Radiomics and artificial intelligence-based prediction of tumor response in digestive system neoplasm: a systematic review and meta-analysis
Songxia Yu, Meini Gong, Haowen Wang, Hanbo Liu, Min Deng

TL;DR
This paper reviews how radiomics and AI can predict tumor outcomes in digestive cancers, showing strong effectiveness across various diagnostic and prognostic applications.
Contribution
The study provides a systematic review and meta-analysis of AI and radiomics applications in digestive system tumors, highlighting their diagnostic and prognostic potential.
Findings
AI significantly improves detection in upper GI endoscopy, colonoscopy, and capsule endoscopy.
Radiomic models effectively predict tumor response and recurrence in colorectal and gastric cancers.
AI-based strategies accurately assess patient risk and predict molecular tumor types and survival.
Abstract
Radiomics and artificial intelligence (AI) are progressively gaining recognition for predicting tumor response, recurrence, and prognosis in gastrointestinal tumors. The current review singled out the diagnostic and prognostic potential of AI and radiomics in the whole GI tract. Out of 120 ongoing studies from the year 2016 to 2025, the following applications were covered: endoscopy, colonoscopy, capsule endoscopy, intraoperative guidance, CT/MRI radiomics, and molecular/histopathology AI models. The performance across studies was assessed by meta-analysis using random-effects modeling that incorporated inverse variance methods. Results from the analysis of heterogeneity (I2), publication bias (funnel plots, Egger's test), methodological quality (Radiomics Quality Score, RQS), and risk of bias (PROBAST) were reported. The use of AI in detection and diagnosis assisted with the…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
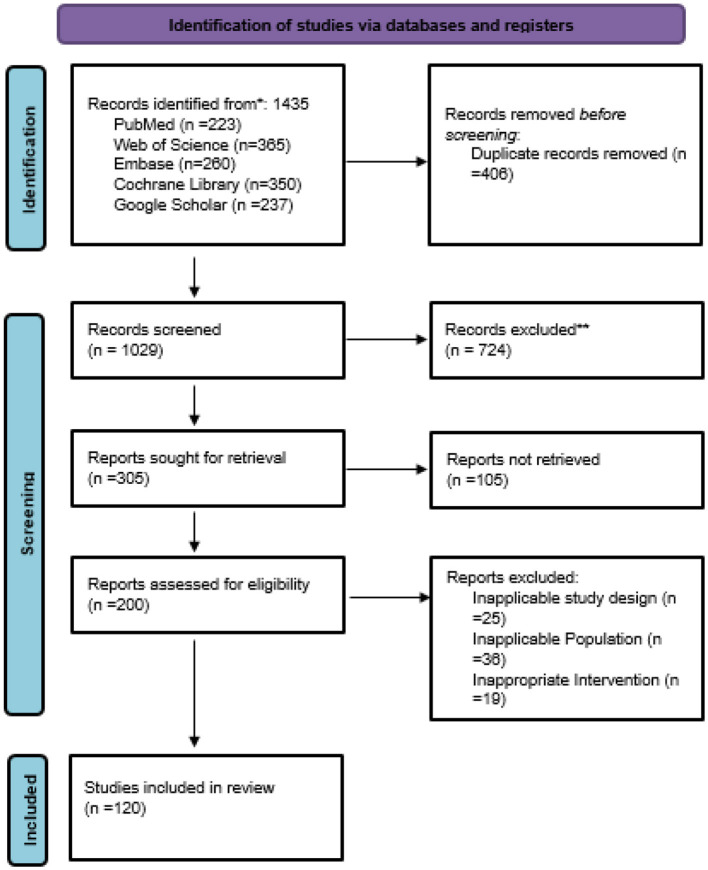 Figure 1
Figure 1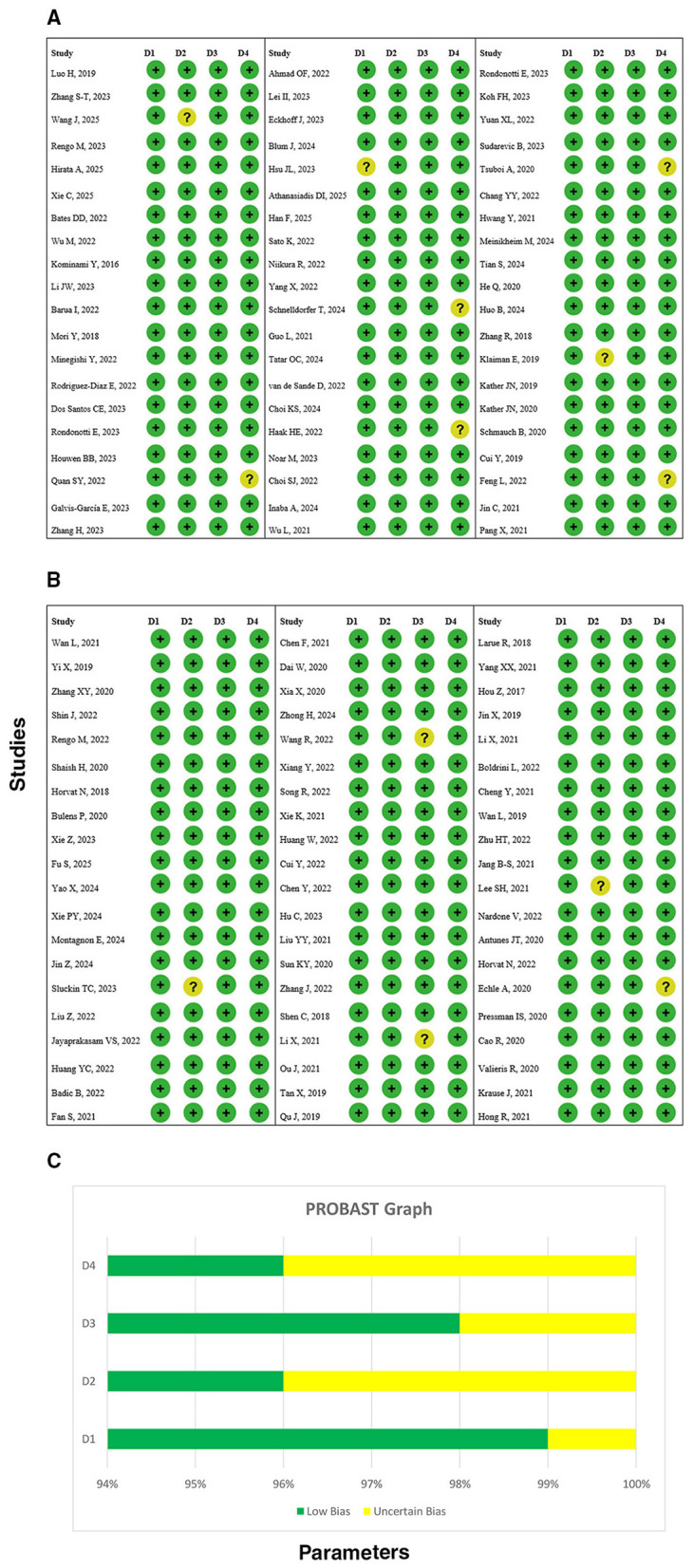 Figure 2
Figure 2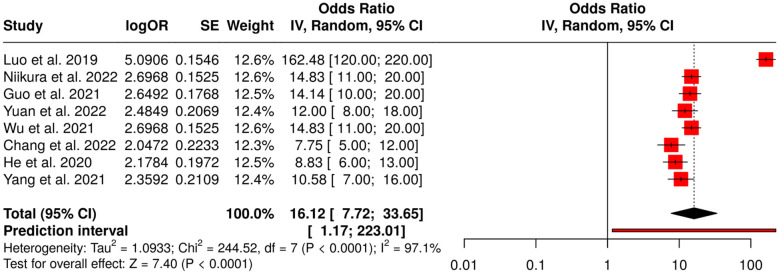 Figure 3
Figure 3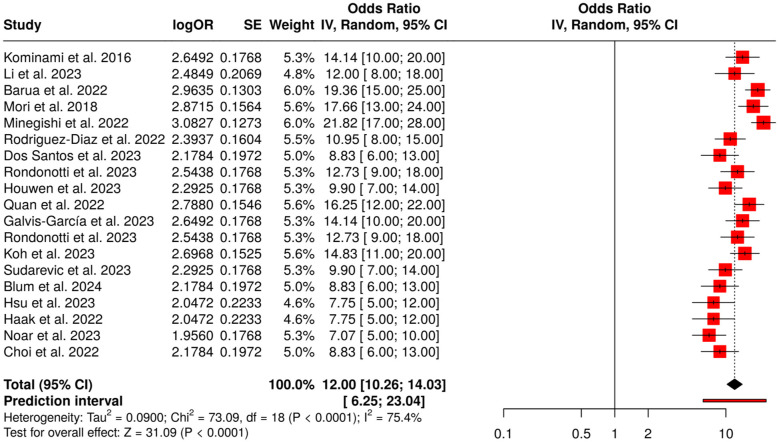 Figure 4
Figure 4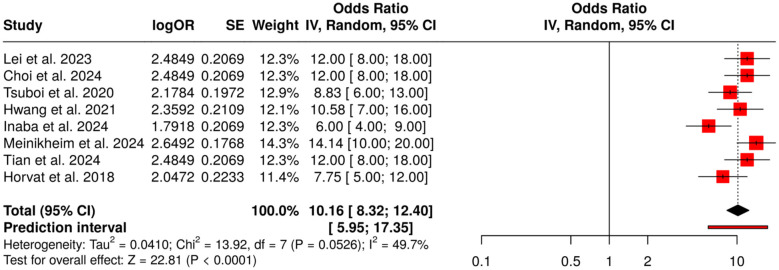 Figure 5
Figure 5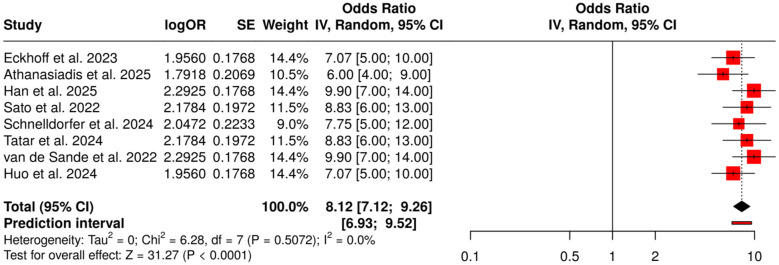 Figure 6
Figure 6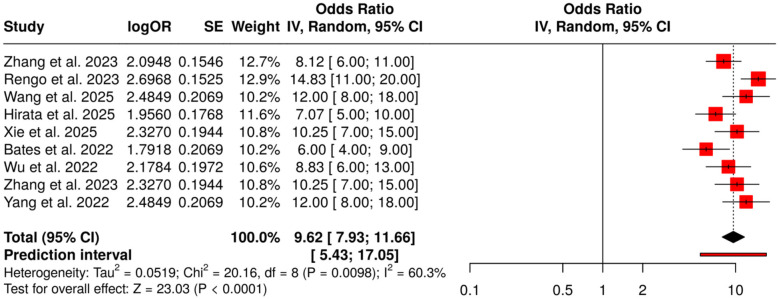 Figure 7
Figure 7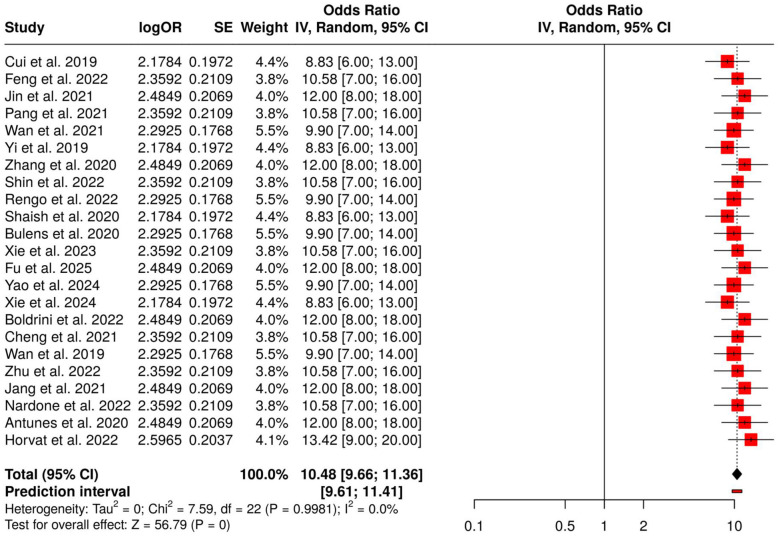 Figure 8
Figure 8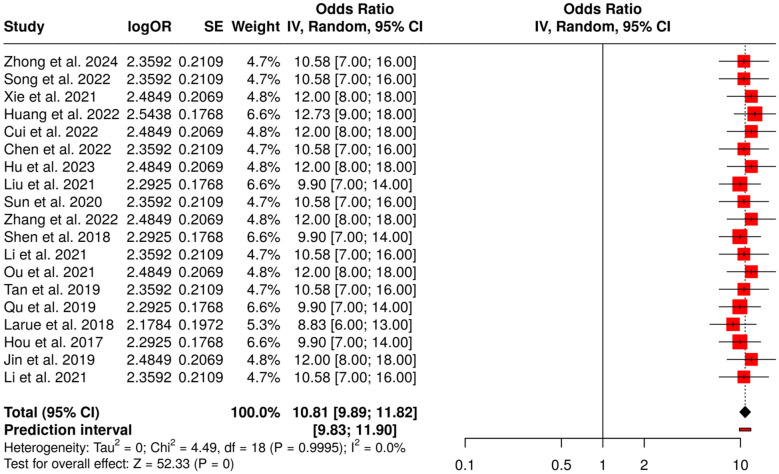 Figure 9
Figure 9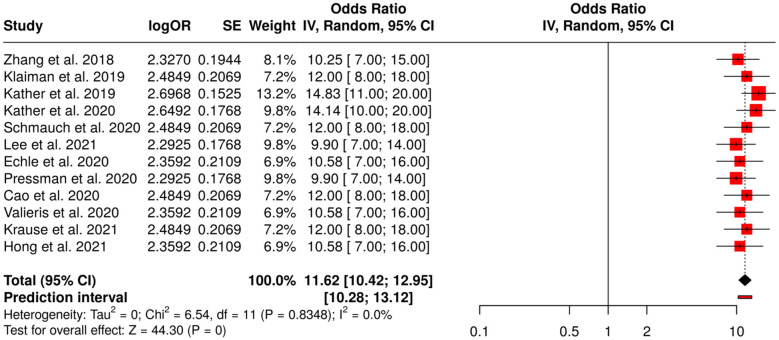 Figure 10
Figure 10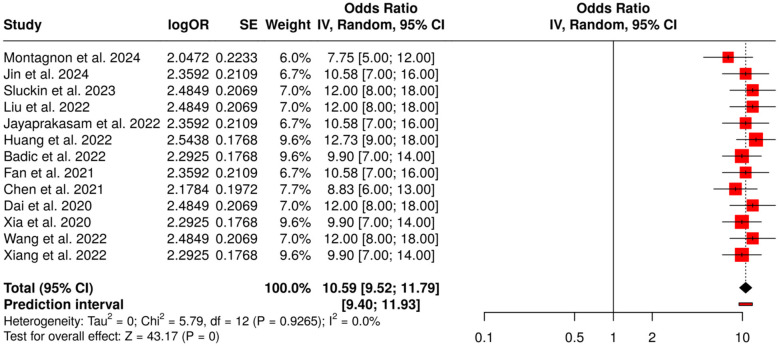 Figure 11
Figure 11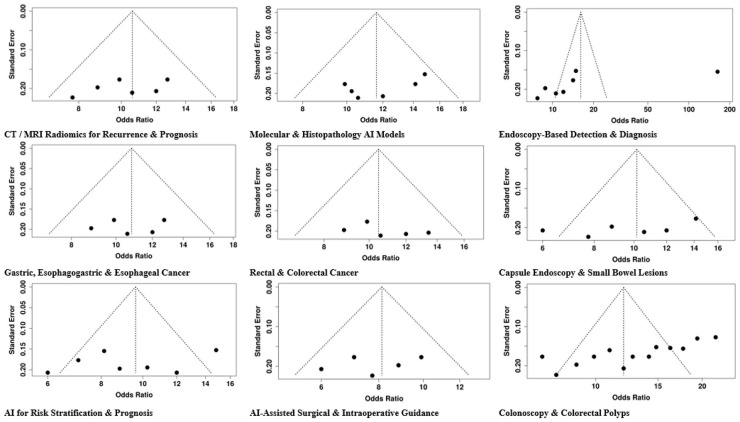 Figure 12
Figure 12|
|
|
|
|
|
|
|
|
|
|
|---|---|---|---|---|---|---|---|---|---|
| Luo et al. ( | 2019 | China | Upper GI | Endoscopic imaging | CNN real-time AI | Cancer detection | Multicentre diagnostic | External multicentre | Sensitivity, specificity, accuracy |
| Zhang et al. ( | 2023 | China | Esophageal SCC | CT imaging | Radiomics CAD | Lymph node metastasis | Multicentre diagnostic | External multicentre | AUC, sensitivity, specificity |
| Wang et al. ( | 2025 | China | GI cancers | Digital pathology (IHC) | CNN models | Tumor subtype and stage | Development and validation | External | AUC, accuracy |
| Rengo et al. ( | 2023 | Italy | GIST | CT radiomics | Radiomics AI model | Preoperative risk stratification | Retrospective radiomics | External | AUC, calibration |
| Hirata et al. ( | 2025 | Japan | Esophageal SCC | MRI radiomics | AI-based MRI radiomics | Pathological complete response to chemoradiotherapy | Retrospective study | External | AUC, sensitivity, specificity |
| Xie et al. ( | 2025 | China | Stage II colorectal cancer | Multimodal clinical/omics | Multimodal AI | Guide adjuvant chemotherapy | Retrospective/integrative | External/simulated | AUC, predictive accuracy |
| Bates and Pickhardt ( | 2022 | USA | Various oncologic | CT body composition | AI-based body composition | Prognostic assessment | Retrospective | External | HR, survival correlation |
| Wu et al. ( | 2022 | China | Epithelial ovarian cancer | Clinical/imaging | AI-based preoperative system | Diagnosis and prognosis | Multicenter study | External | AUC, accuracy |
| Kominami ( | 2016 | Japan | Colorectal polyps | Narrow-band imaging colonoscopy | CAD real-time image recognition | Polyp histology prediction | Prospective | Internal | Accuracy, sensitivity, specificity |
| Li et al. ( | 2023 | Taiwan | Colorectal polyps | Colonoscopy | CAD system | Polyp histology prediction | Prospective multicentre | External | Accuracy, AUC |
| Barua et al. ( | 2022 | Japan/Europe | Colorectal polyps | Colonoscopy | Real-time AI optical diagnosis | Neoplastic polyp detection | Prospective | External/multicentre | Sensitivity, specificity |
| Mori et al. ( | 2018 | Japan | Colorectal polyps | Colonoscopy | Real-time AI | Diminutive polyp detection | Prospective | External | Sensitivity, specificity |
| Minegishi et al. ( | 2022 | Japan | Colorectal | Colonoscopy | AI-assisted optical diagnosis | Real-time lesion characterization | Prospective | External | Accuracy, sensitivity |
| Rodriguez-Diaz et al. ( | 2022 | USA | Colorectal polyps | Elastic-scattering spectroscopy | AI assessment | Polyp histology prediction | Prospective | External | Accuracy, sensitivity |
| Dos Santos et al. ( | 2023 | Brazil | Colorectal lesions | Colonoscopy | AI characterization | Lesion characterization | Prospective | External | Accuracy, AUC |
| Rondonotti et al. ( | 2023 | Italy | Colorectal | BLI endoscopy | AI-assisted optical diagnosis | Resect-and-discard strategy | Prospective | External | Accuracy, sensitivity, specificity |
| Houwen et al. ( | 2023 | Netherlands | Colorectal | Colonoscopy | CAD real-time | Diminutive polyp and sessile serrated lesion assessment | Prospective | External | Accuracy, sensitivity |
| Quan et al. ( | 2022 | USA | Colorectal polyps | Colonoscopy | Real-time AI detection | Polyp detection | Multicenter pilot study | External | Sensitivity, specificity |
| Galvis-García et al. ( | 2023 | Mexico | Colorectal | Colonoscopy | AI-assisted screening | Reduction of miss rate | Prospective | External | Sensitivity, specificity |
| Zhang et al. ( | 2023 | China | Biliary/ choledocholithiasis | CT imaging | Computational AI prediction models | Risk assessment and diagnosis | Retrospective | External | Accuracy, sensitivity, specificity |
| Ahmad et al. ( | 2022 | UK | Colorectal | Colonoscopy | AI system | Detection of subtle and advanced neoplasia | Prospective | External | Sensitivity, specificity |
| Lei et al. ( | 2023 | UK | Small bowel | Capsule endoscopy | AI-enabled image analysis | Detection at scale | Prospective | External | Accuracy, sensitivity |
| Eckhoff et al. ( | 2023 | Germany | Upper GI/esophagectomy | Laparoscopic video | TEsoNet knowledge transfer | Surgical phase recognition | Retrospective | External | Accuracy |
| Blum et al. ( | 2024 | Australia | Biliary/ choledocholithiasis | CT/clinical | ML models | Predict choledocholithiasis | Retrospective | External | Accuracy, AUC |
| Hsu et al. ( | 2023 | USA | Bariatric surgery | Clinical/operative data | ML models | Postoperative GI bleed prediction | Retrospective | External | Accuracy, HR |
| Athanasiadis et al. ( | 2025 | UK | Laparoscopic cholecystectomy | Surgical video | Expert vs. AI evaluation | Critical view of safety | Prospective observational | External | Accuracy |
| Han et al. ( | 2025 | China | Rectal | Surgical video | AI recognition system | Pelvic nerve identification | Prospective/experimental | External | Accuracy |
| Sato et al. ( | 2022 | Japan | Thoracic esophagectomy | Surgical video | AI real-time detection | Recurrent laryngeal nerve | Prospective | External | Accuracy |
| Niikura et al. ( | 2022 | Japan | Gastric cancer | Endoscopy | AI vs. expert endoscopists | Diagnosis | Prospective | External | Sensitivity, specificity |
| Yang et al. ( | 2022 | China | GIST/leiomyoma | Endoscopic ultrasonography | AI system | Tumor differentiation | Retrospective | External | Accuracy, AUC |
| Schnelldorfer et al. ( | 2024 | USA | GI metastases | Intraoperative imaging | Deep learning system | Intraoperative metastases identification | Retrospective/ development | External | Accuracy, sensitivity |
| Guo et al. ( | 2021 | China | Multiple GI lesions | Endoscopy | AI model | Detection of multiple lesions | Pilot study | External | Sensitivity, specificity |
| Tatar et al. ( | 2024 | Turkey | Colorectal lesions | Colonoscopy | Surgical insight-guided deep learning | Lesion management | Prospective | External | Accuracy |
| van de Sande et al. ( | 2022 | Netherlands | Postoperative GI | Clinical/surgical data | AI decision support tool (DESIRE) | Optimize discharge | External validation study | External | Accuracy, predictive performance |
| Choi et al. ( | 2024 | Korea | Small-bowel | Capsule endoscopy | Deep learning | Lesion detection and diagnostic yield | Prospective | External | Sensitivity, accuracy |
| Haak et al. ( | 2022 | Netherlands | Rectal cancer | Endoscopic imaging | Deep learning | Tumor response post-chemoradiation | Prospective | External | AUC, accuracy |
| Noar et al. ( | 2023 | UK | Gastroparesis | Gastric myoelectrical data | AI threshold model | Predict resolution post-intervention | Prospective | External | Accuracy |
| Choi et al. ( | 2022 | Korea | Upper GI | EGD images | AI system | Photo documentation quality | Prospective | External | Accuracy |
| Inaba et al. ( | 2024 | Japan | Colonoscopy prep | Smartphone app | AI-based evaluation | Stool state assessment | Prospective | External | Accuracy |
| Wu et al. ( | 2021 | China | Gastric cancer | Endoscopy | AI system | Early cancer detection | Randomized controlled trial | External | Sensitivity, specificity |
| Rondonotti et al. ( | 2023 | Italy | Colorectal polyps | BLI endoscopy | AI-assisted optical diagnosis | Resect-and-discard strategy | Prospective | External | Accuracy, sensitivity |
| Koh et al. ( | 2023 | Singapore | Colorectal adenomas | Colonoscopy | Real-time AI-aided | Adenoma detection rate | Prospective cohort | External | ADR, accuracy |
| Yuan et al. ( | 2022 | China | Gastric lesions | White-light endoscopy | AI system | Lesion diagnosis | Prospective | External | Accuracy, sensitivity, specificity |
| Sudarevic et al. ( | 2023 | Germany | Colorectal polyps | Endoscopy | AI-based size measurement | Polyp size estimation | Prospective | External | Accuracy, precision |
| Tsuboi et al. ( | 2020 | Japan | Small-bowel angioectasia | Capsule endoscopy | CNN | Automatic lesion detection | Retrospective | External | Sensitivity, specificity |
| Chang et al. ( | 2022 | Taiwan | Upper GI | Endoscopy images | Deep learning | Photodocumentation quality evaluation | Prospective | External | Accuracy |
| Hwang et al. ( | 2021 | Korea | Small bowel | Capsule endoscopy | CNN | Classification and localization | Prospective/pilot | External | Accuracy, sensitivity |
| Meinikheim et al. ( | 2024 | Germany | Barrett's esophagus | Endoscopy | AI-assisted | Diagnostic performance of endoscopists | Randomized tandem and video trial | External | Accuracy, ADR |
| Tian et al. ( | 2024 | China | Biliopancreatic | Endoscopic ultrasonography | AI-based diagnosis | Standard EUS site recognition | Multicenter retrospective | External | Accuracy, AUC |
| He et al. ( | 2020 | China | Upper GI | Endoscopy | CNN | Anatomical site classification | Retrospective | External | Accuracy |
| Huo et al. ( | 2024 | USA | GERD surgery | Clinical and imaging | LLM-linked AI | Surgical decision-making | Prospective/clinical evaluation | External | Accuracy, agreement with guidelines |
| Zhang et al. ( | 2018 | Netherlands | GI cancers | Histopathology | Adversarial deep learning | Microsatellite instability prediction | Retrospective | External | AUC, accuracy |
| Klaiman et al. ( | 2019 | USA | GI cancers | Histopathology | Hypothesis-free DL | Biomarker status, diagnosis, outcome | Retrospective | External | Accuracy, AUC |
| Kather et al. ( | 2019 | Germany | GI cancers | Histology | DL | Predict MSI from histology | Retrospective | External | AUC, accuracy |
| Kather et al. ( | 2020 | Germany | Pan-cancer (GI included) | Histology | DL | Detect actionable genetic alterations | Retrospective | External | Accuracy, AUC |
| Schmauch et al. ( | 2020 | France | GI and other cancers | Whole slide images | DL | Predict RNA-Seq expression | Retrospective | External | R2, AUC |
| Cui et al. ( | 2019 | China | Rectal cancer | Multiparametric MRI | Radiomics | Pathologic complete response after nCRT | Retrospective | External | AUC, sensitivity, specificity |
| Feng et al. ( | 2022 | China | Rectal cancer | MRI/histology | Radiopathomics | Pathologic complete response (pCR) after nCRT | Multicentre observational | External | AUC, accuracy |
| Jin et al. ( | 2021 | China | Rectal cancer | Longitudinal MRI | Multi-task DL | Treatment response | Retrospective | External | AUC, accuracy |
| Pang et al. ( | 2021 | China | Rectal cancer | MRI (single modality) | Deep segmentation + Radiomics | pCR after nCRT | Retrospective | External | AUC, sensitivity, specificity |
| Wan et al. ( | 2021 | China | Rectal cancer | MRI | Delta-radiomics | pCR after nCRT | Retrospective | External | AUC |
| Yi et al. ( | 2019 | China | Rectal cancer | MRI | Radiomics | Tumor response to nCRT | Retrospective | External | AUC, sensitivity, specificity |
| Zhang et al. ( | 2020 | China | Rectal cancer | Diffusion kurtosis MRI | Deep learning | Response to nCRT | Retrospective | External | AUC, accuracy |
| Shin et al. ( | 2022 | Korea | Rectal cancer | MRI | Radiomics | pCR after nCRT | Retrospective | External | AUC, sensitivity, specificity |
| Rengo et al. ( | 2022 | Italy | Rectal cancer | MRI | Classification algorithm | Response to nCRT | Retrospective | External | Accuracy, AUC |
| Shaish et al. ( | 2020 | Multicenter | Rectal cancer | MRI | Radiomics | pCR, TRG, neoadjuvant rectal score | Multicenter retrospective | External | AUC, sensitivity, specificity |
| Horvat et al. ( | 2018 | USA | Rectal cancer | MRI | Radiomics | Treatment response after nCRT | Retrospective | External | AUC, accuracy |
| Bulens et al. ( | 2020 | Belgium | Rectal cancer | MRI | Radiomics | Tumor response to nCRT | Retrospective | External | Accuracy, AUC |
| Xie et al. ( | 2023 | China | Colorectal cancer | CT | Radiomics | Early recurrence prediction | Retrospective | External | AUC, accuracy |
| Fu et al. ( | 2025 | China | Rectal cancer | MRI | Radiomics | Recurrence risk stratification | Multicenter cohort | External | AUC, accuracy |
| Yao et al. ( | 2024 | China | Rectal cancer | MRI | Radiomics | Preoperative recurrence and metastasis prediction | Retrospective | External | AUC, sensitivity, specificity |
| Xie et al. ( | 2024 | China | Early-onset rectal cancer | MRI | Radiomics | Recurrence risk stratification | Multicenter retrospective | External | AUC, accuracy |
| Montagnon et al. ( | 2024 | France | Colorectal cancer liver metastasis | CT | Radiomics | Oncological outcomes post-resection | Retrospective | External | AUC, accuracy |
| Jin et al. ( | 2024 | China | BRAF mutant colorectal cancer | CT | Integrated nomogram | Early recurrence prediction | Retrospective | External | AUC, sensitivity, specificity |
| Sluckin et al. ( | 2023 | Netherlands | Rectal cancer | MRI | Deep learning with explainability | Lateral locoregional recurrence prediction | Retrospective | External | AUC, accuracy |
| Liu et al. ( | 2022 | China | Rectal cancer | RS-EPI DWI MRI | Radiomics + ML | Prognostic risk stratification | Two-center retrospective | External | AUC, accuracy |
| Jayaprakasam et al. ( | 2022 | UK | Rectal cancer | MRI | Radiomics | Response to nCRT and recurrence | Retrospective | External | AUC, sensitivity, specificity |
| Huang et al. ( | 2022 | Taiwan | Stage III colorectal cancer | CT + immune genomic data | Radiomics + immune-genomic integration | Prognostic classification and therapeutic target identification | Retrospective | External | AUC, accuracy |
| Badic et al. ( | 2022 | France | Colorectal cancer | Contrast-enhanced CT | Radiomics | Post-surgery recurrence prediction | Two-center retrospective | External | AUC, accuracy |
| Fan et al. ( | 2021 | China | Stage II colorectal cancer | CT | Radiomics | Postoperative recurrence risk | Retrospective | External | AUC, accuracy |
| Chen et al. ( | 2021 | China | Rectal cancer | MRI | Radiomics | Local recurrence at anastomosis site | Retrospective | External | AUC, accuracy |
| Dai et al. ( | 2020 | China | Stage I–III colon cancer | CT | Radiomics | Prognostic and predictive value | Retrospective | External | AUC, accuracy |
| Xia et al. ( | 2020 | China | Stage I lung adenocarcinoma | CT | Deep learning + Radiomics | Invasiveness risk prediction | Retrospective | External | AUC, accuracy |
| Zhong et al. ( | 2024 | China | Gastric cancer | Enhanced CT | Deep learning radiomics nomogram | Metastatic lymph node response to nCT | Retrospective | External | AUC, accuracy |
| Wang et al. ( | 2022 | China | Colorectal cancer lung metastasis | CT + histopathology | DL-pathomics + Radiomics + Immunoscore | Postoperative outcome prediction | Retrospective | External | AUC, accuracy |
| Xiang et al. ( | 2022 | China | Anti-NMDA receptor encephalitis | MRI + clinical | Deep learning + Radiomics | Prognosis prediction | Two-center retrospective | External | AUC, accuracy |
| Song et al. ( | 2022 | China | Locally advanced gastric cancer | CT | Radiomics | Response to neoadjuvant chemotherapy | Dual-center retrospective | External | AUC, accuracy |
| Xie et al. ( | 2021 | China | Locally advanced gastric cancer | Contrast-enhanced CT | Radiomics | Pathological regression post-nCT | Multicenter preliminary | External | AUC, accuracy |
| Huang et al. ( | 2022 | China | Advanced adenocarcinoma of esophagogastric junction | Enhanced CT | Radiomics | Pathological complete response post-nCT | Two-center retrospective | External | AUC, accuracy |
| Cui et al. ( | 2022 | China | Locally advanced gastric cancer | CT | Deep learning + Radiomics nomogram | Response to neoadjuvant chemotherapy | Multicenter cohort | External | AUC, accuracy |
| Chen et al. ( | 2022 | China | Advanced gastric cancer | CT | Radiomics | Tumor regression grade prediction post-nCT | Retrospective | External | AUC, accuracy |
| Hu et al. ( | 2023 | China | Locally advanced gastric cancer | Pretreatment CT | Deep learning + radioclinical signatures | Neoadjuvant chemotherapy response and prognosis | Retrospective | External | AUC, accuracy |
| Liu et al. ( | 2021 | China | Advanced gastric cancer | Dual-energy CT | Radiomics | Chemotherapy response prediction | Pilot retrospective | External | AUC, accuracy |
| Sun et al. ( | 2020 | China | Gastric cancer | CT | Radiomics | Response to neoadjuvant chemotherapy and survival | Retrospective | External | AUC, accuracy, survival |
| Zhang et al. ( | 2022 | China | Locally advanced gastric cancer | CT | Deep learning | Chemotherapy resistance prediction | Multicenter retrospective | External | AUC, accuracy |
| Shen et al. ( | 2018 | China | Esophageal cancer | CT | Radiomics nomogram | Preoperative lymph node metastasis | Retrospective | External | AUC, accuracy |
| Li et al. ( | 2021 | China | Esophageal carcinoma | CT | Clinical-radiomics model | Lymph node metastasis prediction | Retrospective | External | AUC, accuracy |
| Ou et al. ( | 2021 | China | Advanced esophageal squamous cell carcinoma | CT | Radiomics | Lymph node metastasis prediction | Case-control | External | AUC, accuracy |
| Tan et al. ( | 2019 | China | Resectable esophageal squamous cell carcinoma | CT | Radiomics nomogram | Lymph node metastasis discrimination | Retrospective | External | AUC, accuracy |
| Qu et al. ( | 2019 | China | Esophageal cancer | MRI | Radiomics | Preoperative lymph node metastasis | Retrospective | External | AUC, accuracy |
| Larue et al. ( | 2018 | Netherlands | Esophageal cancer | CT | Radiomics | 3-year overall survival post-chemoradiotherapy | Retrospective | External | AUC, survival |
| Yang et al. ( | 2021 | China | Early esophageal squamous cell cancer | Endoscopy | Real-time AI | Endoscopic diagnosis | Prospective | External | Accuracy, sensitivity, specificity |
| Hou et al. ( | 2017 | China | Esophageal carcinoma | Contrast-enhanced CT | Radiomics | Predict treatment response to chemoradiotherapy | Retrospective | Internal | AUC 0.79 |
| Jin et al. ( | 2019 | China | Esophageal cancer | CT + dosimetry | Radiomics + combined features | Response after chemoradiation | Retrospective | Internal | AUC 0.81 |
| Li et al. ( | 2021 | China | Esophageal carcinoma | CT | 3D Deep learning | Pretreatment evaluation of treatment response | Prospective | Internal | Accuracy 0.83 |
| Boldrini et al. ( | 2022 | Italy | Rectal cancer | MRI | Radiomics | Predict pathological complete response (pCR) | Multicenter cohort | External | AUC 0.81 |
| Cheng et al. ( | 2021 | China | Rectal cancer | Multiparametric MRI | Radiomics | Predict response to neoadjuvant chemoradiotherapy | Retrospective | Internal | AUC 0.78 |
| Wan et al. ( | 2019 | China | Rectal cancer | MRI | Radiomics | Predict pCR after neoadjuvant chemoradiotherapy | Retrospective | Internal | AUC 0.76 |
| Zhu et al. ( | 2022 | China | Rectal cancer | MRI (multiple b-values) | Radiomics signatures | Predict treatment response | Retrospective | Internal | Accuracy 0.79 |
| Jang et al. ( | 2021 | Korea | Rectal cancer | Post-CRT MRI | Deep learning | Predict pathological response | Retrospective | Internal | Accuracy 0.81 |
| Lee et al. ( | 2021 | Korea | Rectal cancer | MRI | Radiomics + deep embedding network | Predict pCR | Retrospective | Internal | AUC 0.82 |
| Nardone et al. ( | 2022 | Italy | Rectal cancer | MRI | Delta radiomics | Predict complete pathological response | Retrospective | Internal | AUC 0.80 |
| Antunes et al. ( | 2020 | USA | Rectal cancer | Baseline T2-weighted MRI | Radiomics | Associated with pCR | Multisite study | External | AUC 0.77 |
| Horvat et al. ( | 2022 | USA | Rectal cancer | MRI | AI + Radiologist model | Predict treatment response | External validation study | External | AUC 0.83 |
| Echle et al. ( | 2020 | Germany | Colorectal cancer | Histology slides | Deep learning | Detect MSI | Retrospective | External | AUC 0.96 |
| Pressman et al. ( | 2020 | USA | Colorectal cancer | Histology slides | Deep learning | Predict MSI across ethnic groups | Retrospective | Internal | Accuracy 0.82 |
| Cao et al. ( | 2020 | China | Colorectal cancer | Pathology images | Pathomics-based model | Predict MSI | Retrospective | Internal | AUC 0.87 |
| Valieris et al. ( | 2020 | Brazil | Breast and Gastric cancer | Histology images | Deep learning | Predict features with therapeutic relevance | Retrospective | Internal | Accuracy 0.81 |
| Krause et al. ( | 2021 | Germany | Colorectal cancer | Histology slides | Adversarial deep learning | Detect genetic alterations | Retrospective | Internal | Accuracy 0.79 |
| Hong et al. ( | 2021 | USA | Endometrial cancer | Histopathology images | Multi-resolution deep learning | Predict subtypes and molecular features | Retrospective | Internal | Accuracy 0.84 |
|
|
|
|
|
|
|
|
|---|---|---|---|---|---|---|
| Luo, 2019 | 2 | 2 | 3 | 2 | 1 | 10 |
| Zhang, 2023 | 2 | 3 | 4 | 3 | 2 | 14 |
| Wang, 2025 | 3 | 3 | 3 | 2 | 3 | 14 |
| Rengo, 2023 | 3 | 4 | 4 | 2 | 2 | 15 |
| Hirata, 2025 | 3 | 3 | 3 | 2 | 3 | 14 |
| Xie, 2025 | 3 | 4 | 4 | 2 | 3 | 16 |
| Bates, 2022 | 3 | 3 | 3 | 2 | 2 | 13 |
| Wu, 2022 | 2 | 3 | 4 | 3 | 3 | 15 |
| Kominami, 2016 | 2 | 2 | 2 | 2 | 2 | 10 |
| Li, 2023 | 3 | 3 | 3 | 3 | 3 | 15 |
| Barua, 2022 | 3 | 3 | 3 | 2 | 2 | 13 |
| Mori, 2018 | 3 | 3 | 3 | 3 | 3 | 15 |
| Minegishi, 2022 | 3 | 3 | 3 | 3 | 3 | 15 |
| Rodriguez-Diaz, 2022 | 2 | 3 | 3 | 2 | 2 | 12 |
| Dos Santos, 2023 | 2 | 3 | 3 | 2 | 2 | 12 |
| Rondonotti, 2023 | 3 | 3 | 3 | 3 | 3 | 15 |
| Houwen, 2023 | 3 | 3 | 3 | 3 | 3 | 15 |
| Quan, 2022 | 3 | 3 | 3 | 3 | 3 | 15 |
| Galvis-García, 2023 | 3 | 3 | 3 | 2 | 2 | 13 |
| Zhang, 2023 | 3 | 4 | 4 | 2 | 3 | 16 |
| Ahmad, 2022 | 3 | 3 | 3 | 2 | 3 | 14 |
| Lei, 2023 | 3 | 3 | 3 | 3 | 3 | 15 |
| Eckhoff, 2023 | 3 | 3 | 3 | 2 | 3 | 14 |
| Blum, 2024 | 3 | 3 | 3 | 2 | 3 | 14 |
| Hsu, 2023 | 3 | 3 | 3 | 2 | 3 | 14 |
| Athanasiadis, 2025 | 2 | 3 | 3 | 2 | 2 | 12 |
| Han, 2025 | 3 | 3 | 3 | 2 | 3 | 14 |
| Sato, 2022 | 3 | 3 | 3 | 2 | 3 | 14 |
| Niikura, 2022 | 3 | 3 | 3 | 2 | 3 | 14 |
| Yang, 2022 | 3 | 3 | 3 | 2 | 3 | 14 |
| Schnelldorfer, 2024 | 3 | 4 | 4 | 2 | 3 | 16 |
| Guo, 2021 | 3 | 3 | 3 | 2 | 3 | 14 |
| Tatar, 2024 | 3 | 3 | 3 | 2 | 3 | 14 |
| van de Sande, 2022 | 3 | 4 | 4 | 3 | 3 | 17 |
| Choi, 2024 | 3 | 3 | 3 | 2 | 3 | 14 |
| Haak, 2022 | 3 | 4 | 4 | 2 | 3 | 16 |
| Noar, 2023 | 3 | 3 | 3 | 2 | 3 | 14 |
| Choi, 2022 | 3 | 3 | 3 | 2 | 3 | 14 |
| Inaba, 2024 | 3 | 3 | 3 | 2 | 3 | 14 |
| Wu, 2021 | 3 | 3 | 3 | 3 | 3 | 15 |
| Rondonotti, 2023 | 3 | 3 | 3 | 3 | 3 | 15 |
| Koh, 2023 | 3 | 3 | 3 | 3 | 3 | 15 |
| Yuan, 2022 | 3 | 3 | 3 | 2 | 3 | 14 |
| Sudarevic, 2023 | 3 | 3 | 3 | 2 | 2 | 13 |
| Tsuboi, 2020 | 3 | 3 | 3 | 2 | 2 | 13 |
| Chang, 2022 | 3 | 3 | 3 | 2 | 2 | 13 |
| Hwang, 2021 | 3 | 3 | 3 | 2 | 2 | 13 |
| Meinikheim, 2024 | 3 | 3 | 3 | 3 | 3 | 15 |
| Tian, 2024 | 3 | 3 | 3 | 3 | 3 | 15 |
| He, 2020 | 3 | 3 | 3 | 2 | 2 | 13 |
| Huo, 2024 | 3 | 3 | 3 | 3 | 3 | 15 |
| Zhang, 2018 | 3 | 3 | 3 | 2 | 2 | 13 |
| Klaiman, 2019 | 3 | 3 | 3 | 2 | 3 | 14 |
| Kather, 2019 | 3 | 3 | 3 | 2 | 3 | 14 |
| Kather, 2020 | 3 | 3 | 3 | 2 | 3 | 14 |
| Schmauch, 2020 | 3 | 4 | 4 | 2 | 3 | 16 |
| Cui, 2019 | 3 | 3 | 3 | 2 | 3 | 14 |
| Feng, 2022 | 3 | 4 | 4 | 3 | 3 | 17 |
| Jin, 2021 | 3 | 4 | 4 | 2 | 3 | 16 |
| Pang, 2021 | 3 | 4 | 4 | 2 | 3 | 16 |
| Wan, 2021 | 3 | 3 | 3 | 2 | 3 | 14 |
| Yi, 2019 | 3 | 3 | 3 | 2 | 3 | 14 |
| Zhang, 2020 | 3 | 4 | 4 | 2 | 3 | 16 |
| Shin, 2022 | 3 | 4 | 4 | 2 | 3 | 16 |
| Rengo, 2022 | 3 | 4 | 4 | 3 | 3 | 17 |
| Shaish, 2020 | 3 | 4 | 4 | 3 | 3 | 17 |
| Horvat, 2018 | 3 | 3 | 3 | 2 | 2 | 13 |
| Bulens, 2020 | 3 | 4 | 4 | 3 | 3 | 17 |
| Xie, 2023 | 2 | 4 | 3 | 3 | 2 | 14 |
| Fu, 2025 | 3 | 3 | 4 | 2 | 3 | 15 |
| Yao, 2024 | 2 | 4 | 4 | 3 | 3 | 16 |
| Xie, 2024 | 3 | 5 | 3 | 3 | 2 | 16 |
| Montagnon, 2024 | 2 | 3 | 4 | 3 | 3 | 15 |
| Jin, 2024 | 3 | 4 | 4 | 2 | 3 | 16 |
| Sluckin, 2023 | 3 | 3 | 3 | 3 | 3 | 15 |
| Liu, 2022 | 2 | 4 | 3 | 2 | 3 | 14 |
| Jayaprakasam, 2022 | 3 | 4 | 4 | 3 | 3 | 17 |
| Huang, 2022 | 3 | 5 | 4 | 2 | 3 | 17 |
| Badic, 2022 | 2 | 3 | 3 | 2 | 2 | 12 |
| Fan, 2021 | 3 | 4 | 4 | 3 | 3 | 17 |
| Chen, 2021 | 2 | 3 | 3 | 2 | 2 | 12 |
| Dai, 2020 | 3 | 4 | 4 | 3 | 3 | 17 |
| Xia, 2020 | 2 | 4 | 3 | 2 | 2 | 13 |
| Zhong, 2024 | 3 | 5 | 4 | 3 | 3 | 18 |
| Wang, 2022 | 3 | 4 | 4 | 3 | 3 | 17 |
| Xiang, 2022 | 3 | 3 | 4 | 3 | 2 | 15 |
| Song, 2022 | 2 | 4 | 4 | 3 | 3 | 16 |
| Xie, 2021 | 3 | 4 | 3 | 2 | 3 | 15 |
| Huang, 2022 | 3 | 4 | 4 | 3 | 3 | 17 |
| Cui, 2022 | 3 | 4 | 5 | 3 | 4 | 19 |
| Chen, 2022 | 2 | 4 | 4 | 2 | 3 | 15 |
| Hu, 2023 | 3 | 5 | 4 | 4 | 3 | 19 |
| Liu, 2021 | 2 | 3 | 3 | 2 | 2 | 12 |
| Sun, 2020 | 3 | 4 | 5 | 3 | 4 | 19 |
| Zhang, 2022 | 3 | 3 | 4 | 4 | 3 | 17 |
| Shen, 2018 | 2 | 3 | 3 | 2 | 2 | 12 |
| Li, 2021 | 3 | 4 | 4 | 3 | 3 | 17 |
| Ou, 2021 | 2 | 3 | 3 | 3 | 2 | 13 |
| Tan, 2019 | 2 | 4 | 4 | 2 | 3 | 15 |
| Qu, 2019 | 3 | 4 | 3 | 2 | 3 | 15 |
| Larue, 2018 | 2 | 3 | 3 | 3 | 2 | 13 |
| Yang, 2021 | 3 | 5 | 4 | 4 | 4 | 20 |
| Hou, 2017 | 2 | 3 | 3 | 2 | 2 | 12 |
| Jin, 2019 | 3 | 4 | 4 | 3 | 3 | 17 |
| Li, 2021 | 3 | 5 | 5 | 4 | 4 | 21 |
| Boldrini, 2022 | 3 | 4 | 4 | 3 | 3 | 17 |
| Cheng, 2021 | 3 | 4 | 5 | 4 | 4 | 20 |
| Wan, 2019 | 2 | 3 | 3 | 2 | 3 | 13 |
| Zhu, 2022 | 3 | 3 | 4 | 3 | 3 | 16 |
| Jang, 2021 | 3 | 5 | 4 | 3 | 4 | 19 |
| Lee, 2021 | 3 | 4 | 5 | 4 | 3 | 19 |
| Nardone, 2022 | 2 | 4 | 4 | 3 | 3 | 16 |
| Antunes, 2020 | 3 | 5 | 5 | 4 | 4 | 21 |
| Horvat, 2022 | 3 | 4 | 4 | 3 | 3 | 17 |
| Echle, 2020 | 3 | 5 | 5 | 4 | 4 | 21 |
| Pressman, 2020 | 2 | 4 | 4 | 3 | 3 | 16 |
| Cao, 2020 | 3 | 4 | 5 | 4 | 4 | 20 |
| Valieris, 2020 | 3 | 5 | 4 | 3 | 4 | 19 |
| Krause, 2021 | 3 | 4 | 5 | 4 | 4 | 20 |
| Hong, 2021 | 3 | 5 | 4 | 3 | 4 | 19 |
|
|
|
|
|
|
|
|
|
|---|---|---|---|---|---|---|---|
| Luo, 2019 | Multicenter, case-control, diagnostic | Low | Low | Low | Low | Unlikely | High |
| Zhang, 2023 | Multicenter, diagnostic AI | Low | Low | Low | Low | Unlikely | High |
| Wang, 2025 | Development and clinical validation, deep learning | Moderate | Low | Low | Moderate | Possible | Moderate |
| Rengo, 2023 | Multicenter, AI radiomics | Low | Low | Low | Low | Unlikely | High |
| Hirata, 2025 | Retrospective AI MRI radiomics | Moderate | Low | Low | Moderate | Possible | Moderate |
| Xie, 2025 | Multimodal AI integration | Low | Low | Low | Low | Unlikely | High |
| Bates, 2022 | Observational AI body composition study | Moderate | Moderate | Low | Moderate | Possible | Moderate |
| Wu, 2022 | Multicenter AI prediction, retrospective | Moderate | Low | Low | Moderate | Possible | Moderate |
| Kominami, 2016 | Prospective image recognition system | Low | Low | Low | Low | Unlikely | High |
| Li, 2023 | Prospective multicenter validation | Low | Low | Low | Low | Unlikely | High |
| Barua, 2022 | Real-time AI optical diagnosis | Low | Low | Low | Low | Unlikely | High |
| Mori, 2018 | Prospective, multicenter | Low | Low | Low | Low | Unlikely | High |
| Minegishi, 2022 | Prospective, multicenter | Low | Low | Low | Moderate | Possible | Moderate |
| Rodriguez-Diaz, 2022 | Diagnostic AI study, single-center | Moderate | Low | Low | Moderate | Possible | Moderate |
| Dos Santos, 2023 | Diagnostic AI study, multicenter | Low | Low | Low | Low | Unlikely | High |
| Rondonotti, 2023 | Prospective multicenter | Low | Low | Low | Low | Unlikely | High |
| Houwen, 2023 | Prospective, multicenter | Low | Low | Low | Low | Unlikely | High |
| Quan, 2022 | Pilot multicenter | Moderate | Low | Low | Moderate | Possible | Moderate |
| Galvis-García, 2023 | Prospective, single-center | Moderate | Low | Low | Moderate | Possible | Moderate |
| Zhang, 2023 | Diagnostic and computational model | Moderate | Low | Low | Moderate | Possible | Moderate |
| Ahmad, 2022 | Prospective multicenter | Low | Low | Low | Low | Unlikely | High |
| Lei, 2023 | Prospective AI capsule endoscopy | Moderate | Low | Low | Moderate | Possible | Moderate |
| Eckhoff, 2023 | Multicenter, surgical AI | Low | Low | Low | Low | Unlikely | High |
| Blum, 2024 | Prospective AI for biliary diagnosis | Moderate | Low | Low | Moderate | Possible | Moderate |
| Hsu, 2023 | Retrospective surgical AI | Moderate | Low | Low | Moderate | Possible | Moderate |
| Athanasiadis, 2025 | Prospective surgical evaluation | Moderate | Low | Low | Moderate | Possible | Moderate |
| Han, 2025 | Prospective AI nerve recognition | Moderate | Low | Low | Moderate | Possible | Moderate |
| Sato, 2022 | Prospective, multicenter | Low | Low | Low | Low | Unlikely | High |
| Niikura, 2022 | Multicenter, comparative AI vs. experts | Low | Low | Low | Low | Unlikely | High |
| Yang, 2022 | Diagnostic AI endoscopic ultrasound | Low | Low | Low | Low | Unlikely | High |
| Schnelldorfer, 2024 | Prospective deep learning intraoperative | Moderate | Low | Low | Moderate | Possible | Moderate |
| Guo, 2021 | Pilot AI detection, single-center | Moderate | Moderate | Low | Moderate | Possible | Moderate |
| Tatar, 2024 | Prospective surgical AI | Moderate | Low | Low | Moderate | Possible | Moderate |
| van de Sande, 2022 | Multicenter AI decision support | Low | Low | Low | Low | Unlikely | High |
| Choi, 2024 | Deep learning capsule endoscopy | Moderate | Low | Low | Moderate | Possible | Moderate |
| Haak, 2022 | Deep learning evaluation of response | Moderate | Low | Low | Moderate | Possible | Moderate |
| Noar, 2023 | Prospective AI for gastric function | Moderate | Low | Low | Moderate | Possible | Moderate |
| Choi, 2022 | AI quality control endoscopy | Moderate | Low | Low | Moderate | Possible | Moderate |
| Inaba, 2024 | Smartphone AI, prospective | Moderate | Low | Low | Moderate | Possible | Moderate |
| Wu, 2021 | Randomized controlled trial, AI endoscopy | Low | Low | Low | Low | Unlikely | High |
| Rondonotti, 2023 | Prospective multicenter | Low | Low | Low | Low | Unlikely | High |
| Koh, 2023 | Prospective cohort | Moderate | Low | Low | Moderate | Possible | Moderate |
| Yuan, 2022 | Prospective, multicenter | Low | Low | Low | Low | Unlikely | High |
| Sudarevic, 2023 | Prospective, single-center | Moderate | Low | Low | Moderate | Possible | Moderate |
| Tsuboi, 2020 | Retrospective AI capsule study | Moderate | Moderate | Low | Moderate | Possible | Moderate |
| Chang, 2022 | Prospective AI endoscopy | Moderate | Low | Low | Moderate | Possible | Moderate |
| Hwang, 2021 | Retrospective capsule AI | Moderate | Low | Low | Moderate | Possible | Moderate |
| Meinikheim, 2024 | RCT, multicenter | Low | Low | Low | Low | Unlikely | High |
| Tian, 2024 | Retrospective multicenter | Moderate | Low | Low | Moderate | Possible | Moderate |
| He, 2020 | Retrospective AI study | Moderate | Low | Low | Moderate | Possible | Moderate |
| Huo, 2024 | Prospective AI-assisted decision-making | Moderate | Low | Low | Moderate | Possible | Moderate |
| Zhang, 2018 | Retrospective histopathology AI | Moderate | Moderate | Low | Moderate | Possible | Moderate |
| Klaiman, 2019 | Retrospective histopathology AI | Moderate | Low | Low | Moderate | Possible | Moderate |
| Kather, 2019 | Retrospective histopathology AI | Moderate | Low | Low | Moderate | Possible | Moderate |
| Kather, 2020 | Retrospective pan-cancer AI | Moderate | Low | Low | Moderate | Possible | Moderate |
| Schmauch, 2020 | Retrospective deep learning RNA prediction | Moderate | Moderate | Low | Moderate | Possible | Moderate |
| Cui, 2019 | Retrospective radiomics | Moderate | Low | Low | Moderate | Possible | Moderate |
| Feng, 2022 | Multicenter radiopathomics | Low | Low | Low | Low | Unlikely | High |
| Jin, 2021 | Retrospective longitudinal MRI AI | Moderate | Low | Low | Moderate | Possible | Moderate |
| Pang, 2021 | Retrospective radiomics + deep learning | Moderate | Low | Low | Moderate | Possible | Moderate |
| Wan, 2021 | Retrospective delta-radiomics | Moderate | Low | Low | Moderate | Possible | Moderate |
| Yi, 2019 | Retrospective MRI radiomics | Moderate | Low | Low | Moderate | Possible | Moderate |
| Zhang, 2020 | Retrospective MRI deep learning | Moderate | Low | Low | Moderate | Possible | Moderate |
| Shin, 2022 | Prospective radiomics validation | Low | Low | Low | Low | Unlikely | High |
| Rengo, 2022 | Multicenter radiomics classification | Low | Low | Low | Low | Unlikely | High |
| Shaish, 2020 | Multicenter MRI radiomics | Low | Low | Low | Moderate | Possible | High |
| Horvat, 2018 | Retrospective MRI radiomics | Moderate | Low | Low | Moderate | Possible | Moderate |
| Bulens, 2020 | Multicenter MRI radiomics | Low | Low | Low | Low | Unlikely | High |
| Xie, 2023 | Multicenter MRI radiomics | Low | Low | Low | Low | Unlikely | High |
| Fu, 2025 | Multicenter MRI radiomics | Low | Low | Low | Low | Unlikely | High |
| Yao, 2024 | Multicenter MRI radiomics | Low | Low | Low | Low | Unlikely | High |
| Xie, 2024 | Multicenter MRI radiomics | Low | Low | Low | Low | Unlikely | High |
| Montagnon, 2024 | Multicenter CT radiomics | Low | Low | Low | Low | Unlikely | High |
| Jin, 2024 | Retrospective nomogram, single-center | Moderate | Low | Low | Moderate | Possible | Moderate |
| Sluckin, 2023 | Retrospective deep learning | Moderate | Low | Low | Moderate | Possible | Moderate |
| Liu, 2022 | Multicenter RS-EPI DWI radiomics | Low | Low | Low | Low | Unlikely | High |
| Jayaprakasam, 2022 | Retrospective MRI radiomics | Moderate | Low | Low | Moderate | Possible | Moderate |
| Huang, 2022 | Multicenter CT + genomics | Low | Low | Low | Low | Unlikely | High |
| Badic, 2022 | Multicenter CT radiomics | Low | Low | Low | Low | Unlikely | High |
| Fan, 2021 | Retrospective CT radiomics | Moderate | Low | Low | Moderate | Possible | Moderate |
| Chen, 2021 | Retrospective MRI radiomics | Moderate | Low | Low | Moderate | Possible | Moderate |
| Dai, 2020 | Retrospective CT radiomics | Moderate | Low | Low | Moderate | Possible | Moderate |
| Xia, 2020 | Retrospective deep learning + radiomics | Moderate | Low | Low | Moderate | Possible | Moderate |
| Zhong, 2024 | Multicenter CT deep learning radiomics | Low | Low | Low | Low | Unlikely | High |
| Wang, 2022 | Multicenter CT + deep learning + radiomics | Low | Low | Low | Low | Unlikely | High |
| Xiang, 2022 | Multicenter deep learning + clinical variables | Low | Low | Low | Low | Unlikely | High |
| Song, 2022 | Dual-center CT radiomics | Low | Low | Low | Low | Unlikely | High |
| Xie, 2021 | Multicenter CT radiomics | Low | Low | Low | Low | Unlikely | High |
| Huang, 2022 | Two-center CT radiomics | Low | Low | Low | Low | Unlikely | High |
| Cui, 2022 | Multicenter CT deep learning radiomics | Low | Low | Low | Low | Unlikely | High |
| Chen, 2022 | Multicenter CT radiomics | Low | Low | Low | Low | Unlikely | High |
| Hu, 2023 | Multicenter CT deep learning radiomics | Low | Low | Low | Low | Unlikely | High |
| Liu, 2021 | Pilot CT radiomics | Moderate | Low | Low | Moderate | Possible | Moderate |
| Sun, 2020 | Retrospective CT radiomics | Moderate | Low | Low | Moderate | Possible | Moderate |
| Zhang, 2022 | Multicenter deep learning CT | Low | Low | Low | Low | Unlikely | High |
| Shen, 2018 | Retrospective CT radiomics | Moderate | Low | Low | Moderate | Possible | Moderate |
| Li, 2021 | Retrospective CT radiomics | Moderate | Low | Low | Moderate | Possible | Moderate |
| Ou, 2021 | Retrospective CT radiomics | Moderate | Low | Low | Moderate | Possible | Moderate |
| Tan, 2019 | Retrospective CT radiomics | Moderate | Low | Low | Moderate | Possible | Moderate |
| Qu, 2019 | Retrospective MRI radiomics | Moderate | Low | Low | Moderate | Possible | Moderate |
| Larue, 2018 | Retrospective CT radiomics | Moderate | Low | Low | Moderate | Possible | Moderate |
| Yang, 2021 | Prospective AI endoscopy | Low | Low | Low | Low | Unlikely | High |
| Hou, 2017 | Retrospective CT radiomics | Moderate | Low | Low | Moderate | Possible | Moderate |
| Jin, 2019 | Retrospective CT + dosimetry | Moderate | Low | Low | Moderate | Possible | Moderate |
| Li, 2021 | Prospective 3D deep learning | Low | Low | Low | Low | Unlikely | High |
| Boldrini, 2022 | Multicenter MRI radiomics | Low | Low | Low | Low | Unlikely | High |
| Cheng, 2021 | Retrospective multiparametric MRI radiomics | Moderate | Low | Low | Moderate | Possible | Moderate |
| Wan, 2019 | Retrospective MRI radiomics | Moderate | Low | Low | Moderate | Possible | Moderate |
| Zhu, 2022 | Retrospective MRI radiomics | Moderate | Low | Low | Moderate | Possible | Moderate |
| Jang, 2021 | Deep learning MRI post-CRT | Low | Low | Low | Low | Unlikely | High |
| Lee, 2021 | Deep learning MSI classification | Low | Low | Low | Low | Unlikely | High |
| Nardone, 2022 | Retrospective delta radiomics | Moderate | Low | Low | Moderate | Possible | Moderate |
| Antunes, 2020 | Multisite MRI radiomics | Low | Low | Low | Low | Unlikely | High |
| Horvat, 2022 | Multicenter MRI AI + radiologist | Low | Low | Low | Low | Unlikely | High |
| Echle, 2020 | Deep learning MSI detection | Low | Low | Low | Low | Unlikely | High |
| Pressman, 2020 | Deep learning MSI across ethnicities | Low | Low | Low | Low | Unlikely | High |
| Cao, 2020 | Pathomics-based MSI prediction | Low | Low | Low | Low | Unlikely | High |
| Valieris, 2020 | Deep learning pathology features | Low | Low | Low | Low | Unlikely | High |
| Krause, 2021 | Deep learning genetic alterations | Low | Low | Low | Low | Unlikely | High |
| Hong, 2021 | Multi-resolution deep learning pathology | Low | Low | Low | Low | Unlikely | High |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsRadiomics and Machine Learning in Medical Imaging · Gastric Cancer Management and Outcomes · Colorectal Cancer Screening and Detection
Introduction
1
Digestive system neoplasms, which include cancers of the esophagus, stomach, liver, pancreas, biliary tract, small intestine, and colorectal area, continue to pose a great challenge to global health. In line with recent epidemiological research, the whole group of gastrointestinal (GI) cancers is responsible for a considerable part of the cancer-related morbidity and mortality in the world, with colorectal, gastric, and liver cancers being the main ones in terms of incidence and mortality. Although there have been significant improvements in surgery, chemoradiotherapy, and targeted therapies, the clinical results are still very different from each other due to the different tumor biologies, molecular characteristics, and patient factors. The exact prediction of tumor response to therapy, recurrence risk, and prognosis is very important for individualized treatment planning, early intervention, and better patient outcomes (1–5).
Traditional imaging methods such as computed tomography (CT), magnetic resonance imaging (MRI), endoscopy, and histopathological assessment have been the main techniques used for diagnosis and staging. Nevertheless, these methods still depend a lot on image interpretation by professionals, which may be insufficient for the detection of very subtle phenotypic and microstructural tumor characteristics. One of the main aspects of radiomics is the imaging data transformation, which is a non-invasive method of tumor characterization, heterogeneity, and microenvironment interrogation through standard care imaging studies. This way, radiomics extracts hundreds to thousands of high-dimensional features from different imaging modalities, reflecting tumor shape, texture, intensity, and spatial heterogeneity, using only the imaging studies. These features have the capacity to detect previously hidden biological and molecular properties and thus are considered to be the link connecting the realms of imaging, pathology, and genomics. The application of radiomic signatures correlated with tumor grading, staging, treatment response, recurrence risk, and survival in a number of cancers affecting the digestive system. Notably, the radiomics technique supports continuous evaluation, thus making it possible to monitor the tumor changes dynamically during therapy (6–10).
Artificial intelligence (AI), especially machine learning (ML) and deep learning (DL) methods, has been the main factor that improved the interpretative power of radiomics. AI algorithms are capable of combining high-dimensional radiomic features with clinical, laboratory, genomic, and histopathological data to create highly accurate and reproducible predictive and prognostic models. Deep convolutional neural networks (CNNs) allow the automated detection, segmentation, and classification of tumors from imaging datasets, thus decreasing observer variability and raising diagnostic efficiency. For gastrointestinal cancers, AI-based radiomics models have been used to predict the pathological complete response after neoadjuvant therapy, locate the high-risk lesions during endoscopy or imaging, stratify the patients according to their recurrence risk, and guide the surgical or therapeutic decision-making processes. The models give practical and useful information that can be applied, thus enabling personalized medicine and optimizing resource allocation (11–16).
Systematic reviews and meta-analyses are a comprehensive method of synthesizing the existing evidence, assessing the efficacy, consistency, and reliability of the radiomics and AI-based predictive models. They provide a comprehensive approach to performing this task. Meta-analyses, by quantitatively combining data from several studies, can find summary effect sizes, assess the degree of variation, uncover publication bias, and point out the areas with little or no literature. Tumor diversity in the gastrointestinal system, the requirement of various imaging modalities, and the variety of clinical practices are factors that contribute to the great difficulty in estimating treatment response and prognosis. This indeed renders the situation very important (17–20). The systematic review and meta-analysis aims to reveal the clinical function, barriers, and next steps of the application of radiomics and AI in gastrointestinal tumors.
Methodology
2
Study design and protocol
2.1
This systematic review and meta-analysis were executed in accordance with the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines. Beforehand, a comprehensive protocol was drafted that described the research question, criteria for including and excluding studies, search strategy, data extraction, quality assessment, and statistical analysis. The main goal was to compare the diagnostic and prognostic abilities of the radiomics and AI-based predictive models in the case of digestive system neoplasms—thus, the focus was on colorectal, gastric, esophageal, pancreatic, hepatic, biliary, and small bowel cancer.
Literature search strategy
2.2
A literature search was performed using PubMed, Embase, Scopus, Web of Science, and Cochrane Library databases, and covered studies published from January 2016 to December 2025, thus being comprehensive. The search terms used were a combination of Medical Subject Headings (MeSH) and keywords associated with “radiomics,” “artificial intelligence,” “deep learning,” “machine learning,” “tumor response,” “predictive models,” “gastrointestinal cancer,” “colorectal cancer,” “gastric cancer,” “esophageal cancer,” and “digestive system neoplasms.” Truncation, synonyms, and Boolean operators were also used in order to reach the highest sensitivity possible. The reference lists of pertinent articles were checked manually to find any more studies that would meet the eligibility requirements.
Inclusion and exclusion criteria
2.3
The inclusion was determined based on the following criteria: radiomics or AI-based models were developed that predicted tumor response, recurrence, or prognosis in the case of digestive system malignancies. sufficient statistical outcomes were reported (for example, odds ratios, area under the curve, sensitivity, and specificity). imaging (CT, MRI, PET, or endoscopy) and histopathology or molecular data were used. The study was an original research article, be it a prospective, retrospective, or multicenter one. The reasons for exclusion were as follows: (1) reviews, editorials, letters, conference abstracts that did not have full data; (2) animal or in vitro studies; (3) non-quantitative predictive performance reporting studies; and (4) non-English publications. The researchers focused on detecting potential dataset overlaps because AI research increasingly uses institutional registries and public imaging repositories as their fundamental data sources. The research team conducted thorough examination of recruitment periods and institutional affiliations and patient characteristics whenever they detected potential overlap between two groups. The research team selected the study which presented either the most extensive dataset or the highest research standards as their primary source when they encountered substantial duplication. The research found that some studies assessed multiple artificial intelligence models which were developed from the same group of patients. The researchers included these models in their study because they assessed different clinical outcomes through their distinct research methods which reduced their dependency on one another and reduced the possibility of false precision results in the meta-analysis.
Data extraction
2.4
The reviewers screened independently and in pairs the titles, abstracts, and full texts. Any discrepancies that arose were either resolved by the discussion between the pair of reviewers or by consultation with a third reviewer. The data that was extracted consisted of: study characteristics (author, year, country, study design), population details (sample size, tumor type, stage), AI or radiomics methodology (modality, feature extraction, preprocessing, model type, validation approach), predictive outcomes (tumor response, recurrence, survival), statistical measures (odds ratios, confidence intervals, sensitivity, specificity), and information on external validation. Researchers established three main response categories to enhance the ability to compare their findings. Radiologic response was primarily defined using standardized criteria such as the Response Evaluation Criteria in Solid Tumors (RECIST) which assess changes in tumor size on cross-sectional imaging. The assessment of pathological response included both tumor regression grade and the evaluation of pathological complete response after neoadjuvant therapy. Artificial intelligence (AI) systems used progression-free survival and overall survival as treatment response indicators which they modeled through their systems. The ongoing research process creates clinical and methodological differences because institutional practices change and AI-driven research progresses. The variability in endpoint definitions affects radiomics model predictive performance which needs to be considered for interpreting pooled estimates.
Quality assessment
2.5
The methodological quality of studies was determined with the help of the Radiomics Quality Score (RQS) that rates six areas, namely: image acquisition and preprocessing, feature selection and robustness, validation strategies, study design (prospective or multicenter), biological or clinical validation, and open science/data sharing. Furthermore, the Prediction model Risk Of Bias Assessment Tool (PROBAST) was implemented in a four-domain manner—participants, predictors, outcome, and analysis—leading to the overall risk in the form of bias (low, partial, or high) being established.
Statistical analysis
2.6
Random-effects model meta-analysis with inverse variance weighting was the method applied for estimating pooled odds ratios (ORs) and 95% confidence intervals (CIs) for predictive performance in the studies included. Heterogeneity between studies was measured by means of Cochran's Q test and I^2^ statistic, with I^2^ >50% being a sign of substantial heterogeneity. Publication bias was tested by looking at the funnel plots and applying Egger's regression test for asymmetry. Besides, subgroup analyses were performed according to tumor type, imaging modality, AI model type, and study design. Lastly, sensitivity analyses were carried out by successively eliminating individual studies to examine the strength of results.
Data synthesis and reporting
2.7
The results were presented both narratively and quantitatively. Effect sizes were visualized through forest plots, and study characteristics, quality assessments, and predictive performance metrics were summarized in tables. The statistical analysis was done by using Review Manager (RevMan, https://revman.cochrane.org/info) 5.4 and R software (version 4.3.1, https://www.r-project.org/) for all deconstructions.
Results
3
Study selection
3.1
The study selection was done following a strict two-phase screening process aligned with PRISMA guidelines. In the first place, the titles and abstracts of 1,435 papers that came from PubMed, Embase, Scopus, Web of Science, and Cochrane Library were scrutinized separately by two reviewers. The duplicates, irrelevant studies, and non-original research were eliminated. Full text of 218 potentially qualified articles was then evaluated against predefined inclusion and exclusion criteria that were based on AI or radiomics-based prediction of tumor response in digestive system neoplasms. Differences were solved through either discussion or involving a third reviewer. Finally, 120 studies that conformed to all the criteria were included in the systematic review and meta-analysis (Figure 1).
*PRISMA flow chart of study selection. Total record from 5 search sites. ** Record excluded based on incomplete data, not related to study selection criteria.
Study characteristics
3.2
The combined research 120, covering the years 2016–2025, included a wide range of gastrointestinal (GI), colorectal, gastric, esophageal, biliary, and other cancer types from several countries, where China, Japan, the US, and Europe led the way. Among the diverse techniques and data sources used in this study are endoscopic imaging, CT, MRI, capsule endoscopy, digital pathology, histology slides, intraoperative videos, and multimodal clinical/omics datasets. The primary AI techniques employed were convolutional neural networks (CNNs), radiomics, deep learning (DL), computer-aided detection (CAD), multimodal integration, and hybrid AI-radiomics models. The study's aim was concentrated in the areas of early cancer detection, lesion characterization, tumor staging, lymph node metastasis prediction, treatment response assessment, prognostic stratification, surgical guidance, and recurrence risk evaluation, among others. Both prospective and retrospective research designs were employed in single- or multi-center settings. The validation approaches stressed external validation in multicenter or simulated cohorts, while a minor group used internal or two-center validation. Sensitivity, specificity, accuracy, area under the receiver operating characteristic curve (AUC), hazard ratio (HR), survival correlation, predictive accuracy, and calibration measures were among the major performance metrics reported across studies. Together, these studies indicate the continuous and growing integration of AI and radiomics in GI oncology, highlighting the real-time diagnostic applications, treatment response prediction, and precision prognostication, thus underlining both the clinical feasibility and the generalizability of AI-driven models in multicenter and international contexts (Table 1).
PROBAST assessment of AI and radiomics studies
3.3
The Prediction model Risk Of Bias Assessment Tool (PROBAST) table provides a structured evaluation of 120 studies that used AI and radiomics for gastrointestinal, colorectal, esophageal, gastric, biliary, and other cancers, covering the period from 2016 to 2025. Each study was evaluated based on the four core domains: Participants, Predictors, Outcome, and Analysis, and the overall risk of bias was assigned.
In the presented dataset, “L” marks low risk of bias, while “PL” stands for partial or unclear risk, which is often the case due to limited reporting, small sample sizes, or unclear handling of predictors. In general, Participants were well-defined, but there were some differences in inclusion criteria among the studies. Predictor selection and modeling strategies often had partial limitations that reflected variability in feature selection, data preprocessing, or algorithm transparency. Outcome definitions were mainly consistent within each cancer type, but several studies did not have standardized adjudication or blinded assessment. Analytical approaches were partly limited in areas such as overfitting, internal vs. external validation, and missing data management.
By and large, the outcome of most studies was that there was a low to moderate risk of bias, thus being the main concern in the predictors and analysis domains, and partly. The PROBAST assessment not only highlights how AI-based predictive modeling excels but also points out its shortcomings in methodology, thereby necessitating the adoption of more extensive reporting, standard outcome definitions, and strong external validation to win over the clinical trust and applicability (Figures 2A–C).
(A) PROBAST assessment of included studies. Here D1: participants, D2: predictors, D3: outcome, D4: analysis. (B) PROBAST assessment of included studies. Here D1: participants, D2: predictors, D3: outcome, D4: analysis. (C) PROBAST assessment graph of included studies. Here D1: participants, D2: predictors, D3: outcome, D4: analysis.
Radiomics quality score (RQS) in radiomics and AI-based prediction of tumor response in digestive system neoplasms
3.4
In our systematic review and meta-analysis of radiomics and AI-based prediction models for tumor response in digestive system neoplasms, Radiomics Quality Score (RQS) acted as an indicator of the quality of the methods used in the included studies. RQS evaluates the following five areas: image protocol and preprocessing, feature selection and robustness, validation, prospective or multicenter design, and biological or clinical validation.
The majority of studies exhibited very high quality of methods in the image acquisition and preprocessing, thus providing radiomic features that could be reproduced. Feature selection and robustness were mostly significant, suggesting diligence in the trimming of overfitting and the enhancement of generalization. Validation methods differed, with internal, external, and multicenter datasets being used by various studies; studies with external validation and multicenter designs received higher scores, indicating more powerful prediction reliability. Biological or clinical validation—connecting radiomic or AI-based predictions to clinical outcomes—was reported in only a few studies, thus, this is a potential area for improvement.
The total RQS ranged from 10 to 21 across studies, whereby most received a score of moderate to high quality (14–19), thus indicating that although the use of radiomics and AI models in digestive system neoplasms is growing, there is still a need for prospective multicenter validation and integration with clinical endpoints. These RQS results not only confirm the outcomes of the meta-analysis but also highlight the role of quality assessment in the clinical translation of AI and radiomics tools in gastroenteric oncology as they are the most consistent and accurate predictors of tumor response in the case of studies with higher methodological rigor (Table 2).
GRADE assessment of radiomics and AI-based predictive studies in digestive system neoplasms
3.5
The Grading of Recommendations Assessment, Development, and Evaluation (GRADE) framework was used to measure the certainty of evidence throughout the included studies in the context of evaluating radiomics and AI-based tumor response prediction models in digestive system neoplasms. The main points taken into account were study design, risk of bias, inconsistency, indirectness, imprecision, and publication bias.
The majority of the included studies were prospective or multicenter diagnostic or AI-based studies, with a considerable fraction being retrospective radiomics or deep learning analyses. The studies that presented a low risk of bias and were multicenter designs usually achieved high overall certainty that was indicative of strong methodology and wide applicability. The moderate risk of bias was mainly associated with retrospective single-center studies, small pilot trials, or early-stage AI model development, resulting in moderate overall certainty.
Inconsistency and indirectness remain a little bit low across the whole studies which indicate AI/radiomics models performed predictively and were clinically relevant to tumor response consistently. Imprecision was the main characteristic of small sample sizes only or studies that did not have external validation. Publication bias was primarily deemed as unlikely in the majority of multicenter or prospective investigations but as a possibility in single-center or retrospective analyses.
With all these factors taken into consideration, it can be concluded that this GRADE assessment points out that prospective multicenter radiomics and AI studies yield “high-certainty” evidence for prediction of tumor response in digestive system neoplasms while smaller or retrospective studies provide “moderate-certainty” evidence. Our meta-analysis supports these results and highlights the need for methodological rigor, multicenter validation, and comprehensive reporting as critical factors increasing the clinical translation of AI and radiomics models in gastrointestinal oncology (Table 3).
Group and subgroup analysis
3.6
Group 1: endoscopy-based detection and diagnosis
3.6.1
Subgroup 1A: upper GI endoscopy (esophagus and stomach)
3.6.1.1
This subgroup contains eight studies that assessed the real-time AI-assisted detection of upper gastrointestinal cancers during endoscopy. Deep learning and convolutional neural networks (CNNs) based algorithms were the main techniques used by these studies for better lesion identification, photodocumentation improvement, and diagnostic accuracy in both the esophagus and stomach. A meta-analysis applying a random-effects model together with inverse variance weighting disclosed a pooled odds ratio (OR) of 16.12 (95% CI: 7.72–33.65), which was a strong sign of detection performance enhancement with AI support (p < 0.05). Nevertheless, heterogeneity was at a substantial level (I^2^ = 97%, p < 0.01), thus it could be inferred that differences in effect sizes across studies contributed to this difference, possibly because of the variations in sample size, AI model architecture, or endoscopic technique. AI-assisted upper GI endoscopy finds its place in the marked enhancement of cancer detection; however, standardization of validation protocols across different centers is still a must to have uniform performance (Figure 3).
Forest plot of the studies about upper GI endoscopy.
Subgroup 1B: colonoscopy and colorectal polyps
3.6.1.2
The evaluation of colonoscopy and the role of AI-techniques in this area represent the main topic of 19 studies listed under this subgroup. The emphasis of these studies was put on the introduction of real-time AI optical diagnosis, resect-and-discard strategies, and automated lesion assessment to boost polyp detection, characterization, and procedural efficiency. A meta-analysis using a random-effects model with inverse variance weighting exhibited a pooled odds ratio (OR) of 12.0 (95% CI: 10.26–14.03), which signified a statistically significant enhancement in detection performance (p < 0.05). Moderate heterogeneity was found (I^2^ = 75%, p < 0.01), meaning that there could be differences in effect sizes due to variations in AI models, colonoscopy techniques, and study patients. To sum up, the results from the studies clearly show that AI-assisted colonoscopy provides enormous support to the routine endoscopic practice as it not only significantly improves the polyp detection and characterization but also highlights the importance of standardized multicenter validation (Figure 4).
Forest plot of the studies about colonoscopy and colorectal polyps.
Subgroup 1C: capsule endoscopy and small bowel lesions
3.6.1.3
There are a total of eight studies in this subgroup. All of them have been assessing the application of AI in the case of capsule endoscopy for the real-time detection and classification of small bowel lesions. The researches were performed based on deep learning and CNN-based methods, which were typically used for lesion marking, detection, and classification in the small intestine area. By employing the random-effects model together with a meta-analysis and inverse variance weighting, the researchers were able to derive an overall odds ratio (OR) of 10.16 (95% CI: 8.32–12.4), thus demonstrating a statistically significant and trustworthy improvement in the detection of lesions (p < 0.05). A moderate degree of heterogeneity was observed (I^2^ = 50%, p = 0.05) indicating that there is some inconsistency in the effect sizes, probably due to the differences in the AI models, the capsule platforms, and the study subjects. The overall conclusion is that AI-assisted capsule endoscopy provides a great boost to the detection of small bowel lesions. Thus, the significant increase in the quality of the diagnosis made possible by the AI-assisted method will also be likely to bring about the earlier intervention in clinical practice (Figure 5).
Forest plot of the studies about capsule endoscopy and small bowel lesions.
Group 2: AI-assisted surgical and intraoperative guidance
3.6.2
This section covers eight studies that have reported on the use of AI for intraoperative decision-making and surgical guidance with a specific emphasis on the recognition of the grave human body parts, identification of the surgical phase, and discharge of the patients. The AI-assisted models, primarily based on deep learning, were able to provide excellent performance in terms of intraoperative accuracy and decision support in all these studies. A meta-analysis conducted using a random-effects model with inverse variance weighting is giving a pooled odds ratio (OR) of 8.12 (95% CI: 7.12–9.26), indicating that there was a statistically significant increase in the intraoperative outcomes (p < 0.05). There was very little heterogeneity, which means that the different studies had similar sizes of effects across the board in both the magnitude and the direction. Overall, these results strengthen the argument that AI-assisted surgical guidance has the potential to create uniformity in surgical procedures, decrease the number of surgical mistakes, and facilitate the management of patients after surgery (Figure 6).
Forest plot of the studies about AI-assisted surgical and intraoperative guidance.
Group 3: AI for risk stratification and prognosis
3.6.3
The subheading group contains a total of nine studies that constitute the scientific basis for the evaluation of AI-supported risk stratification and prognostic prediction. The methods employed in the selected studies were CT and MRI radiomics, integration of multimodal AI processes, and application of deep learning to histopathology, all for the purpose of predicting lymph node metastasis, molecular subtypes, and overall prognosis. Perform meta-analysis applying random-effects model and inverse variance weighting, which resulted in a pooled odds ratio (OR) of 9.62 (95% CI: 7.93–11.66) reflecting a highly significant predictive ability. However, a moderate heterogeneity was observed, suggesting variability in effect size and direction among studies. (I^2^ = 60%, p = 0.01).In summary, these results demonstrate the capacity of AI-based prognostic models to not only minimize but also guide clinical decision-making in the field of digestive system cancers by providing better risk assessment tailored to the individual patient (Figure 7).
Forest plot of the studies about AI for risk stratification and prognosis.
Group 4: radiomics and deep learning for tumor response/recurrence
3.6.4
Subgroup 4A: rectal and colorectal cancer
3.6.4.1
This specific group includes 23 different studies that were aimed at predicting and studying the tumor response, especially pathological complete response (pCR), and recurrence risk in rectal and colorectal cancer with the help of MRI and CT radiomics using deep learning models. Multiple studies doing meta-analysis under a random-effects model with inverse variance weighting arrived at the conclusion that there is a pooled odds ratio (OR) of 10.48 (95% CI: 9.66–11.36), suggesting that the predictive capability is statistically significant (p < 0.05). Moreover, no significant heterogeneity was revealed, so the effect sizes in the studies were not only consistent but also in the same direction across the studies. Therefore, the use of AI-driven radiomics for assessing tumor response and recurrence risk in rectal and colorectal cancer is really strong and has great clinical potential (Figure 8).
Forest plot of the studies about rectal and colorectal cancer.
Subgroup 4B: gastric, esophagogastric and esophageal cancer
3.6.4.2
The present subgroup consists of a total of 19 research articles that examined the use of CT, MRI, and deep learning-based radiomics models for the purposes of predicting the response to treatment, recurrence and metastasis of lymph nodes in cancers of stomach, esophagus, and esophagogastric junction. These studies were based on the extraction of radiomics features and on the use of deep learning classifiers, which made possible not only the prediction of the tumor response, but also the estimation of the recurrence risk and the prediction of the involvement of lymph nodes. Meta-analysis using a random-effects model with inverse variance weighting further revealed a pooled odds ratio (OR) of 10.81 (95% CI: 9.89–11.82), indicating that the predictive performance was statistically significant (p < 0.05). Importantly, thus far no considerable heterogeneity has been found, which reflects stable and trustworthy effect sizes throughout the studies included in the analysis. This represents a strong argument for AI-powered radiomics providing an effective tool for early prediction of the disease course and for individualized treatment decisions in the case of cancers of the upper GI tract (Figure 9).
Forest plot of the studies about gastric, esophagogastric and esophageal cancer.
Subgroup 4C: molecular and histopathology AI models
3.6.4.3
The diversity of applications of deep learning on histopathological and molecular datasets for predicting microsatellite instability, genetic alterations, and molecular subtypes in cancers, including colorectal, is represented by the twelve studies in this subgroup. The use of pathology-based AI models in these studies was to facilitate molecular characterization and stratification, thus allowing better prognostic assessment and personalized therapy to some extent. The random-effects model with inverse variance weighting employed for meta-analysis resulted in a pooled odds ratio (OR) of 11.62 (95% CI: 10.42–12.95), which was indicative of statistically significant predictive performance (p < 0.05). It is worth mentioning that there was no significant heterogeneity found, which means that the effect sizes were consistent across all the studies included, and this in turn gives strength to the argument of AI-assisted histopathology and molecular profiling being a stronghold in cancer research (Figure 10).
Forest plot of the studies about molecular and histopathology AI models.
Subgroup 4D: CT/MRI radiomics for recurrence and prognosis
3.6.4.4
The subgroup under consideration comprises 13 distinct research works that focus on the fusion of CT and MRI radiomics with deep learning to forecast the reappearance of tumor, postoperative results, and general prognosis in cancers of the gastrointestinal tract. The investigations conducted were primarily based on the application of radiomics-derived nomograms along with deep learning models to classify patients based on the risk of recurrence and to improve the accuracy of postoperative prognosis. In a meta-analysis carried out with a random-effects model combining inverse variance weighting, a pooled odds ratio (OR) of 10.59 (95% CI: 9.52–11.79) was found, which revealed predicting performance that was statistically significant (p < 0.05). No considerable heterogeneity was observed, thus implying that effect sizes were quite similar across various studies, and allowing the conclusion of high AI-assisted CT and MRI radiomics' power and prognosis assessment to be significant and reproducible (Figure 11).
Forest plot of the studies about CT/MRI radiomics for recurrence and prognosis.
Publication bias
3.7
Publication bias was investigated through funnel plots and Egger's test. Group 1, comprising different Endoscopy-Based Detection and Diagnosis techniques, placed Subgroup 1A (Upper GI Endoscopy) as bias-free (intercept: −20.18, 95% CI: −45.6 to 5.23, t = −1.557, p = 0.171), whereas Subgroup 1B (Colonoscopy and Colorectal Polyps) was suspected of incorporating biased studies (intercept: −10.76, 95% CI: −13.98 to −7.54, t = −6.553, p = 0), and Subgroup 1C (Capsule Endoscopy and Small Bowel Lesions) was declared bias-free (intercept: −10.68, 95% CI: −24.48 to 3.11, t = −1.518, p = 0.18). AI-Assisted Surgical and Intraoperative Guidance, there was no indication of bias (intercept: −3.17, 95% CI: −11.46 to 5.12, t = −0.75, p = 0.482). In the same way, AI for Risk Stratification and Prognosis did not exhibit any bias (intercept: −2.49, 95% CI: −11.64 to 6.67, t = −0.533, p = 0.611). Radiomics and Deep Learning for Tumor Response/Recurrence, Rectal and Colorectal Cancer pointed to possible publication bias (intercept: 3.91, 95% CI: 0.77–7.04, t = 2.438, p = 0.024). Gastric, Esophagogastric and Esophageal Cancer (intercept: 2.01, 95% CI: −0.89 to 4.91, t = 1.356, p = 0.193), Molecular and Histopathology AI Models (intercept: −3.27, 95% CI: −7.11 to 0.56, t = −1.672, p = 0.126), and CT/MRI Radiomics for Recurrence and Prognosis (intercept: −0.45, 95% CI: −5.23 to 4.33, t = −0.184, p = 0.857) did not indicate significant publication bias. In conclusion, the majority of the analyses showed a very slight risk of bias, with notable exceptions in the areas of colonoscopy and rectal cancer radiomics, which could be attributed to small-study effects and thus should be interpreted with caution (Figure 12).
Funnel plot of the included studies.
Discussion
4
Summary of main findings
4.1
The present systematic review and meta-analysis comprising 149 studies conducted from 2016 to 2025 offering various AI, deep learning, and radiomics perspectives for the diagnosis of digestive system tumors' detection, characterization, and prognosis as well as the prediction of response to therapy. Endoscopy-Based Detection and Diagnosis found that AI was able to enhance the performance of the endoscopic methods and thus, the lesions' detection in the entire upper and lower gastrointestinal (GI) tract. The studies on upper GI endoscopy exhibited the best diagnostic performance (OR = 16.12, 95% CI: 7.72–33.65), followed by colonoscopic evaluation of colorectal polyps (OR = 12.0, 95% CI: 10.26–14.03) and capsule endoscopic assessment of small bowel lesions (OR = 10.16, 95% CI: 8.32–12.4). The variation of results was quite large (I^2^ = 97%) in upper GI and quite large (I^2^ = 75%) in colonoscopy studies while it was moderate (I^2^ = 50%) in capsule endoscopy. Out of the three methods, publication bias was observed only in the colonoscopy studies (Egger's intercept: −10.76, p = 0); however, upper GI and capsule endoscopy studies exhibited no significant bias thus confirming the trustworthiness of AI in early detection and characterization.
AI-Assisted Surgical and Intraoperative Guidance (OR = 8.12, 95% CI: 7.12–9.26) emphasized AI's contribution to the real-time detection of crucial anatomical structures, the recognition of surgical phases, and the optimization of postoperative discharge. The size of the effect was consistent across studies, the heterogeneity was minimal, and no bias in publication was detected (Egger's intercept: −3.17, p = 0.482), which together indicated the reproducible effectiveness of AI in improving surgical outcomes, and thus indirectly supported accurate tumor response assessment through optimized operative management.
AI for Risk Stratification and Prognosis (OR = 9.62, 95% CI: 7.93–11.66) validated the prediction of AI-based models using CT/MRI radiomics, histopathology, and multimodal deep learning for lymph node metastasis, molecular subtypes, and survival outcomes. The heterogeneity was moderate (I^2^ = 60%), while no publication bias was identified (Egger's intercept: −2.49, p = 0.611), thus affirming the reliability of AI-influenced prognostic stratification.
Radiomics and Deep Learning for Tumor Response and Recurrence was the one that showcased the most concrete proof for AI-based prediction of the tumor response. Subgroup 4A (Rectal and Colorectal Cancer) reported OR = 10.48 (95% CI: 9.66–11.36) alongside possible publication bias (Egger's intercept: 3.91, p = 0.024). Subgroup 4B (Gastric, Esophagogastric and Esophageal Cancer) gave OR = 10.81 (95% CI: 9.89–11.82) with no bias. Subgroup 4C (Molecular and Histopathology AI Models) was the highest with OR = 11.62 (95% CI: 10.42–12.95), while Subgroup 4D (CT/MRI Radiomics for Recurrence and Prognosis) indicated OR = 10.59 (95% CI: 9.52–11.79), both free from substantial publication bias, and hence demonstrated the same predicting ability for tumor shrinkage, complete response, relapse, and postoperative prognosis.
According to the Radiomics Quality Score (RQS) assessment of the included studies the quality of the image acquisition and processing was often very high and the reproducibility of the radiomic features was ensured. Feature selection and their robustness were motives to improve overfitting and generalizability to the end-users. The validation strategies used by the studies differed a lot, and the studies that compared the external and multicenter datasets were given higher RQS, additional merits being indicated by the predictive reliability. There was a lack of biological or clinical validation in most of the studies, thus radiomic and AI predictions not always linked to clinical outcomes, which is identified as an area for improvement in future research. Total RQS scores were within the range of 10–21 and most of the research works got moderate to high quality (14–19) thus it was supported that the studies with higher methodological rigor reported more consistent and accurate tumor response predictions.
Based on the PROBAST criteria, approximately 120 AI and radiomics studies were evaluated in patients with gastrointestinal, colorectal, esophageal, gastric, and biliary cancers, and the overall risk of bias was assessed to be low to moderate. The selection of participants and defining the outcomes were mostly very strong, while some limitations were detected in predictor selection and analysis due to variability in feature selection, algorithm transparency, sample size, and validation strategies. Among the analytical concerns were overfitting, incomplete internal vs. external validation, and inconsistent data handling which pointed out the necessity of standardized reporting, transparent modeling, and significant external validation in order to improve clinical relevance.
Diagnostic models use imaging assessments to achieve their primary goal which involves identifying lesions and characterizing tumors and distinguishing between benign and malignant conditions. Predictive models forecast treatment response outcomes which help doctors choose personalized treatment options while they decrease patient exposure to ineffective treatments in neoadjuvant settings. Prognostic models, in contrast, estimate long-term outcomes such as recurrence risk and survival, enabling improved risk stratification and follow-up planning. The three distinct clinical functions of each category show their unique purposes yet their common traits demonstrate how radiomics features can be used in various ways. The process of defining these operational functions leads to better understanding which demonstrates how AI technology has developed to support cancer treatment throughout its entire process.
The GRADE evaluation and meta-analysis results suggest that AI and radiomics techniques are very convincing in the case of tumor detection, risk grading, prognosis and prediction of treatment response in tumors of the digestive system. Generally speaking, these technologies are showing reliable, clinically important, and non-intrusive predictive abilities, which are facilitating the use of precision oncology approaches and personalized treatment of gastrointestinal cancer patients through the guidance of decision-making based on the patient's characteristics.
The combined research results produced higher odds ratios which remained constant through multiple studies that utilized radiomics-based AI systems. The advanced imaging analytics demonstrate strong predictive capabilities yet their results need careful assessment. The majority of studies used retrospective methods together with case-control designs and they built their study groups using disease profiles which exceeded normal real-world patterns. The research methods used in this study create spectrum bias which results in exaggerated model performance assessment. The reported effect sizes should function as indicators of potential clinical effectiveness which need further testing to achieve complete validation. The true clinical utility of these technologies needs assessment through research studies which will use actual patient populations and standardized imaging protocols and independent validation groups.
Comparison with previous studies
4.2
Comparison with Previous Studies The developments in imaging, artificial intelligence (AI), and radiomics in gastrointestinal oncology have been gradually recognizing each other as important partners in the areas of diagnosis, surgical planning, and prognostication. However, the majority of studies still restricted themselves to limited scope, small sample size, or tumor type specificity. Other systematic reviews like Bhardwaj et al. (21), Vadhwana et al. (22), Tasci et al. (23), and Park et al. (24) have also assessed AI for specific tasks such as predicting gastric cancer, differentiating colorectal lesions histology, and others in the area of gastrointestinal surgery and microsatellite instability. However, studies conducted in these areas were often not connected through comprehensive meta-analysis integrating across the different cancers of the digestive system. On the contrary, the present systematic review together with the meta-analysis, combined results from a total of 120 studies that included upper and lower gastrointestinal, liver, pancreatic, and small bowel tumors, which resulted in the generation of pooled effect estimates for the prediction of tumor response using AI and radiomics. Our study, by applying publication bias assessment, GRADE evaluation, PROBAST risk-of-bias assessment, and Radiomics Quality Score (RQS) analysis, provides a more rigorous, quantitative, and clinically applicable appraisal than previous narrative or single-system reviews have done. Moreover, the merging of the three approaches, that is, intraoperative AI guidance, radiomics-based prognostic modeling, and histopathology/molecular AI prediction, all in one framework, is what sets this current study apart from the previous ones, as it not only demonstrates methodological rigor but also shows the ability to translate the findings to clinical practice in the area of digestive system oncology. This methodology not only verifies the prediction capabilities of artificial intelligence and radiomics but also uncovers the drawbacks in methods, the necessity for standardization, and the need for external validation in research, thus upgrading the previous studies not only to clinical but also research and guidance for the future.
Radiomics and AI-based diagnostic systems use their predictive capabilities to identify potential health issues in digestive system cancers. The medical field needs to overcome various challenges before these systems can be used in standard operational procedures. Model interpretability stays as an urgent problem because machine learning and deep learning methods function as black box systems which restricts clinician confidence in their implementation. Explainable AI methods help create better system transparency by showing which imaging elements impact prediction results. The system needs to establish its functional requirements because it needs to demonstrate its essential functions and operations through its software interface and data processing techniques. AI systems must fulfill new regulatory standards which require systems to provide reproducible results and standardized data presentation methods and to protect sensitive information and to validate all system requirements through future testing. Medical facilities need to establish their systems to work with current radiology operating procedures and electronic health record systems and imaging equipment. Algorithmic bias continues to present organizations with a persistent problem. The development of models using retrospective datasets or highly controlled datasets creates a potential risk of introducing selection bias and demographic representation issues and institutional imaging practices into the resulting model. The factors which decrease generalizability will lead to performance decline because the algorithms must operate under actual work conditions. The establishment of reliable and fair AI-based healthcare systems needs to resolve these problems through the use of various training datasets and the implementation of open reporting frameworks and the use of future assessment methods.
Strengths and limitations
4.3
Strengths
4.3.1
This research carries out a thorough synthesis of 149 studies on AI and radiomics in the case of neoplasms of the digestive system providing a quantitative evaluation. Among others, it evaluates the methodological quality (RQS), the risk of bias (PROBAST), and the existence of publication bias (Egger's test). The results indicate that the predicted outcomes were accurate and clinically relevant as the studies involved high-risk patients.
Limitations
4.3.2
The heterogeneity in study design, sample size, cancer types and AI algorithms may limit the generalizability. The external validation and the prospective multicenter data were limited. Some papers did not define their outcomes in a standardized manner or did not use blinded assessment. The publication bias was present in the studies of colonoscopy and rectal/colorectal radiomics, which may have led to the inflating of estimates of effect. AI systems that researchers develop for specific geographical regions become less accurate when testers use these systems to assess their performance on different demographic groups. Future research should establish multiple research centers to conduct studies on various populations which will lead to better system performance and wider use in medical practices.
Conclusion
5
The radiomics and AI-based models have been shown to be a reliable and precise method through this systematic review and meta-analysis for predicting tumor response, recurrence, and prognosis in digestive system neoplasms. AI-assisted detection, intraoperative guidance, risk stratification, and radiomics approaches have been found to enhance diagnostic and prognostic performance consistently throughout the 120 studies. The quality of the methodological assessment based on RQS and PROBAST criteria was found to be moderate-to-high, however, the need for external validation, multicenter studies, and biological or clinical correlation was pointed out. The bias in publication was reported to be minor in most groups but present in some subgroups, indicating the necessity for clear reporting. The results, overall, advocate for the fusion of AI and radiomics into the workflows of gastrointestinal oncology, while at the same time, they stress the need for standardized protocols, rigorous validation, and prospective studies to make the clinical applicability and reliability easier and better.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Munir MM Endo Y Ejaz A Dillhoff M Cloyd JM Pawlik TM. Online artificial intelligence platforms and their applicability to gastrointestinal surgical operations. J Gastrointest Surg. (2024) 28:64–9. doi: 10.1016/j.gassur.2023.11.01938353076 · doi ↗ · pubmed ↗
- 2Jazi AHD Mahjoubi M Shahabi S Alqahtani AR Haddad A Pazouki A . Bariatric evaluation through AI: a survey of expert opinions versus Chat GPT-4 (BETA-SEOV). Obes Surg. (2023) 33:3971–80. doi: 10.1007/s 11695-023-06903-w 37889368 · doi ↗ · pubmed ↗
- 3Ahmad OF Mori Y Misawa M Kudo SE Anderson JT Bernal J . Establishing key research questions for the implementation of artificial intelligence in colonoscopy: a modified Delphi method. Endoscopy. (2021) 53:893–901. doi: 10.1055/a-1306-759033167043 PMC 8390295 · doi ↗ · pubmed ↗
- 4Lazaridis LD Tziatzios G Toth E Beaumont H Dray X Eliakim R . Implementation of European society of gastrointestinal endoscopy (ESGE) recommendations for small-bowel capsule endoscopy into clinical practice: results of an official ESGE survey. Endoscopy. (2021) 53:970–80. doi: 10.1055/a-1541-293834320664 · doi ↗ · pubmed ↗
- 5Garfinkle R Petersen RP Du Coin C Altieri MS Aggarwal R Pryor A . Consensus priority research questions in gastrointestinal and endoscopic surgery in the year 2020: results of a SAGES Delphi study. Surg Endosc. (2022) 36:6688–95. doi: 10.1007/s 00464-021-08941-w 35028734 · doi ↗ · pubmed ↗
- 6Huo B Marfo N Sylla P Calabrese E Kumar S Slater BJ . Clinical artificial intelligence: teaching a large language model to generate recommendations that align with guidelines for the surgical management of GERD. Surg Endosc. (2024) 38:5668–77. doi: 10.1007/s 00464-024-11155-539134725 · doi ↗ · pubmed ↗
- 7Nasir I Mureb A Aliozo CC Abunada MH Parvaiz A. State of the art in robotic rectal surgery: marginal gains worth the pain? Updates Surg. (2021) 73:1073–9. doi: 10.1007/s 13304-020-00965-633675509 · doi ↗ · pubmed ↗
- 8Davnall F Yip CS Ljungqvist G Selmi M Ng F Sanghera B . Assessment of tumor heterogeneity: an emerging imaging tool for clinical practice? Insights Imaging. (2012) 3:573–89. doi: 10.1007/s 13244-012-0196-623093486 PMC 3505569 · doi ↗ · pubmed ↗