Cancer screening information-seeking before and during the COVID-19 pandemic
Heather Platter, Adaora Ezeani, Travis Hyams, Grace C. Huang, William M.P. Klein, Robin C. Vanderpool

TL;DR
This study found that cancer screening information-seeking changed during the pandemic, with increased interest in breast cancer and decreased interest in other cancers.
Contribution
The study provides new insights into how the pandemic affected public cancer screening information-seeking behaviors.
Findings
Post-pandemic, breast cancer screening inquiries increased while others decreased.
Telephone inquiries increased, but email and chat inquiries decreased.
Referrals to cancer detection programs increased significantly.
Abstract
The COVID-19 pandemic disrupted routine cancer screening; however, it is unclear whether the public’s cancer screening information-seeking behaviors changed. Our study examined cancer screening information-seeking before and after pandemic onset using data from the National Cancer Institute’s Cancer Information Service. We analyzed screening inquiries from general public users before (3/27/19–3/26/20) and after (3/27/20–3/26/21) pandemic onset. We examined point of access, subjects of interaction, and referrals. There were more general public cancer screening inquiries made post-pandemic onset (n = 1069; 56.1%) compared to before (n = 837, 43.9%). Although the proportion of breast cancer screening inquiries increased after pandemic onset, inquiries for cervical, colorectal, and other cancers decreased. Telephone inquiries increased, whereas email and instant chat inquiries decreased.…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
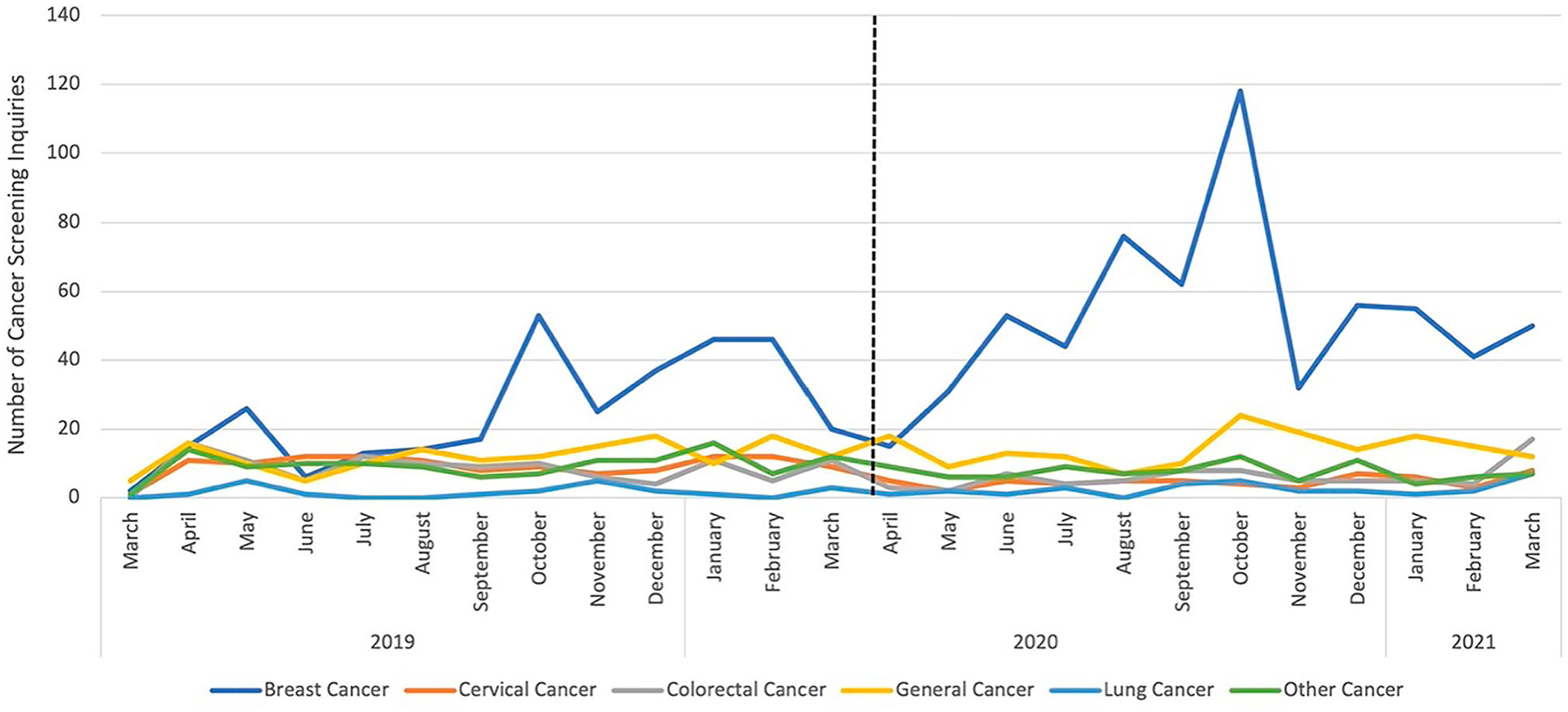 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCOVID-19 and healthcare impacts · Global Cancer Incidence and Screening · Colorectal Cancer Screening and Detection
Introduction
Routine guideline-based screening allows for the early identification of precancerous lesions or established cancers, which improves individual longevity and population health [1]. The COVID-19 pandemic interrupted routine medical care procedures such as cancer screening due to stay-at-home orders, reduced medical facility staffing, cancelation of elective medical procedures, and hesitancy to enter public spaces [2]. Data show that by June 2020, 40% of United States (U.S.) adults reported avoiding medical care, such as cancer screening, due to COVID-19 concerns [3]. Statistical models suggest an excess of 10,000 deaths from breast and colorectal cancer over the next decade due to pandemic screening delays [4].
Cancer information-seeking is an important behavior across the cancer control continuum [5] and seeking information about screening and early detection is associated with improved adherence and timeliness of screening [6]. However, little research has focused on cancer information-seeking behaviors during the COVID-19 pandemic. Vanderpool et al. [7] found that people who inquired about COVID-19 to the U.S. National Cancer Institute’s (NCI) Cancer Information Service (CIS) were significantly more likely to ask about cancer diagnosis, treatment, and post-treatment compared to those who did not inquire about COVID-19. Likewise, while cancer screening information-seeking could be more substantial during the pandemic given potential concerns about missing a screening, information-seeking may decrease due to the shift in health priorities during a heightened state of emergency. It is important to understand information-seeking in the context of health emergencies to adequately prepare for future emergencies.
In this study, we specifically examined cancer screening information-seeking before and after the COVID-19 pandemic onset using data over a 24-month period from the U.S. NCI’s CIS, a well-known and trusted multichannel source of cancer information. We examined CIS point of access (e.g. telephone, instant chat), which describes how the general public contacted the CIS, to determine any differences before and after pandemic onset. We also examined additional topics mentioned by the general public when inquiring about cancer screening, and how CIS referrals to other resources differed during the study period. We hypothesized that cancer screening information-seeking would decrease after the pandemic onset due to interrupted routine medical care procedures and a focus on the pandemic. Findings can be used to contextualize longitudinal, downstream changes in cancer screening, incidence, and mortality following public crises, and have implications for local and state public health agencies to optimize communication of cancer information during future public health emergencies.
Methods
Data source
Established by NCI in 1975, the CIS is a publicly available source of accurate, up-to-date cancer information accessible to the general public, health professionals, caregivers, and patients in English and Spanish language [8]. The program provides cancer information through various modalities, such as email ([email protected]), an instant chat service (LiveHelp), social media (i.e. Face-book, Instagram, LinkedIn, Twitter, YouTube), and telephone (1-800-4-CANCER). Users have access to publications, recorded cancer information, or an information specialist who can answer cancer-related questions and provide individually tailored information [9].
Study sample
Recorded via an electronic contact record form, CIS information specialists (IS) are trained to code each inquiry using multiple variables, such as the phase of the cancer continuum an inquiry centers on (e.g. screening, diagnosis, treatment) and user type (e.g. cancer survivor, caregiver, general public, health professionals, tobacco user). For the purposes of this analysis, we examined cancer screening inquiries made by general public CIS users as they totaled the majority of all cancer screening inquiries (n = 1906, 76.9%). General public CIS users included members of the public or their family members and friends who may have had precancerous or non-cancerous conditions or cancer-related symptoms. The timeline for this study was determined by the first general public CIS user inquiry received about cancer screening after pandemic onset, which occurred on March 27, 2020. Cancer screening inquiries were compared across two equal periods: (1) one year before the COVID-19 pandemic: March 27, 2019-March 26, 2020, and (2) one year after the pandemic onset: March 27, 2020-March 26, 2021. As CIS programmatic data are fully deidentified, related analyses did not qualify as human subjects research by Westat (No. 00005551) and U.S. National Institutes of Health (No. 000815) Institutional Review Boards.
Measures
We examined several variables to understand information-seeking about cancer screening among general public CIS users before and after pandemic onset (March 27, 2019-March 26, 2020 vs. March 27, 2020-March 26, 2021). Variables included: (1) CIS point of access (email, Live-Help, social media, telephone); (2) subjects of interaction to understand what subjects CIS users inquired about in relation to cancer screening; and (3) types of referrals offered to CIS users, such as where someone can go to get screened. Subjects were aggregated into five categories: (1) ‘finding healthcare services to manage cancer care’; (2) ‘general cancer questions’; (3) ‘managing costs and medical information’; (4) ‘other’; and (5) ‘tests to screen, diagnose, stage, or monitor cancer’. For example, finding healthcare services included finding support, transportation, and lodging for screening services. There were eight users without a subject of interaction code and were treated as missing. IS referrals included: (1) ‘Centers for Disease Control and Prevention National Breast and Cervical Cancer Early Detection Program (CDC NBCCEDP)’; (2) ‘health professional’; (3) ‘national or community organization (includes referrals to community organizations and government programs)’; (4) ‘other (includes any other recommendation that does not fall in the before listed categories)’; and (5) ‘no referral’.
We calculated cancer screening inquiries by general public CIS users before and after the pandemic onset for each cancer site. Cancer sites of interest were categorized as ‘breast’, ‘cervical’, ‘colorectal’, and ‘lung and bronchus’, representing cancer types with A or B screening test recommendations from the U.S. Preventive Services Task Force (USPSTF) [1]. We combined the 28 remaining cancer sites into a single category, ‘other’, to account for cancer screening inquiries without A or B USPSTF ratings. The largest ‘other’ inquiry was prostate cancer (n = 84) and 16 ‘other’ cancers had five inquiries or less (n = 42). Users who inquired about cancer screening, but did not specify a cancer site, were categorized as ‘general’. For each CIS inquiry, IS could code up to four subjects of interaction categories, three referrals, and two cancer sites.
Data analysis
We calculated descriptive statistics of cancer screening inquiries from general public CIS users before and after the pandemic onset. To illustrate trends over time, we graphed frequencies. We computed descriptive statistics for point of access, subjects of interaction, and referrals for the pre – and during-pandemic periods. To examine trends over time, we performed bivariate analyses using chi-squared tests of independence to examine the association between these variables and period for each cancer site. We considered associations statistically significant at p ≤ 0.05. We conducted analyses with IBM SPSS Statistics Subscription for Mac OS Build 1.0.0.1058.
Results
Over a 24-month period (March 2019–March 2021), there were 8868 total inquiries to the CIS across the cancer care continuum from general public CIS users. Of these general public inquiries, 1906 inquired about cancer screening: 837 (43.9%) inquiries were pre-pandemic and 1069 (56.1%) during the pandemic.
Cancer site
Cancer site inquiries across the two periods included breast (n = 958), cervical (n = 179), colorectal (n = 183), general (n = 327), lung (n = 51), and 28 other cancers combined (n = 213). Before the pandemic, breast cancer (n = 319, 38.1%), general cancer (n = 150, 17.9%), and cervical cancer (n 133, 15.9%) accounted for more than two-thirds of screening inquiries. After pandemic onset, breast cancer (n = 639, 59.8%) alone made up almost two-thirds of the inquiries, followed by general cancer screening (n = 177, 16.6%). The proportion of breast cancer inquiries increased by 21.7% after the pandemic onset (x^2^ = 88.13, p < .001), the only increase among all cancer types (Table 1).
Figure 1 shows the monthly totals of cancer screening CIS inquiries pre – and post-pandemic onset separated by cancer type. Breast cancer screening inquiries peaked in October 2019 (n = 53), more than tripling inquiries from September 2019 (n = 17). Breast cancer inquiries decreased by 28 in November 2019, then rebounded to 46 across January and February 2020. The decrease may be due to end-of-year holidays in November and December. After the pandemic onset, breast cancer inquiries in June 2020 were more than eight times that of June 2019 and matched October 2019 (Breast Cancer Awareness Month). Inquiries peaked again in October 2020 (n = 118), followed by a decline in November 2020 (n = 32), which is similar to end-of-year trends from 2019.
Point of access
General public cancer screening inquiries from telephone calls significantly increased by 14.9% during the pandemic (64.3%; n = 538 to 79.2%; n = 847; p < .001). Inquiries by email decreased by 3.8% (7.4%; n = 62 to 3.6%; n = 38; p < = .001) and LiveHelp decreased by 10.6% (25.1%; n = 210 to 14.5%; n = 155; p < .001). Among cancer sites, breast cancer received the highest proportion of telephone-based inquiries, which increased by 21.3% after pandemic onset (48.1%; n = 256 to 69.4%; n = 587; p < 0.001). The highest proportion of LiveHelp inquiries pre-pandemic was for cervical cancer (31.9%; n = 67), but general cancer was higher after the pandemic onset (28.4%; n = 44). General cancer had the highest proportion of inquiries for email (27.4%; n = 17 vs 36.8%; n = 14) and social media (40.7%; n = 11 vs 65.5%; n = 19) across both periods.
Subjects of interaction
Three subjects of interaction had notable differences in cancer screening inquiries before and after the pandemic onset: (1) finding healthcare services (n = 916); (2) tests (n = 530); and (3) managing costs (n = 503). There was a significant increase after the pandemic onset of 17.1% (n = 272) and 22.6% (n = 223) for inquiries coded as finding healthcare services and managing costs, respectively (p < 0.001). However, inquiries about tests and other subjects of interactions decreased (p < 0.001; Table 1).
When examining subjects of interaction by cancer site, there was a large increase after the pandemic onset for finding healthcare services among breast cancer inquiries (53.1%; n = 171 to 77.6%; n = 461; p < .001). The greatest decrease for finding healthcare services was for colorectal cancer inquiries (18.6%; n = 60 to 5.4%; n = 32; p < .001). The largest increase in general cancer questions was for breast cancer (14.3%; n = 18 to 28.7%; n = 54; p < .003) and the biggest decrease was cervical cancer (26.2%; n = 33 to 6.4%; n = 12; p < .001). For managing costs, the only increase was for breast cancer (52.2%; n = 60 to 83.8%; n = 325; p < .001), whereas the largest decrease was colorectal cancer (26.1%; n = 30 to 7%; n = 27; p < .001). For tests, the biggest increase was for breast cancer inquiries (34.8%; n = 96 to 54.3%; n = 138; p < .001) and the biggest decrease was for other cancers (19.2%; n = 53 to 9.8%; n = 25; p = .002). The only significant change for other subjects of interaction was for cervical cancer (18.7%; n = 46 to 10.7%; n = 19; p = .025) (Table 2).
Referrals given by CIS staff
The most common IS referral was for a health professional (64.4%; n = 539), but this percentage decreased to 52.1% (n = 557) after pandemic onset (p < 0.001; Table 1). The second highest referral was for national or community organizations (37.8%; n = 316), which increased to 60.1% (n = 643; p < 0.001). Furthermore, 32.8% (n = 351) of referrals were to CDC NBCCEDP after pandemic onset, an increase from the 9.3% (n = 78) pre-pandemic (p < .001). Specifically, CDC NBCCEDP referrals increased for breast cancer (83.3%; n = 65 to 93.4%; n = 328; p < .001) and decreased for colorectal (6.4%; n = 5 to 1.4%; n = 5; p = .008). Referrals to health professionals increased for breast cancer (31.4%; n = 169 to 49.2%; 274; p < .001) yet decreased for cervical (17.6%; n = 95 to 8.8%; n = 49; p < .001) and colorectal cancer (16.5%; n = 89 to 9.2%; n = 51; p < .001). The only increase for national or community organizations after pandemic onset was for breast cancer (55.7%; n = 176 to 79.9%; n = 514; p < .001), whereas there were decreases for cervical (11.1%; n = 35 to 5.3%; n = 34; p = .001), colorectal (17.4%; n = 55 to 6.4%; n = 41; p < .001), and other cancers (8.2%; n = 26 to 4.4%; n = 28; p = .014). Referrals to other places increased for breast cancer (42.6%; n = 124 to 54.3%; n = 170; p = .004) and decreased for cervical cancer (12.7%; n = 37 to 6.4%; n = 20; p = .008). No referrals showed an increase for general cancer (26.4%; n = 23 to 48.1%; n = 38; p = .004) and a decrease for cervical cancer (20.7%; n = 18 to 7.6%; n = 6; p = .017). It is noteworthy that there was a significant increase in all referral types for breast cancer-related inquiries after the onset of the pandemic (Table 3).
Discussion
Information-seeking has been shown to be associated with cancer screening adherence [6]; therefore, it may be used as a potential indicator of cancer screening behavior in future public health emergencies. CIS inquiries may demonstrate patterns in cancer screening information-seeking when essential healthcare services are disrupted. We hypothesized that health information-seeking about cancer screening would decrease after the pandemic onset. On the contrary, we found that the proportion of cancer screening inquiries increased by 12.2% (in absolute terms) after pandemic onset. It is notable that this increase was driven primarily by breast cancer inquiries, despite a substantial decrease in the first two months of COVID-19 (March-April 2020). This suggests the majority of inquiries declined at the early onset of the pandemic when hospitals, healthcare centers, and medical providers postponed or canceled non-emergent care and cancer screenings [10]. As with breast cancer, cervical and general cancer inquiries declined in March, whereas colorectal, lung, and other cancer inquiries started to decline in April. Similar studies have used Google Trends to examine public interest in cancer screenings following COVID-19, finding a sharp decline in information-seeking regarding screening tests, such as colonoscopies, human papillomavirus testing, and Pap smears [11,12]. This trend was also similar to previously reported sharp declines and rebound, at least for breast cancer, in cancer screening [13].
We observed a twofold increase in colorectal cancer screening inquiries in March 2020 compared to February 2020, with March 2021 inquiries being more than four times that of February 2021, which coincides with National Colorectal Cancer Awareness Month. We witnessed a peak in breast cancer inquiries during Breast Cancer Awareness Month (October 2019, October 2020), yet October 2020 inquiries were more than twice that of 2019. As stay-at-home emergency orders started to ease by June 2020 [14], breast cancer inquiries matched those in October 2019 (n = 53). Hospitals and medical facilities began to reopen, which may have motivated the general public to contact the CIS about cancer screening.
The CIS experienced a significant increase in telephone inquiries after pandemic onset, whereas all other points of access decreased. The surge in telephone inquiries may be due to the increased urgency for expert information and personalized advice on cancer screening during a crisis. Vanderpool et al. [7] found higher telephone usage among general public CIS users, cancer survivors, and tobacco users who inquired about COVID-19 compared to users who did not inquire about COVID-19, indicating that there may be a preference to speak with a ‘live person’ during health emergencies.
Notably, in May 2019, the CIS conducted a communication campaign in the National Library of Medicine Patient Magazine, resulting in an increase of 14,000 inquiries, a majority through LiveHelp. This campaign may account for the higher number of LiveHelp inquiries in 2019.
Study results emphasize the need for local, state, and national public health agencies to strengthen bidirectional information services to communicate essential health information during a crisis [15]. The President’s Cancer Panel on cancer screening recommends using the four-part health literacy framework to develop and disseminate effective communications about cancer screening to empower the public to make decisions about their health [16]. It is important for public health agencies to consider using this framework to develop targeted messaging for individual cancer types and tailor messages to specific populations, especially those with low rates of cancer screening. Furthermore, public health agencies may consider improving the promotion and use of multiple communication channels (e.g. telephone, email) to improve interpersonal communication with the public [7,16]. Interpersonal communication resources via trusted public health organizations and governmental agencies can support the public with information overload, navigating uncertainty, and combating misinformation; provide an outlet to discuss emotional and health-related stressors; and provide referrals to medical, public health, or social service organizations [17,18].
Data demonstrate a significant change in various types of referrals offered to general public CIS users across the study period. The increase in breast cancer inquiries and decrease across other cancer sites after pandemic onset may correspond with the increase in the proportion of referrals to the CDC NBCCEDP. Referrals to programs that serve the uninsured or underinsured, like the CDC NBCCEDP, reduce breast and cervical cancer disparities by providing critical cancer screening and diagnostic services to people with low income and inadequate health insurance [19]. DeGroff et al. [10] examined the impact of the pandemic on the CDC NBCCEDP’s screening services, finding that screening tests declined by 87% in April 2020 for breast cancer. Testing began to recover in May 2020, similar to breast cancer inquiries in this study, although by June it continued to be below the 5-year monthly average [10]. We also found an increase in referrals to national and community organizations or other government programs and a decrease to healthcare providers. Since the beginning of the pandemic, healthcare systems and providers have postponed or canceled services such as elective surgical procedures and cancer screening tests, which may have accounted for the decrease in these referrals [20,21].
Limitations
Data from this study may not be generalizable to the broader general public as the study was based on a sample of users who proactively contacted a national cancer information service for information about cancer screening. Moreover, given that personal identifiable information is not collected by CIS staff, each contact was treated as a unique user; therefore, it is unknown if any of the users were repeat contacts. Third, sociodemographic data are randomly collected after CIS interactions to minimize respondent burden per White House Office of Management and Budget mandates; these data were excluded from analysis due to small sample sizes within sociodemographic groups. Finally, although the data reported here are quantitative, user inquiries are more qualitative in nature and are coded by trained CIS staff who may be subject to internal biases. To reduce the potential for such biases, they receive extensive training on topics such as patient-centered cancer information in order to code inquiries accurately.
Conclusion
Cancer screening information-seeking among general public CIS users experienced a sharp decrease following the pandemic onset in March 2020. Breast cancer inquiries quickly rebounded by June 2020, demonstrating an elevated demand for information about breast cancer screening. Furthermore, the increase in breast cancer screening inquiries associated with finding healthcare services reflected a critical period after the pandemic when cancer screening programs were delayed. The observed increase may point to future increases in screening behaviors, requiring healthcare systems to monitor resultant backlog and delay of catch-up screening appointments. Therefore, it is imperative to develop a strategy to optimize cancer screening activities during the pandemic recovery period. In one study, microsimulation models showed – between 2020 and 2060 – continued screening after the maximum recommended age (e.g. after 74 years for breast cancer) had similar cancer incidence and cancer-specific mortality rates as if screening was undisrupted [22]. Furthermore, these data may give insight into the nature of cancer screening information-seeking during future pandemics and public health emergencies, which can help local, state, and federal agencies optimize their communication of cancer information. Future preparation can support the expansion or development of contact access points as well as training staff to clearly communicate health information in times of stress. Special attention should also be paid to guideline-recommended cervical, colorectal, and lung cancer screening tests considering the reduced information-seeking CIS inquiries among the general public. In addition, study results highlight the necessity of enlisting national and community organizations to alleviate the stress of the pandemic on healthcare systems. Connecting CIS users to community and national programs that provide screening and diagnostic services may be an effective method to alleviate barriers in providing cancer screening information and care during national health crises.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1A and B recommendations. US Preventative Services Task Force. 2017 [cited 2021 Aug 20]. Available from: www.uspreventiveservicestaskforce.org/uspstf/recommendation-topics/uspstf-and-b-recommendations.
- 2Papautsky E, Rice D, Ghoneima H, Characterizing health care delays and interruptions in the United States during the COVID-19 pandemic: internet-based, cross-sectional survey study. JMIR. 2021;23(5):e 25446. doi:10.2196/2544633886489 PMC 8136407 · doi ↗ · pubmed ↗
- 3Czeisler ME, Marynak K, Clarke KEN, Delay or avoidance of medical care because of COVID-19–related concerns — United States. June 2020 [cited 2021 Jun 28]. Available from: https://www.cdc.gov/mmwr/volumes/69/wr/mm 6936 a 4.htm.
- 4Sharpless NE. COVID-19 and cancer. Science. 2020; 368(6497):1290. doi:10.1126/science.abd 337732554570 · doi ↗ · pubmed ↗
- 5National Cancer Institute Division of Cancer Control and Population Sciences (NCI DCCPS). Cancer Control Continuum. 2020 [cited 2024 Apr 2]. Available from: https://cancercontrol.cancer.gov/about-dccps/about-cc/cancer-control-continuum.
- 6Shneyderman Y, Finney Rutten LJ, Arheart KL, Health information seeking and cancer screening adherence rates. JCE. 2016;31(1):75–83. doi:10.1007/s 13187-015-0791-6 · doi ↗
- 7Vanderpool RC, Huang GC, Mollica M, Cancer information-seeking in an Age of COVID-19: findings from the National Cancer Institute’s Cancer Information Service. J Health Commun. 2021;36(1):89–97. doi:10.1080/10410236.2020.1847449 · doi ↗
- 8Bright MA. The National Cancer Institute’s Cancer Information Service: A premiere cancer information and education resource for the nation. JCE. 2007;22(2):S 2–S 7. doi:10.1007/BF 03174340 · doi ↗