk, including history of AKI and/or perinatal growth restriction3Who should have kidney health monitoring?Extremely Preterm Neonates (<28 wks)We recommend that in addition to kidney health education and BP assessment at every healthcare encounter, infants born < 28 weeks GA have a two-year (either chronologic or corrected age) comprehensive kidney health assessment (BP, serum creatinine & Cystatin C, urine protein and/or urine microalbumin to urine creatinine ratio). Assessment may occur sooner if additional CKD risk factors or significant exposures modulating CKD risk are present3Preterm Neonates 28 to < *34 wksWe recommend infants born 28–34 weeks GA have kidney health education and a BP assessment at two years of age in line with current AAP guidelines5Modifying Risk Factors:AKIWe recommend that AKI is defined using modified neonatal KDIGO criteria, with attention paid to accurate diagnosis, documentation, and communication at the time of discharge* [25, 65, 66]. Further, we note that preterm infants (28–34 weeks’ gestation) with AKI are at high risk for CKD and recommend that they should undergo comprehensive kidney health assessment at two years of age (serum creatinine, urine protein) in addition to BP assessment and kidney education.3*IUGR/SGAWe recommend that preterm infants (28–34 weeks’ gestation) born* < 1500 g (<10th percentile for weight at 33 weeks’ GA and <3rd percentile at 34 weeks’ GA) are at high risk for CKD and should undergo comprehensive kidney health assessment (BP, serum creatinine & Cystatin C, urine protein and/or urine microalbumin to urine creatinine ratio) at two years of age in addition to BP assessment and kidney education3Other**We acknowledge that family history, rehospitalization, and other risk factors should be taken into consideration when determining risk assessment for follow-up of preterm infants4What tests are indicated?****SerumWe recommend that serum cystatin C and serum creatinine should be obtained at two years of age for those < 28 weeks GA or in those 29 to < 34 weeks GA with modifying risk factors or concerns. Serum cystatin C and serum creatinine may be obtained at a two-year visit by the general provider optionally irrespective of risk factors.3Urine**We recommend that those at high-risk (preterm infants < 28 weeks GA or those born 28 to < 34 weeks GA but with ≥ 1 modifying risk factor) have urine albumin to creatinine ratios at a two-year follow-up visit. For infants 28 weeks GA to < 34 weeks GA with no risk factors, urine protein/urine creatinine ratios and/or urine microalbumin/urine creatinine ratios may be obtained at the discretion of the primary provider.5Imaging**We suggest that those at the highest risk (preterm infants < 28 weeks GA or those born 28 to < 34 weeks GA but with ≥ 1 modifying risk factor) may benefit from kidney ultrasound at a two year assessment at the discretion of the ordering nephrologist.5When should they be followed?****DischargeWe recommend all infants < 34 weeks have an accurate BP obtained, serum creatinine level checked, and parent(s)/guardian(s) provided with kidney health education.3Kidney Health Assessment at Two Years**We recommend all infants < 34 weeks have follow-up at two years of age, have an accurate BP obtained, serum creatinine level assessed, and parents provided with kidney health education3How should it be performed?****Kidney Health Education and ResourcesWe recommend that provider education should focus on additional risk factors for CKD beyond preterm birth, strategies to optimize kidney health at NICU discharge and throughout childhood, and monitoring strategies, with an emphasis on the importance of kidney-focused follow-up5Comprehensive Kidney AssessmentBP assessmentSerum Creatinine and Cystatin C for eGFR calculationUrine protein and/or albumin to urine creatinine ratio + /- Kidney UltrasoundSee above testingAKI, acute kidney injury, BP, blood pressure; CAKUT, congenital anomaly of kidney or urinary tract; CKD, chronic kidney disease, eGFR, estimated glomerular filtration rate, GA, gestational age, HTN, hypertension, IUGR, intrauterine growth restriction, NICU, neonatal intensive care unit, SGA, small for gestational age.
At- risk: preterm neonates 28 to < 34 weeks GA
The risk of CKD in preterm infants born 28–34 weeks GA should not be minimized. A Swedish registry found that children born at 28–33 weeks GA had a sixfold increased CKD risk by 0-9 years, with an adjusted hazard ratio of 5.96 (95% CI 4.07–8.73 p < 0.001) compared to term counterparts [6]. Similarly, a Norwegian cohort showed that preterm birth ( < 37 weeks GA) was associated with a 48% increase in the odds of stage 3–5 CKD (OR [95% CI]; 1.48 [1.33–1.66]) by a mean age of 26 years [34]. A recent meta-analysis indicated that individuals aged 6–41 years old who were born preterm had lower eGFR, higher BP, higher urine albumin/urine creatinine ratios, and smaller kidneys [21]. HTN is also a concern, with 13% of infants born <34 weeks GA having elevated systolic blood pressure ( > 90th percentile) at 3-year follow-up and additional studies demonstrating higher BP in later childhood and adulthood after preterm birth [35–37].We recommend infants born 28–34 weeks GA have kidney health education (see section: What and how should it be performed?) and a BP assessment at every medical encounter in line with current AAP guidelines (Level of Evidence 5).
Modifying risk factors: AKI
Acute kidney injury occurs in up to 30% of hospitalized neonates and is independently associated with increased length of hospital stay and mortality [38, 39]. The risk of AKI is inversely correlated with gestational age and birth weight in preterm neonates and is not well detected or documented [7, 40]. In pediatric and adult patients, AKI is an independent risk factor for subsequent CKD [41–45]. For neonates, the link between AKI and CKD remains less clear. A secondary analysis of the Preterm Epo Neuroprotection Trial (PENUT) found AKI Stage ≥2 was associated with an increased systolic BP at two years of age with an odds ratio of 1.24 (95% CI 1.04-1.48) [20]. In contrast, other investigators have found no association between neonatal AKI with kidney function later in childhood [46]. This lack of association between AKI and the development of HTN and/or CKD was also supported in a retrospective study examining 222 extremely low birth weight (ELBW, <1000 g) infants, 23 of whom had severe AKI [47].
Differences in outcomes, study design, heterogeneity of AKI causes, inconsistent documentation and study duration likely explains the inconsistent findings [40, 48–51]. Until these conflicting results are addressed in large prospective studies, we believe the health community should still consider CKD monitoring in children with a history of AKI in the NICU. We recommend that AKI is defined using modified neonatal KDIGO criteria, with attention paid to accurate diagnosis, documentation, and communication at the time of discharge [17, 50, 52]. Preterm infants (28–34 weeks GA) with AKI should undergo comprehensive kidney health assessment at two years of age in addition to BP assessment and kidney education (Level of Evidence 3).
Modifying risk factors: IUGR, SGA, and VLBW
Perinatal growth restriction, including intrauterine or fetal growth restriction (IUGR/FGR) and/or small for gestational age (SGA) ( < 10th percentile weight for gestational age), and very low birthweight (VLBW, <1500 g), are independent risk factors for developing CKD and HTN among infants born at 28–34 weeks GA [34, 36, 53, 54]. In a cohort of 446 VLBW infants followed to 3 years of age, a history of IUGR was associated with a significant reduction in kidney function [55]. The Norwegian Renal Registry described that preterm infants born with a combination of low birth weight ( < 2500 g) and SGA ( < 10th percentile) had an increased adjusted hazard ratio 2.96 (95% CI 1.84–4.76) for kidney failure by age 50 [34]. A separate study following preterm ( ≤ 32 weeks GA) VLBW infants until 10–13 years of age noted that 48% (30/62) had an SBP ≥90th percentile [36]. Additionally, in a cohort of Indian children born at <35 weeks’ gestation and evaluated at 12-18 months, for every one week increase in GA, eGFR increased by 5.48 mL/min/1.73m^2^ [53]. More notably, for every increase in birthweight Z-score by one, eGFR rose by 14.34 mL/min/1.73m^2^ (2.66–26.02) [53]. The direct relationship among GA, birth weight, and decreased eGFR is additionally supported in a Japanese cohort of infants born before 35 weeks GA, who were admitted to the NICU without a history of CAKUT, congenital heart disease, or AKI, and then followed up at 2 years of age [54]. We recommend that preterm infants (28–34 weeks GA) born < 1500 g (VLBW, and SGA at 33 weeks’ GA and <3rd percentile at 34 weeks GA) are at high risk for CKD and should undergo comprehensive kidney health assessment (BP assessment, serum creatinine and cystatin C for eGFR calculation, urine protein and/or albumin to urine creatinine ratio, ±kidney ultrasound) at two years of age in addition to kidney education (Level of Evidence 3).
Other modifying risk factors
Attention must be made to maternal history, particularly exposure preeclampsia and tobacco exposure, as these conditions have been associated with kidney disease in offspring [56, 57]. Growing literature supports the role of chronic lung disease (bronchopulmonary dysplasia) in the development of both short and long-term kidney dysfunction [58–61]. However, the relationship is highly confounded, and high-strength literature does not exist to inform recommendations [58]. Preterm infants may have additional risk factors following NICU discharge (Fig. 1B). Hospital readmission is common with nearly 50% of extremely preterm infants being hospitalized during the first two years of life [62–64]. Significant nephrotoxin medication exposures, new or recurrent incidences of AKI, or development of diabetes following NICU discharge can further elevate a child’s risk. In addition, family history and the emerging understanding of inheritable genetic traits are important risk factors in the progression to CKD [65]. Family history, rehospitalization, and other risk factors should be considered when determining an individual’s risk for kidney disease and need for follow-up (Level of Evidence 4).
Extremely preterm neonates (<28 weeks)
Infants born at earliest gestational ages at the highest risk for CKD [6]. In a Swedish birth registry, the adjusted hazard ratio (HR) for CKD by adulthood in infants born <28 weeks GA was 3.01 (95% CI 1.67–5.45) or an adjusted incidence rate of 13.45 per 100,000 person-years [6]. Other studies have shown that clinical features of CKD were detectable in extremely preterm infants ( < 28 weeks) at two years of age [20, 66]. We recommend that infants born < 28 weeks GA have a two-year (either chronologic or corrected age) comprehensive kidney health assessment. Assessment may occur sooner if additional CKD risk factors are present. (Level of Evidence 3).
When and where should they be followed?
Discharge
Screening at hospital discharge is an opportunity to identify those with CKD prior to discharge. Although supporting data is limited, several publications demonstrate that elevated SCr or BP can be detected at discharge [67–69]. Blood pressure should be measured in neonates per unit protocol and compared to published normative values based on post-menstrual age [70]. Preterm infants <34 weeks GA with a SCr>0.5 mg/dl or a BP>95th percentile at rest, nephrocalcinosis, or CAKUT at the time of discharge warrant pediatric nephrology follow-up. A SCr cut off of 0.5 mg/dL was based on consensus and data from Bateman et al. showing that for neonates born 25-27 weeks’ GA, the 95^th^ percentile cut-off for SCr at 60 days of age is 0.51 mg/dL [71]. We recommend all infants < 34 weeks GA have an accurate BP obtained, serum creatinine level assessed, and caregivers provided with kidney health education before NICU discharge (Level of Evidence 3).
Kidney health monitoring between discharge and two years
In newborns and infants, renal blood flow is physiologically low, gradually normalizing to adult levels by two years of age, when GFR stabilizes [72]. Therefore the best evidence for follow-up to determine subsequent CKD risk is at two years of age. Providing kidney health education at annual primary care visits, along with routine blood pressure screening may ensure follow-up and potentially modify future risk factors such as nephrotoxic medication exposure and aligns with the AAP recommendations related to BP screening [12, 73]. We also recognize that assessment by a pediatric nephrologist may be warranted if additional CKD risk factors or other significant exposures that increase this risk of CKD occur before this visit.
We additionally recognize that a pediatrician or family practice physician may not be every infant’s medical home. In a study published in 2014, two-fifths of complex medical patients did not visit their primary care physician in the previous year [74]. Thus, it is important for all care providers to ensure BPs are obtained and kidney health education is performed at follow-up visits. We recommend that infants < 34 weeks GA have kidney health education and BP assessment at every healthcare encounter following discharge** (Level of Evidence 4)**. We recommend at-risk infants < 34 weeks GA have blood pressures checked at every medical encounter per the AAP recommendations and a follow-up at two years of age with kidney health education and optional kidney health assessment (Level of Evidence 3). We recommend for high-risk infants (<28 weeks or 28 to < 34 weeks with at least one risk factor) they have education provided, an accurate BP obtained and a kidney health assessment. (Level of Evidence 3).
Kidney health monitoring after two years
Our recommendations are focused on early childhood based on the current evidence. However, this cohort of patients should be followed throughout childhood as their risk of CKD is likely to increase with age and potential additive risk factors such as obesity, diabetes, chronic illnesses, and nephrotoxic medication exposure. Interestingly, preterm neonates have a greater risk of developing both type 1 and 2 diabetes at a population level and in smaller studies, children born preterm have been found to have insulin insensitivity [75–78]. Diabetes is the leading cause of end-stage kidney disease in the adult population; therefore, those born preterm with an increased risk for diabetes should be monitored closely. It is important to consider kidney monitoring during periods of rapid growth, such as puberty, as kidney function in patients with CKD can deteriorate during this time of accelerated growth and hormonal exposure [79]. Persistent abnormalities in the kidney health assessment should be monitored in accordance with standard monitoring practices established by pediatric nephrologists for albuminuria, elevated blood pressure, hypertension, reduced GFR, or renal hypoplasia.
What and how should it be performed?
Kidney health education and resources
An emphasis on kidney health at NICU discharge and subsequent follow-up with providers is critical–both for families and providers. In a single center study, 75% of caregivers were unaware their infant had AKI and 94% were unaware of any problem with their kidneys [80]. Family education should include education on nephrotoxic medications (including medications like ibuprofen which are over-the-counter) and a discussion of the importance of kidney health awareness (Fig. 1C). As resources vary by institution, this education may be provided by the discharging provider or a subspecialist. Parents identified the transition from the NICU to home as an opportunity to learn to prepare for the unexpected and identified a need for reliable sources of information [81, 82]. Thus, identification of any potential barriers and discussion, preparation, and solutions to overcome them may increase adherence rate for future kidney follow-up [82]. We recognize challenges in providing kidney health education both at discharge and in the outpatient settings due to a variety of constraints. Reliable and easily accessible resources should be provided to families as reference at times when they can accept and retain information. We recommend that education focus on avoiding additional risk factors for CKD beyond preterm birth with an emphasis on the importance of kidney-focused follow-up at 2 years of age (Level of Evidence 5).
Comprehensive kidney assessment
For all preterm neonates <34 weeks GA, BP assessment should be performed by the primary care provider as recommended by the AAP with expansion to all patient interactions [73]. To determine if a blood pressure is elevated, for neonates we recommend using the published reference data and for children over the age of 1 year, we recommend the 2017 guidelines published in Pediatrics which also includes details on standardized techniques [12, 83]. High-risk neonates ( < 28 weeks GA or those <34 weeks GA with additional risk factors) should undergo a comprehensive kidney evaluation including BP assessment, serum and urine studies as described below. Kidney imaging, such as ultrasound, may help guide kidney assessment, but little evidence exists to support its use. If additional risk factors are present or there are clinical concerns like hypertension or failure to thrive, a comprehensive kidney evaluation can be performed earlier than two years. Kidney health education should accompany all laboratory testing as the risk of progression to CKD in preterm infants extends past two years of age [6].
Laboratory studies
Laboratory studies include both blood testing and urine testing. We recommend the measurement of serum creatinine (SCr) and cystatin C to estimate GFR using the U25 formula [12, 73, 84, 85]. The training set for U25 formula included 25 individuals born preterm which was 4% of the total population. Although gold standard, estimated GFR using SCr and cystatin C were not designed for those <1 year of age and should be interpreted with caution for multiple reasons in these populations depending on the time point assessed [66, 86, 87]. An eGFR<90 ml/min/1.73m^2^ would be considered abnormal, CKD stage 2. We recommend that serum cystatin C and serum creatinine should be obtained at two years of age for those < 28 weeks’ GA or in those 29 to < 34 weeks’ GA with modifying risk factors or concerns (Level of Evidence 3).
Proteinuria and albuminuria can be early signs of kidney damage and may be a harbinger for the development of CKD [88–92]. Quantitation of urine protein detects all proteins in the urine, while urine albumin is more specific for glomerular injury, and the addition of a urine creatinine allows assessment of the concentration of the sample. Accepted cutoffs for normal urine protein to urine creatinine (UPC) in infants are higher (0.81 mg of protein per mg of creatinine) until 6 months, 0.5 mg/mg from 6-24 months and <0.2 mg/mg after 24 months. Normal urine albumin to urine creatinine ratios (UAC) is <30 mg albumin per gram of creatinine. Microalbuminuria, referring to smaller amounts of albuminuria (30–300 mg of albumin to g of creatinine) has been linked to kidney disease progression and thus was included in the cutoffs above [93, 94]. These ratios can be challenging and inaccurate in the setting of low urine creatinine, falsely increasing a UPC value. Given the increased risk of kidney disease of this population, we suggest that proteinuria and/or albuminuria at two years of age is an opportunity for screening and/or early detection of CKD. We recommend that those at high-risk (preterm infants < 28 weeks GA or those born 28 to < 34 weeks GA but with ≥ 1 modifying risk factor) have urine albumin to creatinine ratios at a two-year follow-up visit. For infants 28 weeks GA to < 34 weeks GA with no risk factors, urine protein/creatinine and/or urine albumin/creatinine ratio may be obtained at the discretion of the primary provider. (Level of Evidence 5).
Imaging
The impact of kidney volume as a marker for the risk of subsequent chronic kidney disease in preterm neonates remains a hot topic of research. Studies evaluating the association of kidney size with progression to CKD is limited primarily to children with anomalies of the kidney and urinary tract [95, 96]. In early adulthood (median age 23 years), those born <30 weeks GA had lower kidney volumes than matched controls born at term [97]. Smaller kidney volumes and lengths have also been observed in cohorts of adolescents born with IUGR and <30 weeks GA [98], and 12-18 month-old children, born preterm and SGA [53]. Normative values for kidney length and volume have been published to guide interpretation in infants and children, providing important context when assessing for abnormal growth [99, 100]. Thus, evaluation of kidney size over time may help predict CKD. Further research is greatly needed to better understand kidney volume as a risk factor for subsequent CKD [101, 102]. We suggest that those at the highest risk (preterm infants < 28 weeks GA or those born 28 to < 34 weeks GA but with ≥ 1 modifying risk factor) may benefit from kidney ultrasound at a two-year assessment at the discretion of the ordering nephrologist (Level of Evidence 5).
Gaps in knowledge
Despite the evidence above, many recommendations are limited given the significant gaps in the literature. Important gaps in knowledge remain and we recognize that the recommendations above serve only as a starting point. The landscape on which this framework was built is rapidly evolving as younger gestational-age infants survive into early adulthood. Advocating for the inclusion of both short and long-term kidney outcomes in all NICU research studies will help to start to fill this gap [103].
We note that it is essential to standardize outcome measures and gather meaningful data to related to screening, efficiency, and impact through multi-center longitudinal studies [103]. Furthermore, while AKI is well understood to be a risk factor for CKD, AKI encompasses a heterogeneous group of mechanisms and represents functional loss defined by imperfect biomarkers [17]. Thus, improvement in phenotyping of AKI is necessary to aid in risk stratification of progression to CKD for potential targeted prevention [17]. Risk stratification includes diagnostic tools and clinical data. Serum creatinine, cystatin C, and urine output are the most well-studied, but remain largely imperfect for both neonates and infants [48]. Urinary biomarkers, such as urine neutrophil gelatinase-associated lipocalin is gaining traction and implementation, but has not yet been used for long-term risk stratification [104–106]. Further study is greatly needed utilizing current diagnostic tools, clinical data, and novel biomarkers to optimize risk stratification to guide future follow-up strategies.
Research priorities
Research needed includes mechanistic, clinical, and implementation studies to prioritize the outlined knowledge gaps. Statistical models and risk score calculators will be critical for rapid identification, streamlining referral and follow-up scheduling, and enhancing overall implementation and adherence to recommendations. Neonatal kidney health registries and long-term follow-up are urgently needed to understand both in-hospital risk factors, risk modifiers following discharge, and ultimate progression to CKD. Additionally, as kidney replacement devices for infants become more readily available and potentially more widely used, the role of dialysis on long-term kidney health will be critical to address.
Discussion (feasibility, implementation challenges, and potential benefits and harms)
These consensus recommendations provide cohesive best practices in a population at high risk for kidney disease based on current evidence and were developed in a consensus manner with multi-disciplinary experts in the field. These recommendations provide a framework to begin to study and optimize the follow-up of these high-risk neonates.
We recognize that our recommendations present implementation challenges. We estimated that ~20,000 preterm infants would be considered at high risk of future CKD [107]. While a two-year follow-up visit may be most beneficial with a pediatric nephrologist, current workforce issues and uneven distribution of pediatric nephrologists in the country may make this unfeasible [108]. With the expansion of physician extenders like nurse practitioners and physician assistants, and the establishment of specific neonatal AKI follow-up clinics, it may be possible for more children to see a Pediatric Nephrology team in future recommendations. Also, since our recommendations require knowing the potential risk factors that change follow-up timing and screening, it will be vitally important that risk factors like SGA and AKI are included in discharge summaries. Future work could be to find ways to add these risk factors to other enduring childhood health documentation like vaccination or growth records.
We note that the BP recommendations align with the AAP guidelines for screening after NICU discharge. We acknowledge that outpatient pediatricians may not have the necessary equipment for accurate assessment of infant BPs. However, advocacy is needed to ensure that appropriate blood pressure cuffs are available in all pediatric practices. Given the large number of infants who will require blood pressure monitoring including, but not limited to, NICU graduates, ensuring access to proper tools must be a priority.
The recommendations confer several benefits but also risks to consider. The main risk is an increase in anxiety for the parents of these already medically complex children. The potential benefits of these recommendations are significant. Early screening may detect signs of CKD months to years earlier than it would have been identified without screening. This early detection could result in earlier control of blood pressure, treatment of proteinuria, and could ultimately slow the progression of CKD. The educational component could result in parents feeling more empowered and informed and result in avoidance of nephrotoxic medications and maintenance of a healthy weight. From a neonatology standpoint, these recommendations could continue to inform the large work force of the importance of the kidney in NICU care and continue to raise awareness about the implications of preterm birth and AKI on long-term kidney health. Our group recognizes the potential harm that may result from these recommendations, including the potential for more blood draws, BP measurements, and follow up including an increased burden to an already stretched work force in pediatric nephrology [107].
Preterm infants, especially those born before 34 weeks GA, have an increased risk of CKD and HTN. As neonatal survival improves, the long-term adverse impact of preterm birth on kidney health may increase. Through the development these consensus recommendations for kidney health monitoring, we provide guidance on kidney health assessments at NICU discharge and at two years of age for at-risk infants. Comprehensive screening and kidney education for families are crucial to early detection and the management of kidney disease. More research is needed to fill the gaps in knowledge, modifiable risk factors, risk stratification and the interplay between kidney health and other organ systems. These recommendations represent an important step toward improving outcomes for this high-risk population.
Supplementary information
Supplemental Material 1
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Rumpel JA, Perazzo S, Bona J, South AM, Harer MW, Liu D, et al. ADVANCE: a biomedical informatics approach to investigate acute kidney injury in infants. Pediatr Res. 2025;97:608–13.10.1038/s 41390-024-03436-5PMC 1202451539122822 · doi ↗ · pubmed ↗
- 2Flynn JT, Kaelber DC, Baker-Smith CM, Blowey D, Carroll AE, Daniels SR, et al. Clinical practice guideline for screening and management of high blood pressure in children and adolescents. Pediatrics. 2018;142:e 20181739.10.1542/peds.2017-190428827377 · doi ↗ · pubmed ↗
- 3Heo JS, Lee JM. The long-term effect of preterm birth on renal function: a meta-analysis. Int J Environ Res Public Health. 2021;18:2951.10.3390/ijerph 18062951 PMC 800102733805740 · doi ↗ · pubmed ↗
- 4Meena J, Kumar J, Kocharlakota JP, Gupta H, Mittal P, Kumar A, et al. Acute kidney injury in neonates: a meta-analysis. Pediatrics. 2024;154:e 2023065182.10.1542/peds.2023-06518238872621 · doi ↗ · pubmed ↗
- 5Wallace SW, Geers ER, Niehaus JZ, Cristea AI, Starr MC. Kidney complications in children with bronchopulmonary dysplasia. Pediatr Res. 2025;97:2431–35.10.1038/s 41390-024-03638-x PMC 1246346239443697 · doi ↗ · pubmed ↗
- 6Stoops C, Gavigan H, Krallman K, Anderson N, Griffin R, Slagle C, et al. The utility of urinary NGAL as an alternative for serum creatinine to detect acute kidney injury in infants exposed to nephrotoxic medications in the neonatal intensive care unit. Neonatology. 2024;121:203–12.10.1159/000535322 PMC 1098726938151013 · doi ↗ · pubmed ↗
- 7Weidemann DK, Orr CJ, Norwood V, Brophy P, Leonard MB, Ashoor I. Child health needs and the pediatric nephrology subspecialty workforce: 2020–2040. Pediatrics. 2024;153:e 2023063678 P.10.1542/peds.2023-063678 P 38300004 · doi ↗ · pubmed ↗