Pulsed-Field Ablation With Transcatheter Left Atrial Appendage Occlusion for Left Atrial Appendage–Origin Atrial Tachycardia
Junya Komatsu, Hiroki Sugane, Yuki Nishimura, Nao Okamoto, Hayato Hosoda, Yoko Nakaoka, Shinji Mito, Shuichi Seki, Kazuya Kawai

TL;DR
Combining pulsed-field ablation with left atrial appendage occlusion is a feasible treatment for a specific type of heart rhythm disorder.
Contribution
The study demonstrates the feasibility of combining PFA with LAAO for LAA-origin atrial tachycardia.
Findings
PFA can cause significant edema in the left atrial appendage.
Device overcompression based on pre-PFA imaging ensures durable LAA sealing.
Concomitant PFA and LAAO is a viable treatment strategy for LAA-origin AT.
Abstract
Pulsed-field ablation (PFA) may be an emerging treatment for left atrial appendage (LAA)–origin atrial tachycardia (AT), but it may cause thrombus in the LAA. Concomitant transcatheter LAA occlusion (LAAO) may address this risk. A 54-year-old man with symptomatic LAA-origin AT underwent PFA. Post-PFA transesophageal echocardiography showed significant pectinate muscle edema with narrowing of the LAA orifice. To avoid late peridevice leak, a 40-mm Watchman FLX Pro (Boston Scientific) was implanted with intentional overcompression. At the 1-month follow-up, cardiac computed tomography demonstrated a complete LAA seal with adequate device compression. Concomitant PFA and LAAO is feasible for LAA-origin AT. Because PFA can induce significant edema within the LAA, device selection based on pre-PFA imaging is critical to ensure durable sealing. Careful pre-PFA imaging-based device sizing…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1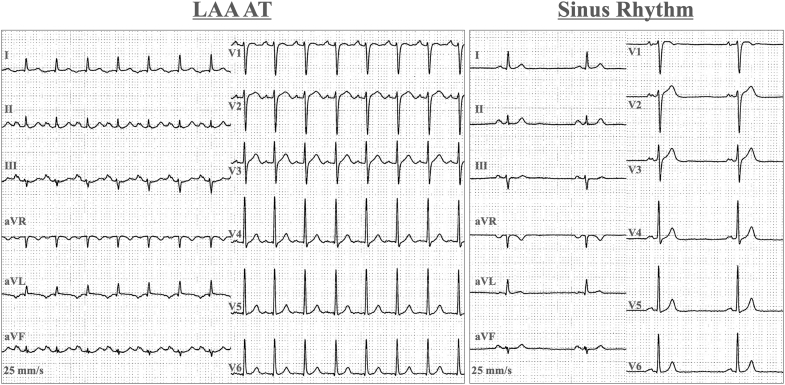 Figure 2
Figure 2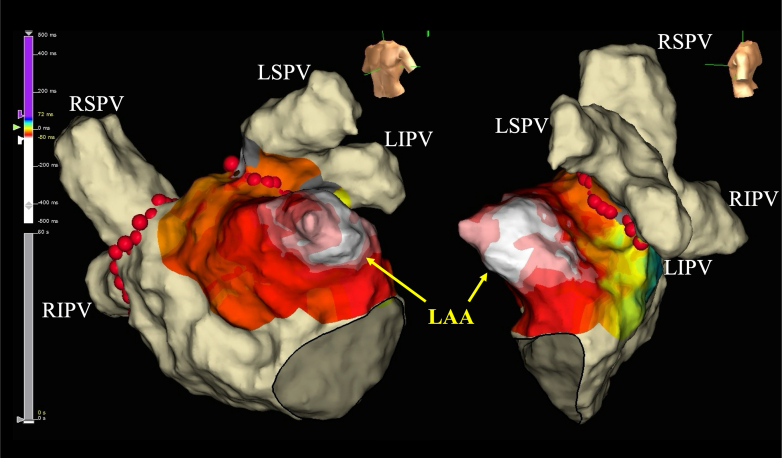 Figure 3
Figure 3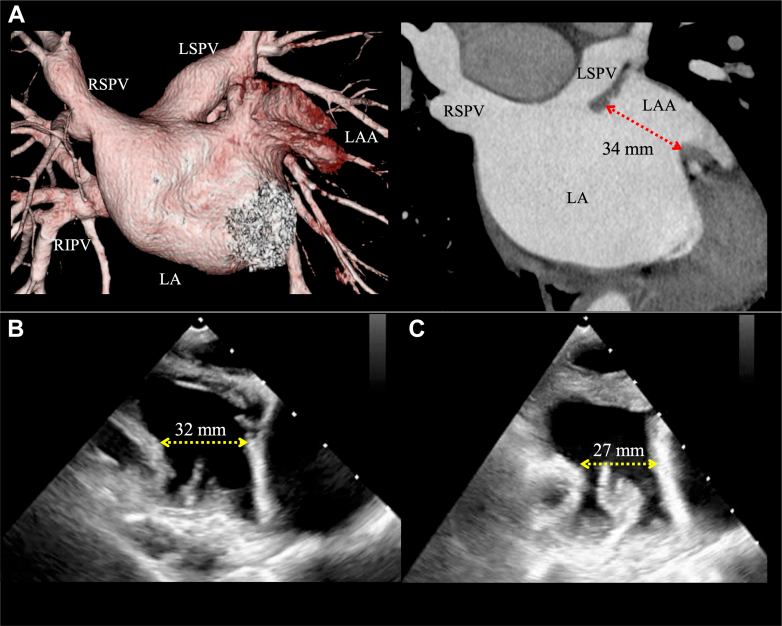 Figure 4
Figure 4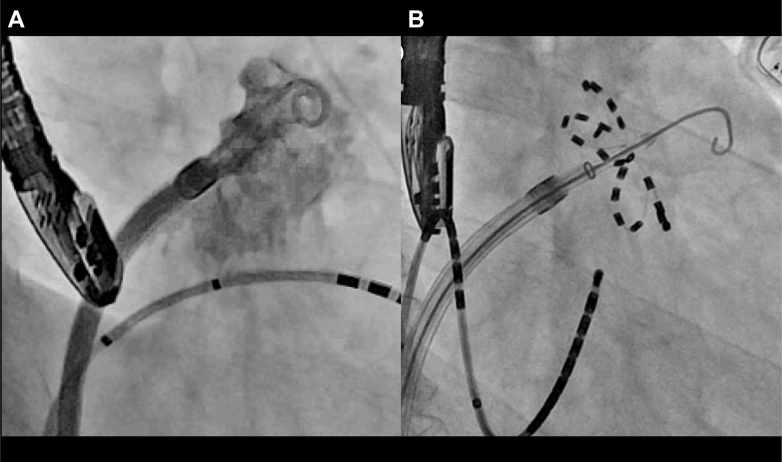 Figure 5
Figure 5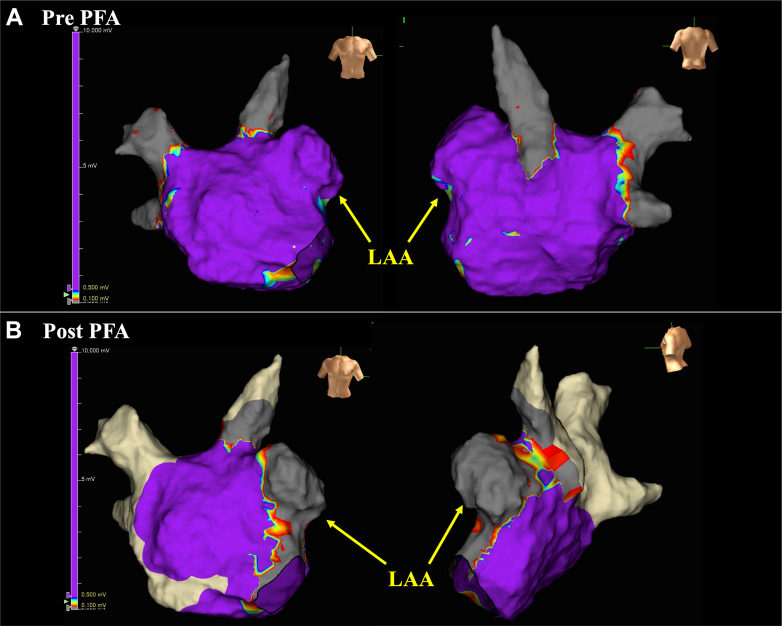 Figure 6
Figure 6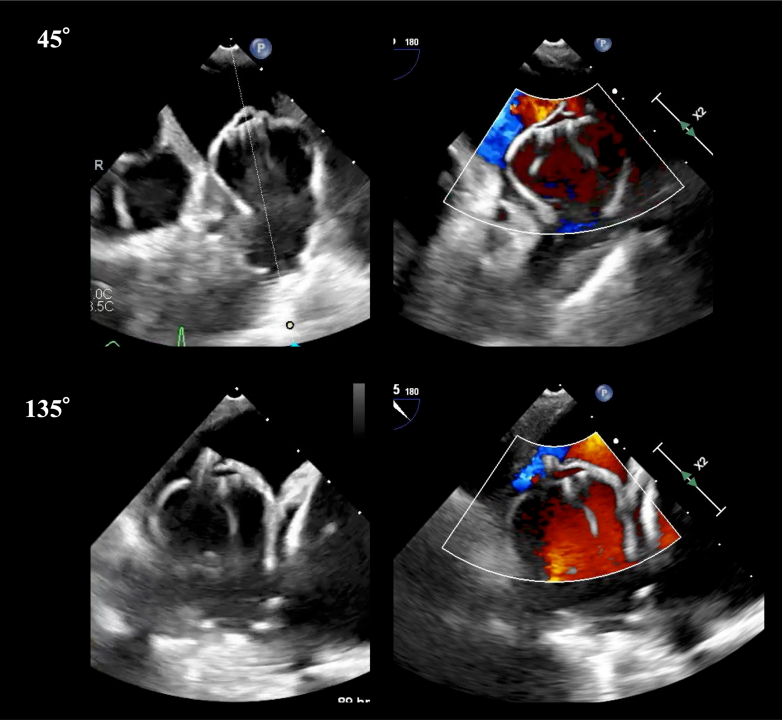 Figure 7
Figure 7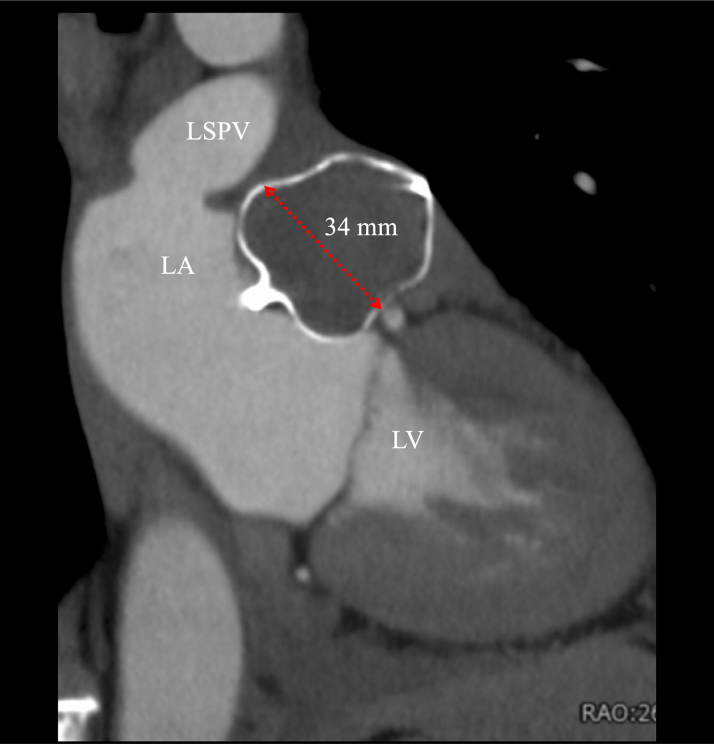 Figure 8
Figure 8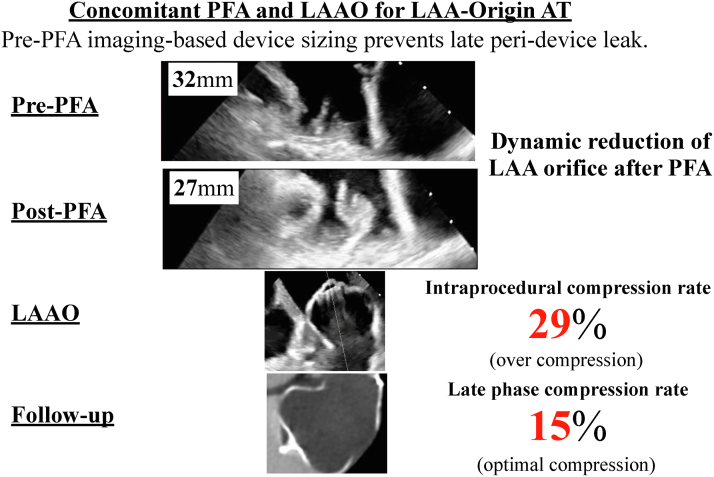 Figure 9
Figure 9Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCardiac Arrhythmias and Treatments · Atrial Fibrillation Management and Outcomes · Cardiac tumors and thrombi
Visual SummaryConcomitant PFA and Transcatheter LAAO for LAA-Origin ATAs PFA can induce acute postablation LAA edema, device sizing based on preablation imaging is critical. AT = atrial tachycardia; LAA = left atrial appendage; LAAO = left atrial appendage occlusion; PFA = pulsed-field ablation.
History of Presentation
A 54-year-old man presented to the outpatient office of our hospital with recurrent palpitations. On examination, his blood pressure was 120/80 mm Hg, his heart rate was 80 beats/min and regular, and there were no signs of heart failure. The arrhythmia terminated spontaneously, but he sought repeat catheter ablation to control symptoms.
Past Medical History
Six months earlier, the patient had undergone standard radiofrequency catheter ablation (RFCA) for paroxysmal atrial fibrillation and the left atrial appendage (LAA)–origin atrial tachycardia (AT) arising from the distal part of the LAA.
Investigations
A 12-lead electrocardiogram showed a positive P-wave deflection in lead V_1_, bifid (notched) P waves in leads II and V_1_, and an inverted P wave in lead I. These findings were suggestive of AT originating from either the left pulmonary vein or the LAA (Figure 1). Transthoracic echocardiography showed normal left ventricular systolic function without valvular or structural abnormalities. Laboratory tests, including thyroid function and cardiac biomarkers, were within normal limits. Ambulatory electrocardiogram monitoring documented frequent episodes of AT. At the initial ablation, invasive electrophysiology study with three-dimensional mapping at the first session showed complete electrical isolation of the pulmonary veins but incomplete suppression of the LAA-origin AT from the distal part of the LAA (Figure 2). Cardiac computed tomography (CT) demonstrated a cactus-shaped LAA with a maximum diameter of 34 mm without thrombus (Figure 3A).Figure 1. Index 12-Lead ElectrocardiogramsElectrocardiograms documenting LAA-origin AT and sinus rhythm for comparison. AT = atrial tachycardia; LAA = left atrial appendage.Figure 23-Dimensional Activation Mapping at the First SessionActivation mapping identifying the earliest atrial activation within the LAA with centrifugal spread to the left atrium. LAA = left atrial appendage; LIPV = left inferior pulmonary vein; LSPV = left superior pulmonary vein; RIPV = right inferior pulmonary vein; RSPV = right superior pulmonary vein.Figure 3LAA Orifice Diameter Findings: Comparison Before and After PFA(A) Preprocedural cardiac CT demonstrating a cactus-shaped LAA with a maximum diameter of 34 mm. Intraprocedural TEE at a 135° angle view (B) before and (C) after PFA showed acute edema of the pectinate muscle with ostial narrowing and contour change caused by PFA, reducing the maximal diameter from 32 mm (B) to 27 mm (C). CT = computed tomography; PFA = pulsed-field ablation; TEE = transesophageal echocardiography; other abbreviations as in Figure 2.
Differential Diagnosis
Alternative mechanisms of AT were considered, including focal AT from other atrial regions and atypical atrial flutter. However, the clinical history and the findings of a prior electrophysiology study with three-dimensional mapping strongly implicated recurrent LAA-origin AT.
Management
Surgical LAA removal was discussed but was declined in favor of catheter-based treatment. Given the prior unsuccessful RFCA, concomitant pulsed-field ablation (PFA) and transcatheter LAA occlusion (LAAO) were planned. The procedure was performed under general anesthesia with transesophageal echocardiography (TEE) guidance. The pre-PFA TEE and the LAA angiography showed a large cactus-shaped LAA with a maximum orifice diameter of 32 mm and no thrombus (Videos 1 and 2). In accordance with this TEE imaging, a 40-mm Watchman FLX Pro (Boston Scientific) was considered appropriate for LAAO.
First, we tried to induce AT, but it was not induced before the procedure. Based on the clinical course, we believed the clinical AT was highly likely to originate from the LAA; we then achieved electrical LAA isolation using the Farapulse PFA system (Boston Scientific). After atrial transseptal puncture, a 12-F Farawave multielectrode pentaspline catheter (Boston Scientific) was advanced into the LAA. Multiple applications (2.5 seconds and 2 kV each) were delivered in the basket and flower configurations (Figure 4), resulting in successful electrical LAA isolation, as evidenced by local dissociation (Figure 5).Figure 4. Findings on LAA Angiography(A) LAA angiography in the right anterior oblique 30° and caudal 30° views. (B) Fluoroscopic image during PFA at the same projection. LAA = left atrial appendage.Figure 5. Left Atrial Voltage Mapping Before and After PFA(A) Pre-PFA left atrial voltage map showing preserved potentials across the LAA-ostial region. (B) Post-PFA voltage map demonstrating abolition of LAA potentials; entrance and exit block were confirmed by pacing maneuvers and lack of capture from within the LAA. LAA = left atrial appendage; PFA = pulsed-field ablation.
Subsequently, the Farapulse system was exchanged for a 15-F Watchman FXD Curve Access system (Boston Scientific) to perform LAAO. However, the post-PFA TEE revealed significant edema of the pectinate muscle, narrowing the LAA orifice from 32 to 27 mm (Figures 3B and 3C, Video 3). Downsizing of the occlusion device from 40 to 35 mm was considered, but this raised concern for late peridevice leak after the improvement of edema. Despite the swollen pectinate muscle occupying part of the LAA, deployment of a 40-mm device from the distal anterior lobe remained feasible (Figure 6). Therefore, a 40-mm Watchman FLX Pro was carefully deployed with intentional overcompression (compression rate: 29%), achieving stable positioning without complications (Videos 4 and 5).Figure 6. Intraprocedural TEE Findings During LAAOA 40-mm device was deployed according to the preablation plan with intentional overcompression (29%), yielding stable seating and no peridevice leak on color Doppler. LAAO = left atrial appendage occlusion; TEE = transesophageal echocardiography.
Outcome and Follow-Up
The patient's recovery was uneventful. Cardiac CT at the 1-month follow-up confirmed a complete LAA seal without leak or device-related thrombus (Figure 7, Video 6). The maximum device size on cardiac CT was 34 mm, corresponding to an appropriate compression rate of 15%. At the 6-month follow-up, the patient remained asymptomatic with no recurrence of palpitation.Figure 7. Follow-Up CT FindingsCardiac CT at 1-month follow-up showing stable device position, appropriate compression (15%), and no device-related thrombus. CT = computed tomography; LA = left atrium; LSPV = left superior pulmonary vein; LV = left ventricle.
Discussion
This case highlights 3 important findings: 1) Concomitant PFA and LAAO is feasible in patients with LAA-origin AT; 2) PFA within the LAA may cause significant edema and narrowing of the LAA orifice, complicating device sizing; and 3) prudent device selection guided by pre-PFA imaging is crucial to avoid late peridevice leak.
LAA-origin AT is rare, representing a small subset of focal ATs.1 Outcomes with RFCA are variable, and distal LAA foci are often resistant to RFCA.2^,^3 PFA has emerged as an attractive alternative therapy because of its myocardial selectivity, reduced risk of collateral injury, and favorable safety profile. Recent studies suggest its efficacy in targeting LAA-origin AT.4 On the other hand, electrical LAA isolation raises concerns about postprocedural thrombus formation and thromboembolic events. Observational studies have documented increased stroke risk after electrical LAA isolation.5, 6, 7 LAAO represents a rational adjunct to mitigate this risk.
Previous reports have indicated that electroporation can create acute edema at the ridge during PFA procedures for AF with LAAO.8^,^9 In the present case, PFA within the LAA induced significant tissue edema, reducing the maximal orifice diameter by 5 mm and causing swelling of the pectinate muscle. These changes complicated LAAO device sizing. One possible strategy is to delay device implantation until edema resolves, allowing accurate sizing. However, this waiting approach exposes the patient to thromboembolic risk. Alternatively, proceeding with concomitant LAAO requires careful consideration. Downsizing the device based on post-PFA imaging risks late peridevice leak once edema resolves. Rather, maintaining device size based on pre-PFA imaging, with intentional overcompression, provides a more secure LAA sealing.
Follow-up cardiac CT imaging in this case confirmed the effectiveness of the latter strategy, with no leak and appropriate device compression rate. These findings demonstrate that device sizing should rely on pre-PFA imaging rather than immediate post-PFA imaging, which may underestimate the true orifice size.
Of note, in our case, swelling of the pectinate muscle made deployment of a 40-mm device technically challenging. Thus, procedural success also depends on meticulous intraprocedural manipulation by experienced operators and high-quality intraprocedural imaging to guide deployment.
Although the Watchman FLX Pro was successfully used here, the feasibility of other LAAO devices in the context of PFA for LAA-origin AT remains to be investigated. More clinical experience will be necessary to establish standardized strategies for concomitant therapy. Recently, the OPTION trial evaluated adjunctive LAAO performed at the time of catheter ablation for atrial fibrillation and demonstrated noninferior outcomes for safety and adverse events compared with oral anticoagulation.10 Our experience of concomitant PFA and LAAO for LAA-origin AT aligns with these findings, supporting the feasibility and potential safety advantage of this combined approach.
Conclusions
Concomitant PFA and LAAO for LAA-origin AT is feasible. However, careful device sizing based on pre-PFA imaging is essential to minimize the risk of late peridevice leak.
Funding Support and Author Disclosures
The authors have reported that they have no relationships relevant to the contents of this paper to disclose.Take-Home Messages
- •Pulsed-field ablation for LAA–origin atrial tachycardia can cause significant tissue edema and narrowing of the orifice.
- •Prudent selection of transcatheter left atrial appendage occlusion device and intentional overcompression, guided by preablation imaging findings, are crucial.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Yang Q.Ma J.Zhang S.Hu J.Liao Z.Focal atrial tachycardia originating from the distal portion of the left atrial appendage: characteristics and long-term outcomes of radiofrequency ablation Europace 142201225426010.1093/europace/eur 30221933799 · doi ↗ · pubmed ↗
- 2Guo X.Zhang J.Ma J.Management of focal atrial tachycardias originating from the atrial appendage with the combination of radiofrequency catheter ablation and minimally invasive atrial appendectomy Heart Rhythm 1112014172510.1016/j.hrthm.2013.10.01724103224 · doi ↗ · pubmed ↗
- 3Xie H.-Y.Feng Z.-C.Guo X.-G.Sun Q.Yang J.-D.Ma J.Treatment strategy in atrial tachycardia originating from the atrial appendage Front Physiol 13202290251310.3389/fphys.2022.902513 PMC 926337135812330 · doi ↗ · pubmed ↗
- 4La Fazia V.M.Mohanty S.Gianni C.Feasibility and safety of pulsed field ablation for coronary sinus and left atrial appendage isolation and mitral isthmus ablation: acute and chronic findings Circ Arrhythm Electrophysiol 182025 e 01402610.1161/CIRCEP.125.01402640874318 · doi ↗ · pubmed ↗
- 5Kim Y.G.Shim J.Oh S.-K.Lee K.-N.Choi J.-I.Kim Y.-H.Electrical isolation of the left atrial appendage increases the risk of ischemic stroke and transient ischemic attack regardless of postisolation flow velocity Heart Rhythm 151220181746175310.1016/j.hrthm.2018.09.01230502771 · doi ↗ · pubmed ↗
- 6Fink T.Vogler J.Heeger C.-H.Impact of left atrial appendage closure on LAA thrombus formation and thromboembolism after LAA isolation JACC Clin Electrophysiol 61320201687169710.1016/j.jacep.2020.07.00333334448 · doi ↗ · pubmed ↗
- 7Dhorepatil A.Lang A.L.Lang M.Long-term stroke risk in patients undergoing left atrial appendage ablation with and without complete isolation Front Cardiovasc Med 8202176283910.3389/fcvm.2021.762839 PMC 869567534957252 · doi ↗ · pubmed ↗
- 8Tam M.T.K.Kojodjojo P.Lam Y.-Y.Combined pulsed field ablation and left atrial appendage occlusion: a multicenter comparative study Heart Rhythm 221020252579258410.1016/j.hrthm.2025.03.196840122196 · doi ↗ · pubmed ↗