Malignant Hypertension and Torsades De Pointes as Initial Presentations of Primary Aldosteronism
Yanqiu Li

TL;DR
A 31-year-old woman with severe hypertension and low potassium was later diagnosed with primary aldosterionism after a delayed diagnosis and life-threatening arrhythmia.
Contribution
The paper highlights how common medications can interfere with PA diagnosis and emphasizes the importance of adrenal imaging and venous sampling.
Findings
Common antihypertensive drugs can mask primary aldosteronism by affecting aldosterone-to-renin ratio testing.
Adrenal venous sampling is critical for accurate diagnosis and surgical planning in PA.
Primary aldosteronism can lead to life-threatening arrhythmias due to severe hypokalemia.
Abstract
Primary aldosteronism (PA) is a common yet underdiagnosed cause of secondary hypertension, particularly in young patients presenting with severe disease. A 31-year-old woman presented with malignant hypertension (264/144 mm Hg), severe hypokalemia (K+ level 2.60 mmol/L), and acute pulmonary edema. Her initial work-up during nicardipine and furosemide infusion showed a normal aldosterone-to-renin ratio (ARR), leading to misdiagnosis as essential hypertension. Over a 3-year follow-up, she developed refractory hypertension during pregnancy and preeclampsia. She was readmitted with torsades de pointes triggered by severe hypokalemia (K+ level 1.90 mmol/L). Repeat testing revealed a markedly elevated ARR (667.26). Adrenal venous sampling confirmed right-sided PA. Right adrenalectomy confirmed a cortical adenoma, with subsequent normalization of blood pressure and potassium levels. This…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1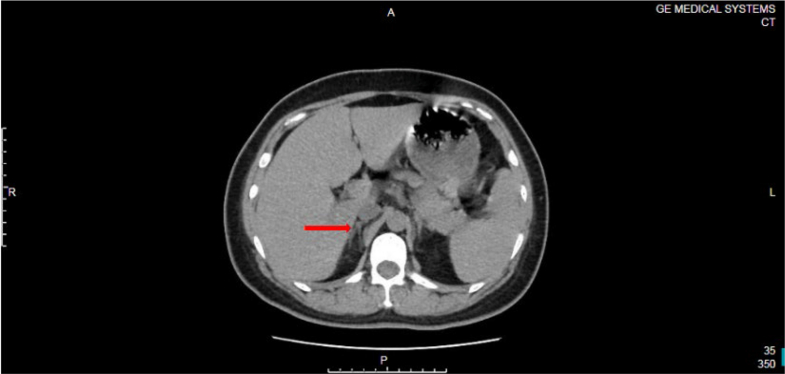 Figure 2
Figure 2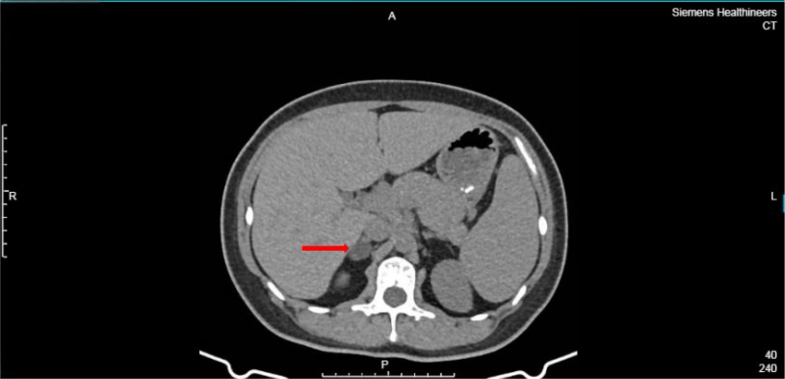 Figure 3
Figure 3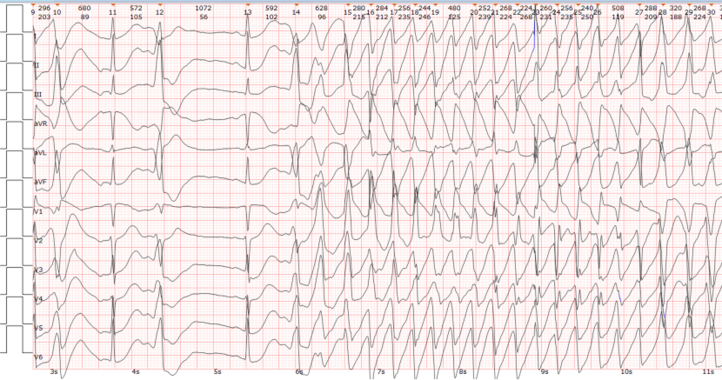 Figure 4
Figure 4 Figure 5
Figure 5Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHormonal Regulation and Hypertension · Adrenal and Paraganglionic Tumors · Renin-Angiotensin System Studies
History of Presentation
A 31-year-old woman presented to the emergency department with progressive cough and dyspnea. One month earlier, she was found to have elevated blood pressure (up to 220/140 mm Hg) but received no treatment. Physical examination revealed tachycardia (heart rate 159 beats/min), tachypnea (respiratory rate 38 breaths/min), a blood pressure of 264/144 mm Hg, and an oxygen saturation of 86%.Visual SummaryCase Timeline: Diagnostic and Therapeutic JourneyARR = aldosterone-to-renin ratio; AVS = adrenal venous sampling; CT = computed tomography; TdP = torsades de pointes.
Past Medical History
The patient had no significant past medical history and no family history of hypertension.
Differential Diagnosis
Initial differential diagnoses included essential hypertension with hypertensive emergency, primary aldosteronism (PA), other secondary causes of hypertension (renal artery stenosis and pheochromocytoma), and acute myocarditis.
Investigations
Arterial blood gas analysis revealed metabolic acidosis with severe hypokalemia (K^+^ level 2.60 mmol/L). Chest radiography confirmed pulmonary edema. The N-terminal pro–B-type natriuretic peptide level was elevated to 1,333.58 pg/mL. The initial etiological work-up for hypertension, conducted during intravenous infusion of nicardipine and furosemide, showed that the aldosterone level was 240.40 pg/mL and the renin level 15.03 pg/mL (aldosterone-to-renin ratio [ARR] 15.99). Adrenal ultrasonography showed no abnormalities. A chest computed tomography (CT) scan incidentally captured portions of the adrenal glands but identified no definite nodules (Figure 1). The secretion rhythms of catecholamines and aldosterone were normal.Figure 1. Noncontrast Chest Computed Tomography Scan From October 29, 2021, Incidentally Capturing the Adrenal Region (Arrows), Showing no Definite Nodule
During pregnancy (in 2023), persistent hypokalemia (K^+^ level 2.66 mmol/L) was documented. Postpartum CT identified a 19 × 14 mm right adrenal nodule (Figure 2).Figure 2. Contrast-Enhanced Adrenal Computed Tomography Scan From January 15, 2024, Revealing an Approximately 19 × 14 mm Nodule in the Right Adrenal Gland (Arrow)
At readmission (in 2024), severe hypokalemia (K^+^ level 1.90 mmol/L) and multiple episodes of torsades de pointes (TdP) were documented (Figure 3). Repeat hypertensive evaluation demonstrated that the aldosterone level was 2,227.87 pg/mL and the renin level 0.34 pg/mL (ARR 667.26). Adrenal venous sampling (AVS) confirmed right-sided lateralization.Figure 3. Rhythm Strip Recorded During Severe Hypokalemia (K^+^ Level 1.90 mmol/L), Showing an Episode of Torsades de Pointes
Management
Initial management included cardiopulmonary resuscitation, endotracheal intubation, and intensive care unit admission for acute heart failure. After the initial admission, the patient was discharged on multiple antihypertensive agents and potassium supplements.
During pregnancy, she received nifedipine, labetalol, and methyldopa but blood pressure control remained inadequate, necessitating cesarean delivery at 32^+1^ weeks for preeclampsia.
Definitive management involved right adrenalectomy after confirmation of right-sided PA by AVS.
Outcome and Follow-Up
Postoperatively, the patient's blood pressure control improved significantly, requiring only 2 oral antihypertensive agents. Potassium levels normalized without supplementation. No further arrhythmic events occurred during follow-up.
Discussion
This case provides 3 inter-related core insights for cardiovascular practice.
The pitfall of pharmacological interference in ARR diagnosis
This case is a classic example of medication interference in biochemical testing. The initial false negative ARR was a direct pharmacological consequence of nicardipine administration. Dihydropyridine calcium-channel blockers potently stimulate renin release via mechanisms including renal arteriolar vasodilation.1 In this patient, nicardipine artificially elevated renin from the suppressed levels typical of PA into the normal range whereas aldosterone remained inappropriately high for the context of hypertension with hypokalemia, mathematically depressing the ARR and creating a diagnostic blind spot.
It is critical to recognize that calcium-channel blockers are not the only antihypertensive agents that confound the ARR. Thiazide diuretic agents stimulate renin secretion via volume contraction and can induce hypokalemia, which itself suppresses aldosterone secretion.2 This combination of “elevated renin and suppressed aldosterone” severely distorts the ARR. Therefore, a comprehensive medication review is imperative before ARR testing.
The dynamic nature of PA and insights from imaging evaluation
Imaging follow-up in this case offers a unique perspective on the natural history of adrenal nodular lesions. Initial adrenal ultrasound and limited chest CT at first presentation showed no definite nodules, whereas a CT scan 3 years later clearly revealed a right adrenal nodule (19 × 14 mm). This dynamic evolution “from absence to presence” strongly suggests that this aldosterone-secreting adenoma likely developed and grew over time.
This reveals that PA is not always a static condition and that functional adenomas have the potential to progress.3 This finding explains why early imaging may have negative results and underscores the necessity of repeat targeted adrenal imaging (eg, dedicated thin-section adrenal CT) during follow-up for patients with high clinical suspicion of PA despite initially negative imaging results. Although ultrasonography is convenient, its detection rate is highly operator dependent and influenced by patient body habitus, whereas CT offers higher spatial resolution and objectivity and is the imaging modality of choice for morphological assessment per guidelines.4
The pathophysiological cascade from aldosterone excess to TdP
This case perfectly illustrates the mechanistic pathway from autonomous aldosterone overproduction to life-threatening ventricular arrhythmia. Aldosterone acts on mineralocorticoid receptors in principal cells of the distal nephron, up-regulating epithelial sodium channels and basolateral sodium-potassium adenosine triphosphatase, promoting potassium excretion and leading to hypokalemia.
Severe hypokalemia alters cardiac potassium channel function, notably causing voltage-dependent inactivation of the rapidly activating delayed rectifier potassium current. Inhibition of this major repolarizing current disrupts the balance between depolarizing and repolarizing forces during the action potential, leading to QT interval prolongation on the surface electrocardiogram. Furthermore, hypokalemia does not uniformly affect all myocardial layers; it preferentially prolongs the action potential duration of mid-myocardial M cells, thereby increasing transmural dispersion of repolarization, creating a vulnerable substrate within the ventricular myocardium. The prolonged repolarization phase also facilitates the occurrence of early afterdepolarizations. When an early afterdepolarization falls within the heterogeneous window of repolarization created by increased transmural dispersion of repolarization, it can precipitate TdP.5^,^6 Therefore, any unexplained QT interval prolongation or TdP should prompt an immediate search for reversible secondary causes, including PA.
The imperative of adrenal venous sampling
Anatomical presence does not invariably correlate with hormonal hypersecretion.7 Guidelines recommend AVS for patients with confirmed PA who are surgical candidates. This case reinforces its necessity. Despite the clear identification of an adrenal nodule on CT, AVS was crucial for confirming it as the functional source. This is critical because if the nodule had been a nonfunctioning incidentaloma, a potentially noncurative surgery could have been avoided. AVS remains indispensable for confirming the functional source and guiding surgical lateralization, which is consistent with current guidelines.8
Conclusions
This case demonstrates that PA can present with malignant hypertension and fatal arrhythmias. It underscores the critical importance of vigilance for medication interference when interpreting the ARR, reveals the dynamic, progressive nature of PA as a disease entity, and delineates the complete, reversible pathophysiological pathway from hormonal excess to end-organ damage.
Patient Consent
Informed consent for publication was obtained from the patient's family.Take-Home Messages
- •Diagnostic vigilance: Primary aldosteronism should be highly suspected in young patients with severe or refractory hypertension and hypokalemia, even if the initial aldosterone-to-renin ratio appears “normal” because of interference from calcium-channel blockers or diuretic agents.
- •Dynamic management perspective: Primary aldosteronism is a progressive disease, and associated adrenal nodules may evolve over time. Repeat targeted adrenal imaging during follow-up should be considered for cases with persistent clinical suspicion despite initially negative imaging results.
Funding Support and Author Disclosures
This work was supported by the Internal Research Fund of The Third Affiliated Hospital of Chongqing Medical University (grant number KY24044). The authors have reported that they have no relationships relevant to the contents of this paper to disclose.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Mulatero P.Rabbia F.Milan A.Drug effects on aldosterone/plasma renin activity ratio in primary aldosteronism Hypertension 40620028979021246857610.1161/01.hyp.0000038478.59760.41 · doi ↗ · pubmed ↗
- 2Williams B.Mancia G.Spiering W.2018 ESC/ESH Guidelines for the management of arterial hypertension Eur Heart J 39332018302131043016551610.1093/eurheartj/ehy 339 · doi ↗ · pubmed ↗
- 3Vaidya A.Carey R.M.The evolution of the primary aldosteronism syndrome: updating the approach J Clin Endocrinol Metab 105122020377137833286520110.1210/clinem/dgaa 606PMC 7899564 · doi ↗ · pubmed ↗
- 4Fassnacht M.Tsagarakis S.Terzolo M.European Society of Endocrinology clinical practice guidelines on the management of adrenal incidentalomas Eur J Endocrinol 18912023 G 1G 423731823910.1093/ejendo/lvad 066 · doi ↗ · pubmed ↗
- 5Drew B.J.Ackerman M.J.Funk M.Prevention of torsade de pointes in hospital settings Circulation 12182010104710602014245410.1161/CIRCULATIONAHA.109.192704 PMC 3056123 · doi ↗ · pubmed ↗
- 6Viskin S.Long QT syndromes and torsade de pointes Lancet 35491901999162516331056069010.1016/S 0140-6736(99)02107-8 · doi ↗ · pubmed ↗
- 7Rossi G.P.Auchus R.J.Brown M.An expert consensus statement on use of adrenal vein sampling for the subtyping of primary aldosteronism Hypertension 63120141511602421843610.1161/HYPERTENSIONAHA.113.02097 · doi ↗ · pubmed ↗
- 8Funder J.W.Carey R.M.Mantero F.The management of primary aldosteronism: case detection, diagnosis, and treatment: an Endocrine Society Clinical Practice Guideline J Clin Endocrinol Metab 10152016188919162693439310.1210/jc.2015-4061 · doi ↗ · pubmed ↗