Clinical implications of an intraoperative margin-positive distal bile duct in perihilar cholangiocarcinoma: international multicentre cohort study
Hasan Ahmad Al-Saffar, Britte H E A ten Haaft, Rebecca Marino, Mario De Bellis, Pim B Olthof, Sondre Busund, Nicolai A Schultz, Stefan Gilg, Andrea Ruzzenente, Bas Groot Koerkamp, Joris I Erdmann, Francesca Ratti, Sheraz Yaqub, Hans-Christian Pommergaard, Christian Sturesson

TL;DR
This study finds that re-surgery after a positive bile duct test during cholangiocarcinoma surgery can achieve good outcomes without increasing risks.
Contribution
The study provides new evidence on the effectiveness and safety of intraoperative re-resection or pancreatoduodenectomy for margin-positive bile ducts in cholangiocarcinoma.
Findings
11.1% of patients had a positive distal bile duct frozen section.
Re-resection or pancreatoduodenectomy achieved margin clearance in 69% of patients.
Long-term survival was comparable to patients with primary negative margins.
Abstract
The short- and long-term outcomes of intraoperative extension of the distal bile duct margin following a positive frozen section in patients with perihilar cholangiocarcinoma remain poorly characterized. Between 1 January 2003 and 1 January 2023, consecutive patients at seven high-volume European hepatopancreatobiliary centres undergoing major hepatectomy for perihilar cholangiocarcinoma with frozen-section analysis of the distal bile duct and subsequent intraoperative management were included retrospectively. The primary endpoint was achievement of an overall R0 resection following distal bile duct re-resection or additional pancreatoduodenectomy after identification of a positive distal bile duct frozen section. Secondary endpoints included overall survival, disease-free survival, and major postoperative complications (Clavien–Dindo grade ≥ IIIa). Outcomes were reported as adjusted…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
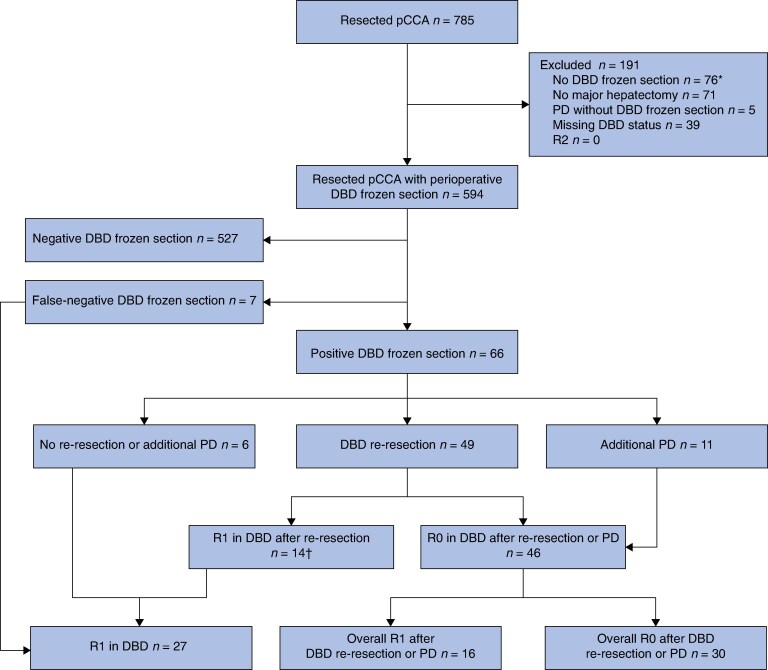 Fig. 1
Fig. 1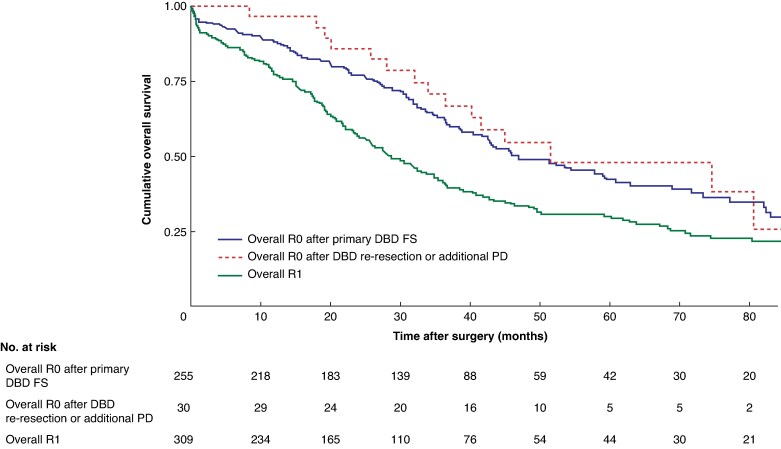 Fig. 2
Fig. 2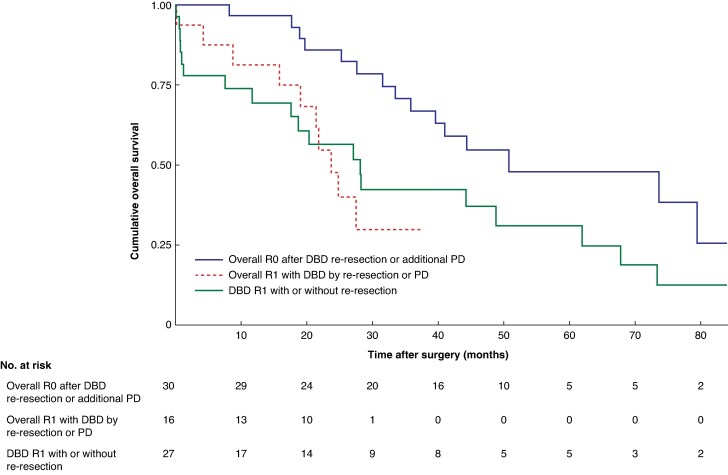 Fig. 3
Fig. 3| Pathological outcome following DBD FS |
| |||
|---|---|---|---|---|
| Overall R1 ( | Overall R0 after re-resection or PD ( | Overall R0 after primary DBD FS ( | ||
|
| 67.4 (58.7–73.0) | 67.2 (57.1–71.8) | 67.2 (59.8–73.4) | 0.650‡ |
| Missing | 0 | 0 | 0 | |
|
| 0.790† | |||
| Female | 116 (37.5%) | 13 (43%) | 100 (39.2%) | |
| Male | 193 (62.5%) | 17 (57%) | 155 (60.8%) | |
| Missing | 0 | 0 | 0 | |
|
| 0.017† | |||
| 2003–2009 | 20 (6.5%) | 1 (3%) | 29 (11.4%) | |
| 2010–2016 | 131 (42.4%) | 10 (33%) | 78 (30.6%) | |
| 2017–2023 | 158 (51.1%) | 19 (64%) | 148 (58.0%) | |
|
| 0.734† | |||
| I | 78 (25.2%) | 6 (20%) | 57 (22.4%) | |
| II | 167 (54.1%) | 15 (50%) | 143 (56.1%) | |
| III | 64 (20.7%) | 9 (30%) | 55 (21.6%) | |
|
| 24.0 (22.1–26.5) | 23.9 (21.7–26.4) | 24.8 (22.2–26.8) | 0.405‡ |
| Missing | 29 | 1 | 25 | |
|
| 206 (67.1%) | 21 (70%) | 184 (72.2%) | 0.318† |
| Missing | 2 | 0 | 0 | |
|
| 148 (46–546) | 84 (59–247) | 126 (39–420) | 0.900‡ |
| Missing | 81 | 2 | 48 | |
|
| < 0.001† | |||
| I | 6 (1.9%) | 3 (10%) | 7 (2.7%) | |
| II | 24 (7.8%) | 7 (23%) | 39 (15.3%) | |
| IIIa | 115 (37.2%) | 12 (40%) | 68 (26.7%) | |
| IIIb | 69 (22.3%) | 4 (13%) | 86 (33.7%) | |
| IV | 95 (30.8%) | 4 (13%) | 55 (21.6%) | |
| Missing | 0 | 0 | 0 | |
|
| < 0.001† | |||
| ERCP | 90 (29.1%) | 10 (33%) | 74 (29.0%) | |
| PTC | 129 (41.7%) | 15 (50%) | 89 (34.9%) | |
| Both | 44 (14.2%) | 2 (7%) | 24 (9.4%) | |
| None | 46 (14.9%) | 3 (10%) | 68 (26.7%) | |
| Missing | 0 | 0 | 0 | |
|
| 75 (24.3%) | 7 (23%) | 40 (15.7%) | 0.039† |
| Missing | 0 | 0 | 0 | |
|
| 0.009† | |||
| Left-sided hemihepatectomy | 137 (44.3%) | 10 (33%) | 142 (55.7%) | |
| Right-sided hemihepatectomy | 163 (52.8%) | 20 (67%) | 111 (43.5%) | |
| Central hepatectomy | 9 (2.9%) | 0 (0%) | 2 (0.8%) | |
| Missing | 0 | 0 | 0 | |
|
| 77 (24.9%) | 8 (27%) | 44 (17.3%) | 0.071† |
| Missing | 0 | 0 | 0 | |
| Pathological outcome following DBD FS |
| |||
|---|---|---|---|---|
| Overall R1 ( | Overall R0 after re-resection or PD ( | Overall R0 after primary DBD FS ( | ||
|
| 0.024¶ | |||
| pT1 | 39 (12.7%) | 0 (0%) | 26 (10.3%) | |
| pT2 | 137 (44.8%) | 18 (60%) | 128 (50.8%) | |
| pT3 | 96 (31.4%) | 11 (37%) | 86 (34.1%) | |
| pT4 | 34 (11.1%) | 1 (3%) | 12 (4.8%) | |
| Missing | 3 | 0 | 3 | |
|
| 143 (46%) | 16 (53%) | 103 (40.4%) | 0.217¶ |
| Missing | 0 | 0 | 0 | |
|
| 12 | |||
| Positive DBD with re-resection | 0 | |||
| Positive DBD without re-resection or PD | 1 | |||
| Negative DBD | 11 | |||
| Missing | 0 | |||
|
| 27 | |||
| DBD re-resection | 14 (52%) | |||
| Positive DBD without re-resection or PD | 13 (48%) | |||
| Missing | 0 | |||
|
| 91 | |||
| DBD re-resection | 6 | |||
| Additional PD | 1 | |||
| Positive DBD without re-resection or PD | 6 | |||
| Negative DBD | 78 | |||
| Missing | 32§ | |||
|
| 244 | |||
| DBD re-resection | 12 | |||
| Additional PD | 4 | |||
| Positive DBD without re-resection or PD | 8 | |||
| Negative DBD | 220 | |||
| Missing | 47§ | |||
|
| 257 (87.1%) | 22 (79%) | 198 (80.8%) | 0.221¶ |
| Missing | 14 | 2 | 10 | |
|
| 0.243¶ | |||
| Well | 38 (14.4%) | 1 (4%) | 41 (17.4%) | |
| Moderate | 157 (59.5%) | 18 (75%) | 127 (54.0%) | |
| Poor | 69 (26.1%) | 5 (21%) | 68 (28.9%) | |
| Missing | 45 | 6 | 20 | |
|
| 28 (20–40) | 20 (17–28) | 21 (16–30) | < 0.001# |
| Missing | 45 | 1 | 18 | |
|
| 135 (43.4%) | 5 (17%) | 63 (24.7%) | < 0.001¶ |
| Missing | 0 | 0 | 0 | |
|
| 36 (11.7%) | 0 (0%) | 19 (7.5%) | 0.013¶ |
| Missing | 0 | 0 | 0 | |
|
| 171 (55.3%) | 17 (57%) | 116 (45.5%) | 0.054¶ |
| Missing | 0 | 0 | 0 | |
|
| < 0.001¶ | |||
| Local | 69 (40.4%) | 3 (18%) | 28 (24.1%) | |
| Liver | 26 (15.2%) | 3 (18%) | 30 (25.9%) | |
| Distant | 38 (22.2%) | 11 (65%) | 39 (33.6%) | |
| Multifocal | 29 (17.0%) | 1 (6%) | 13 (11.2%) | |
| Unknown | 9 (5.3%) | 0 (0%) | 6 (5.2%) | |
| Univariable analysis | Multivariable analysis | |||
|---|---|---|---|---|
| Hazard ratio |
| Hazard ratio |
| |
| Age (years)* | 1.00 (0.99, 1.01) | 0.396 | ||
|
| ||||
| Female | 1.00 (reference) | |||
| Male | 1.38 (0.91, 1.75) | 0.410 | ||
|
| ||||
| 2017–2023 | 1.00 (reference) | 1.00 (reference) | ||
| 2010–2016 | 1.31 (1.03, 1.66) | 0.022 | 1.01 (0.78, 1.30) | 0.923 |
| 2003–2009 | 1.67 (1.18, 2.36) | 0.003 | 1.23 (0.84, 1.79) | 0.280 |
|
| ||||
| I | 1.00 (reference) | |||
| II | 0.95 (0.72, 1.26) | 0.758 | ||
| III | 1.29 (0.93, 1.78) | 0.122 | ||
| BMI (kg/m2)* | 0.99 (0.97, 1.00) | 0.342 | ||
|
| ||||
| No | 1.00 (reference) | 1.00 (reference) | ||
| Yes | 1.29 (1.02, 1.64) | 0.028 | 1.24 (0.97, 1.59) | 0.083 |
| CA19-9 (units/ml)* | 1.00 (1.00, 1.00) | 0.002 | 1.00 (1.00, 1.00) | 0.002 |
|
| ||||
| I or II | 1.00 (reference) | 1.00 (reference) | ||
| IIIa | 1.69 (1.17, 2.44) | 0.004 | 1.22 (0.82, 1.81) | 0.322 |
| IIIb | 1.24 (0.84, 1.83) | 0.271 | 1.08 (0.71, 1.65) | 0.691 |
| IV | 1.57 (1.07, 2.31) | 0.019 | 1.00 (0.66, 1.55) | 0.971 |
|
| ||||
| Left sided hemihepatectomy | 1.00 (reference) | 1.00 (reference) | ||
| Right sided hemihepatectomy | 1.53 (1.23, 1.91) | < 0.001 | 1.27 (0.95, 1.70) | 0.099 |
| Central hepatectomy | 1.51 (0.66, 3.42) | 0.321 | 1.32 (0.57, 3.06) | 0.505 |
|
| ||||
| < III | 1.00 (reference) | 1.00 (reference) | ||
| ≥ III | 1.49 (1.20, 1.86) | < 0.001 | 1.17 (0.92, 1.50) | 0.186 |
|
| ||||
| No | 1.00 (reference) | 1.00 (reference) | ||
| Yes | 1.41 (1.14, 1.76) | 0.001 | 1.46 (1.16, 1.83) | < 0.001 |
|
| ||||
| Overall R0 after primary DBD FS | 1.00 (reference) | 1.00 (reference) | ||
| Overall R0 after DBD re-resection or additional PD | 0.91 (0.54, 1.54) | 0.736 | 0.84 (0.49, 1.44) | 0.536 |
| Overall R1 | 1.66 (1.32, 2.08) | < 0.001 | 1.82 (1.43, 2.33) | < 0.001 |
|
| ||||
| No | 1.00 (reference) | 1.00 (reference) | ||
| Yes | 1.34 (0.99, 1.83) | 0.055 | 1.19 (0.87, 1.64) | 0.263 |
|
| ||||
| Well | 1.00 (reference) | |||
| Moderate | 0.92 (0.69, 1.24) | 0.615 | ||
| Poor | 1.09 (0.77, 1.77) | 0.613 | ||
|
| ||||
| < 30 | 1.00 (reference) | 1.00 (reference) | ||
| ≥ 30 | 1.81 (1.46, 2.25) | < 0.001 | 1.59 (1.26, 2.00) | < 0.001 |
|
| ||||
| No | 1.00 (reference) | 1.00 (reference) | ||
| Yes | 0.62 (0.49, 0.739 | < 0.001 | 0.52 (0.40, 0.68) | < 0.001 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCholangiocarcinoma and Gallbladder Cancer Studies · Gallbladder and Bile Duct Disorders · Pancreatic and Hepatic Oncology Research
Introduction
Perihilar cholangiocarcinoma (pCCA) is a challenging malignancy with 5-year overall survival (OS) rates of between 38 and 47% following surgery with curative intent^1–3^. Few patients are eligible for curative resection because of poor clinical performance status, anatomical unresectability or metastatic disease at diagnosis^1,4^. Achieving a radical resection (R0) is considered crucial for long-term survival in surgically treated patients^4^. In most patients, R0 resection necessitates major hepatectomy with extrahepatic bile duct (EHBD) resection, and occasionally vascular resection and reconstruction^4^.
To ensure longitudinal margin clearance during surgery, frozen-section (FS) analysis of both proximal (PBD) and distal (DBD) bile duct margins is undertaken routinely^5^. If a positive margin (R1) is identified in the FS, intraoperative re-resection can be considered to achieve an R0 margin^6^. Extension of the PBD margin is often limited by the extent of liver that can be resected technically while leaving a sufficient liver remnant^5^. A recent European multicentre study^7^ also demonstrated no long-term benefit of PBD margin extension on positive FS.
In contrast, DBD re-resection into the cranial pancreatic head is not considered technically difficult, and harbours fewer technical difficulties and risks. Where margin involvement extends into the deep intrapancreatic portion of the DBD, an additional pancreatoduodenectomy (PD) may be performed to remove the whole DBD segment^8^.
Despite the utility of DBD re-resection, its oncological value has not been well studied, and data on associated postoperative morbidity remain unknown. Existing scarce evidence is based on small single-centre series^8–10^ from Eastern institutions, or studies^11^ that analysed the PBD and DBD together. Furthermore, the benefits of additional PD following a positive DBD FS remain unclear^10^, with some studies^12,13^ reporting postoperative mortality rates as high as 18%.
Given the lack of large-scale multicentre data, clarifying the oncological impact and perioperative risks of DBD re-resection or additional PD is critical for surgical decision-making. This international, multicentre cohort study aimed to investigate both short- and long-term outcomes in patients with resected pCCA, who underwent DBD re-resection or additional PD following a positive DBD FS.
Methods
Patients (aged ≥ 18 years) with histologically confirmed pCCA who underwent resection with curative intent between 1 January 2003 and 1 January 2023 were included from seven high-volume European hepatopancreatobiliary (HPB) centres: Karolinska University Hospital (Sweden), Copenhagen University Hospital (Denmark), Oslo University Hospital (Norway), IRCCS Ospedale San Raffaele Milano (Italy), G. B. Rossi University Hospital Verona (Italy), Amsterdam UMC (the Netherlands), and Erasmus UMC Rotterdam (the Netherlands). Retrospective data were collected from electronic medical records, including baseline characteristics, surgical and pathological reports, recurrence data, and survival status. All data were anonymized and collected in a standardized data file between January and April 2025. A minimum of 2 years of follow-up was required to ensure assessment of recurrence^14^. Owing to variable data availability, some centres contributed patients from an individual consecutive subset of the inclusion period. Exclusion criteria were: absence of DBD FS, patients not undergoing major hepatectomy, liver transplantation, concomitant PD without previous intraoperative DBD FS, R2 resection, and missing recurrence or DBD margin data. Variations in preoperative and postoperative work-up were accepted given the retrospective nature of the study, but were addressed by including only centres carrying out at least seven resections per year^15,16^. Ethical approval was obtained from the Danish Health Authority in the Capital Region of Denmark (R-23057752), the Regional Ethics Board in Stockholm (2022-06962-02), and the Institutional Review Board at Oslo University Hospital (25/02945). Informed consent was waived owing to the retrospective design. The study adhered to the STROBE guidelines^17^.
Definitions
The preoperative physical status of included patients was categorized according to the American Society of Anesthesiologists (AS) Physical Status classification^18^. All patients underwent major hepatectomy (≥ 3 Couinaud segments) with EHBD resection^6^. Regional lymphadenectomy was performed routinely. Intraoperative FS were taken from the DBD and assessed in real time by a pathologist followed by direct feedback to the surgeon. The DBD FS was classified as negative (no invasive carcinoma) or positive (presence of invasive carcinoma)^19^. Cases of high-grade dysplasia (HGD) were classified as negative, given the lack of consensus on its clinical relevance during the study period^20,21^. When the DBD FS was positive, DBD re-resection or PD was undertaken based on tumour extent at the surgeon’s discretion. If the final pathological results revealed invasive carcinoma despite a negative intraoperative DBD FS, the result was labelled false-negative; in the reverse situation, the result was labelled false-positive. Tumours were staged in accordance with the American Joint Committee of Cancer 8th edition^22^. Pathological evaluation was undertaken locally at each centre by expert HPB pathologists using International Collaboration on Cancer Reporting (ICCR) criteria^23^, including evaluation of the DBD, PBD, and radial margins (RMs)^24–27^. Overall R0 was defined by ≥ 1 mm clearance at all resection margins and dissection planes; and overall R1 as < 1 mm clearance at one or more resection margin or dissection plane. Because of the retrospective and multicentre nature of the study, central re-review of pathology slides was not feasible.
Outcomes
The primary outcome was the proportion of patients achieving an overall R0 margin following DBD FS or PD. Secondary outcomes included OS, disease-free survival (DFS), local recurrence, major morbidity (Clavien–Dindo grade ≥ IIIa within 90 days)^28^, postoperative significant bile leakage (International Study Group of Liver Surgery (ISGLS) grade B or C)^29^, postoperative intra-abdominal abscess requiring drainage, and 90-day mortality.
Statistical analysis
Statistical analyses were undertaken using R 3.5.3 (R Foundation for Statistical Computing, Vienna, Austria). Demographic and clinicopathological variables are documented with missing data. Categorical variables are reported as numbers and percentages, and continuous variables as median (interquartile range).
Clinicopathological variables were described and categorized into three groups to assess long-term outcomes of the DBD FS, with respective P values: overall R0 after primary DBD FS, overall R0 after DBD re-resection or additional PD, and overall R1. The overall R1 group included all patients with a final R1 status, irrespective of whether they underwent DBD re-resection, additional PD, or neither. Group differences were assessed using Pearson’s χ^2^ test for categorical data, and the Kruskal–Wallis test for continuous data.
Median follow-up was estimated using the reverse Kaplan–Meier method, from the date of surgery to death from any cause, loss to follow-up, or the end of the study (1 January 2025). OS was calculated from the date of surgery to date of death or last follow-up. DFS was calculated from date of surgery to date of radiologically confirmed recurrence or death.
Univariable and multivariable Cox regression models were used to identify predictors of OS and DFS, in accordance with the REMARK checklist^30^. Known prognostic factors^31–33^ and variables with P < 0.100 in the univariable analysis were included in the multivariable analysis. Results from the DBD margin, PBD margin, and RM were reported separately^24–27^, but censored from the analysis to avoid multicollinearity. Assumptions governing the Cox proportional hazards ratio (HR) were assessed graphically and tested using scaled Schoenfeld residuals in the cox.zph function of the R survival package. Of note, logistic regression analysis for 90-day mortality, Clavien–Dindo grade ≥ IIIa complications, bile leakage, and intra-abdominal abscess was not part of the initial study design but was performed post hoc; known prognostic factors^31–33^ or those with P < 0.200 in univariable analyses were examined in multivariable analysis. Missing data were handled through multiple imputation (mice package for R 3.5.1; 20 imputed data sets, 10 iterations). Survival differences between groups were tested using Kaplan–Meier curves and log rank tests. All P values were two-sided, and significance was set at P < 0.050.
Results
Baseline characteristics
A total of 785 patients underwent resection for pCCA. The final cohort included 594 patients who underwent intraoperative DBD FS (Fig. 1). Of these, 66 (11.1%) had a positive DBD margin during surgery, and 7 (1.2%) were found to have false-negative results. An additional four patients (0.7%) had HGD on DBD FS. No false-positives were reported. Preoperative features of all patients who underwent DBD FS analysis are presented at Table 1.
Study flow diagramReasons for omitting distal bile duct (DBD) frozen section (FS) analysis are presented in the section entitled Outcomes of positive DBD FS. †One patient had a false-negative DBD re-resection. pCCA, perihilar cholangiocarcinoma; PD, pancreatoduodenectomy.*
Outcomes of positive DBD FS
Among the 66 patients with a positive intraoperative DBD FS, 49 underwent re-resection of the DBD, and 11 had additional PD. Six patients received no further surgical intervention after the primary positive DBD FS, and 14 who underwent DBD re-resection with secondary positive DBD FS did not proceed to additional PD. Reasons for not performing DBD re-resection or additional PD included frailty (13), a positive PBD FS (6) or false-negative DBD re-resection (1).
Although 46 of the 66 patients achieved R0 at the DBD after re-resection or additional PD, only 30 (45%) had an overall R0 margin on the final pathology because of remaining R1 margins at the PBD, RM, or both. Of note, 31 patients (47%) with a positive DBD FS had concurrent involvement of the PBD margin and/or RM (Table 2); among these, DBD re-resection was performed in 22, and additional PD in 4. All patients undergoing additional PD whose margin status remained R1 had RM involvement only (3), or RM involvement with false-negative PBD FS (1). In four of seven patients with a false-negative DBD FS, there was concurrent involvement of the PBD margin and/or RM.
Clinicopathological features
Overall R1 resection was associated with a higher T category (P = 0.024) and larger tumours (P < 0.001), but not with other adverse pathological features. The 90-day mortality rate was also higher in the overall R1 group (11.7%) compared with the groups with either overall R0 after primary DBD FS (7.5%) or overall R0 after DBD re-resection or additional PD (0%) (P = 0.013), although pairwise comparison between overall R1 and overall R0 after primary DBD FS was not significant (P = 0.051). Recurrence in general did not differ between all groups (P = 0.054). Local recurrence was more frequent in the overall R1 group compared with both overall R0 groups (P < 0.001). Adjuvant chemotherapy was administered more frequently in the overall R1 group (P < 0.001). Pathological outcomes following DBD FS varied across eras (P = 0.017).
Survival analysis
Overall R0 was achieved in 51.5% of the cohort. Median OS was longer in patients with overall R0 resections than in those with overall R1 resections (47.1 (95% confidence interval (c.i.) 26.6 to 99.9) versus 28.1 (14.5 to 67.8) months, respectively), with an adjusted HR of 1.83 (95% c.i. 1.44 to 2.32; P < 0.001) (Fig. S1).
Survival by DBD FS outcome is shown in Fig. 2. Median OS was 45.5 (26.1 to 87.2) months for overall R0 after primary DBD FS, 51.2 (31.2 to 80.4) months for overall R0 after DBD re-resection or additional PD, and 28.1 (14.5 to 67.8) months for overall R1. There was no survival difference between the two overall R0 groups (P = 0.706), but both had longer survival than the overall R1 group (P < 0.001 and P = 0.021, respectively). Among patients who survived beyond 90 days after surgery, survival remained comparable between the two overall R0 groups (P = 0.968) (File 2, Fig. S1). In contrast to overall R0 after primary DBD FS versus overall R1, no difference was observed between overall R0 after DBD re-resection or additional PD and overall R1 (P < 0.001 and P = 0.071, respectively). Such a relationship was not observed for DFS (Fig. S3). A separate analysis with HGD regarded as R1 is shown in Fig. S4.
Kaplan–Meier curve showing overall survival according to the outcome of DBD FS analysisPatients were grouped as overall R0 after primary DBD FS, overall R0 after DBD re-resection or additional PD, and overall R1. Pairwise comparisons: P = 0.706 (overall R0 after primary DBD FS versus overall R0 after DBD re-resection or PD); P < 0.001 (overall R0 after primary DBD FS versus overall R1); P = 0.021 (overall R0 after DBD re-resection or additional PD versus overall R1) (log rank test).
Survival for patients with a positive DBD FS is shown in Fig. 3. Median OS was 51.2 (31.2 to 80.4) months for overall R0 after DBD re-resection or PD, 23.3 (17.4 to not reached) months for overall R1 with DBD R0 by DBD re-resection or PD, and 27.5 (6.4 to 61.3) months for DBD R1 with or without re-resection. Survival was similar between the two R1 groups (P = 0.684), and both had worse survival compared with overall R0 after DBD re-resection or PD (P = 0.032 and P = 0.002, respectively).
Kaplan–Meier curve showing overall survival according to outcome of positive DBD frozen sectionPatients were grouped as overall R0 after DBD re-resection or PD, overall R1 with DBD R0 by re-resection or PD, and DBD R1 with or without re-resection. Pairwise comparisons: P = 0.002 (overall R0 after DBD re-resection or PD versus overall R1 after DBD re-resection or PD); P = 0.032 (overall R0 after DBD re-resection or PD versus overall R1); P = 0.684 (overall R1 after DBD re-resection or PD versus overall R1) (log rank test).
The results of univariable and multivariable Cox regression analyses for OS are shown in Table 3. Compared with overall R0 after primary DBD FS, overall R0 after DBD re-resection or additional PD was not associated with a difference in survival (adjusted HR 0.84, 0.49 to 1.44; P = 0.536). In contrast, overall R1 resection was independently associated with worse OS (adjusted HR 1.82, 1.43 to 2.33; P < 0.001). Other independent predictors of OS included carbohydrate antigen 19-9, lymph node metastasis, tumour size ≥ 30 mm, and adjuvant chemotherapy. Year of surgery was not associated with survival. A sensitivity analysis with censored 90-day mortality yielded similar results (Table S2).
In a stratified analysis, patients with overall R0 after DBD re-resection or additional PD had similar OS regardless of lymph node status. Median OS was 51.2 (27.0 to 69.5) months in the presence of lymph node metastasis compared with 55.2 (31.3 to 91.6) months in its absence (adjusted HR 0.90, 0.21 to 3.91; P = 0.896) (Fig. S5). No 90-day mortality was reported in this subgroup.
Morbidity and mortality
Eleven patients undergoing additional PD were younger (by 19 years) than those undergoing DBD re-resection or no intervention (P = 0.013) and had better ASA grades (P = 0.040). No difference in Clavien–Dindo grade ≥ IIIa complications was found between groups (P = 0.126). ISGLS B or C bile leaks occurred in 3 patients (28%) who had additional PD, 11 (22%) who underwent DBD re-resection, and 116 (21.7%) who had no intervention (P = 0.674). Intra-abdominal abscess requiring drainage was more frequent in patients undergoing additional PD than in any other group (P = 0.022). The 90-day mortality rate did not differ between groups (P = 0.121), with no deaths reported among patients who had additional PD, 7 (14%) in the DBD re-resection group, and 49 (9.1%) among those with no intervention (Table S3). In the adjusted post hoc analysis, DBD re-resection was still not associated with increased risk of complications with Clavien–Dindo grade ≥ IIIa, ISLGS B or C bile leak, intra-abdominal abscess, or 90-day mortality (adjusted odds ratio 0.76 (95% c.i. 0.40 to 1.42), 1.07 (0.48 to 2.22), 0.40 (0.15 to 0.90), and 1.49 (0.55 to 3.59), respectively).
Discussion
This was the first multicentre study to focus on intraoperative management of a positive DBD FS in pCCA^10^. Although only 45% of patients with a positive DBD FS achieved overall R0 status after DBD re-resection or additional PD, survival was better in these selected patients, irrespective of lymph node status. Morbidity and mortality did not differ between the groups.
Although DBD FS analysis was associated with conversion to overall R0 in a substantial subset of patients, its oncological impact appeared limited when considered in a broader clinical context. Technically, DBD resections can be extended more easily than PBD procedures following a positive FS. Yet, the present findings still align with those of Nooijen et al.^7^, who reported only a 5% increase in overall R0 rates following routine PBD FS analysis.
In this study, the overall R0 conversion rate was partly constrained by omitting any extended DBD resection in 27 of 73 patients with positive DBD margins. Concurrent involvement of the PBD margin and/or RM was also present in 35 of 73 patients. The risk of false-negative PBD FS has been well documented^7,34^ and invasive carcinoma at the RM dissection plane is often only detected on final pathology^27^. Furthermore, contrary to previous suggestions by Otsuka et al.^10,35^, intraoperative clearance of a positive DBD margin did not improve survival in patients with PBD or RM tumour spread (Fig. 3). These observations suggest that DBD re-resection or additional PD for a positive DBD margin should be carefully weighed in patients with suspected radial rather than longitudinal tumour growth. An alternative approach to improving patient selection could involve performing an upfront resection of the DBD deep into the pancreatic head, then waiting for the final pathology results before discussing the potential benefits and risks of an additional PD if necessary. Recent single-centre cohort studies^24–27,36,37^ from Eastern and Western institutions have also suggested individual association between a positive PBD margin or RM and survival. Thus, further research with larger cohorts is needed to determine whether a positive DBD margin also independently predicts worse oncological outcomes.
Given the large number of patients undergoing DBD FS analysis to determine eligibility for DBD re-resection or additional PD, it was crucial to determine whether these interventions conferred a meaningful survival advantage. The survival curve revealed that patients who achieved overall R0 after DBD re-resection or additional PD had comparable OS to those with overall R0 at primary DBD FS (Fig. 2). Conversely, patients with overall R1 status, irrespective of DBD re-resection or additional PD, experienced worse outcomes. These findings were verified by the multivariable analysis (Table 3), which revealed the independent prognostic value of achieving overall R0 following a positive DBD FS, even after adjusting for 90-day survival. Despite the well established prognostic role of lymph node metastasis^1,8,12,14,20,24–26,31,32^, overall R0 following DBD re-resection or additional PD was associated with similar survival irrespective of lymph node involvement. This should be interpreted with caution as the small sample size limited the power to exclude a clinically relevant effect.
In contrast to the present study, Otsuka et al.^10^ and Zhang et al.^11^ included patients with Bismuth–Corlette type I or II tumours treated with EHBD resection without major hepatectomy, likely contributing to the more favourable 90-day mortality and long-term outcomes. The overall R1 subgroup frequently included patients with Bismuth–Corlette type IIIa or IV tumours with larger lesion size and advanced T category, often necessitating complex right hepatectomies associated with greater operative risk and worse long-term prognosis^38^. Despite this, there was no difference in 90-day mortality between groups, and no early survival disparity appeared to drive any initial divergence between the survival curves. This discrepancy may reflect differences in tumour biology, patient selection, preoperative treatment, technical complexity or surgical strategies between Eastern and Western populations, as noted by Olthof et al.^1^ and Jansson et al.^2^. Nevertheless, a type II error cannot be ruled out owing to the limited sample size.
To evaluate the safety of extended resections, surgical morbidity and mortality were analysed. Patients who had DBD re-resection experienced rates of major surgical complications, bile leakage, and abscess formation similar to those of patients who did not undergo DBD re-resection, indicating that this procedure is generally safe. These results support the upfront use of the technique extending the DBD resection into the pancreatic head. Furthermore, additional PD was performed in younger patients with more favourable ASA grades and was not associated with 90-day mortality. Although Western series have previously reported high mortality rates following additional PD compared with Eastern cohorts^10,12,13,39^, this study emphasizes that the procedure may still be feasible in highly selected young and non-frail patients. However, broadening the indication to less selected populations may increase morbidity and mortality, and is unlikely to be justified in the absence of proven benefit.
This study had several limitations, including its retrospective design, variations in indications for adjuvant chemotherapy, and missing data on neoadjuvant therapy. The small sample size, together with the decision to perform DBD re-resection or additional PD at the operating surgeon’s discretion, introduced potential selection bias related to the identification of suitable candidates. A key limitation was potential interinstitutional heterogeneity in FS technique and margin reporting inherent to a retrospective multicentre design. This was mitigated by limiting participating centres to high-volume HPB centres, applying uniform ICCR definitions for margin status, and use of a standardized data file to register clearance of the margin site. Moreover, era-related variations in DBD FS outcomes did not independently affect survival after adjustment for co-variables. Nevertheless, a central pathology re-review was not undertaken, and variation in sampling or interpretation—particularly for HGD and subtle ductal changes—may persist. Although HGD was prespecified as negative, with comparable results in the sensitivity analysis that treated HGD as positive (Fig. S4), its prognostic significance remains uncertain and requires prospective validation, particularly given the small number of patients with HGD at the DBD margin (4 patients). The higher overall R0 rate after DBD re-resection or PD may reflect baseline differences, as these patients less commonly had Bismuth type IV tumours, and were more likely to have lower T categories and smaller tumours, consistent with more favourable biology. In addition, overall R0 status was more frequently achieved after right-sided resections, which are known to improve clearance of the PBD margin. These results suggest that underlying tumour biology combined with surgical strategy may have contributed to achieving overall R0 following DBD re-resection or PD. Therefore, a causal relationship between the technical achievement of overall R0 resection and improved prognosis cannot be established in this study. Additionally, the higher 90-day mortality rate in the overall R1 group (11.7%) may also reflect suboptimal selection in combination with frailty or co-morbidity, suggesting that resections were futile in a subset of patients. Another limitation is that indications and regimens for adjuvant chemotherapy varied between centres and over time, and patients who had overall R1 resections were more likely to have received treatment, introducing potential confounding. Although a randomized clinical trial would overcome these limitations, such a study is not feasible owing to the rarity of positive DBD FS in pCCA. Nevertheless, this remains the largest multicentre study providing real-world data reflecting clinical practice.
The present findings have indicated that extended DBD resection to achieve overall R0 status is associated with improved prognosis in selected patients, including those with lymph node metastasis. This strategy has a low risk of major complications following DBD re-resection, suggesting that routine extension of the resection into the pancreatic head may be performed safely—without the need for prior DBD FS—to optimize the likelihood of achieving negative margins. Additional PD proved safe when applied highly selectively.
Supplementary Material
zrag010_Supplementary_Data
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Olthof PB, Miyasaka M, Koerkamp BG, Wiggers JK, Jarnagin WR, Noji T et al A comparison of treatment and outcomes of perihilar cholangiocarcinoma between Eastern and Western centers. HPB 2019;21:345–35130087051 10.1016/j.hpb.2018.07.014PMC 7534176 · doi ↗ · pubmed ↗
- 2Jansson H, Oba A, Maekawa A, Villard C, Kobayashi K, Ono Y et al Western and Eastern experience in treating perihilar cholangiocarcinoma: retrospective bi-centre study. BJS Open 2025;9:zraf 01940200911 10.1093/bjsopen/zraf 019PMC 11979329 · doi ↗ · pubmed ↗
- 3Mueller M, Breuer E, Mizuno T, Bartsch F, Ratti F, Benzing C et al Perihilar cholangiocarcinoma—novel benchmark values for surgical and oncological outcomes from 24 expert centers. Ann Surg 2021;274:780–78834334638 10.1097/SLA.0000000000005103 · doi ↗ · pubmed ↗
- 4Rassam F, Roos E, van Lienden KP, van Hooft JE, Klümpen HJ, van Tienhoven G et al Modern work-up and extended resection in perihilar cholangiocarcinoma: the AMC experience. Langenbecks Arch Surg 2018;403:289–30729350267 10.1007/s 00423-018-1649-2PMC 5986829 · doi ↗ · pubmed ↗
- 5Sturesson C, Soreide K. Preoperative management and resectability criteria in perihilar cholangiocarcinoma. Br J Surg 2025;112:znae 32940212003 10.1093/bjs/znae 329 · doi ↗ · pubmed ↗
- 6Nagino M, De Matteo R, Lang H, Cherqui D, Malago M, Kawakatsu S et al Proposal of a new comprehensive notation for hepatectomy. Ann Surg 2021;274:1–333630445 10.1097/SLA.0000000000004808 · doi ↗ · pubmed ↗
- 7Nooijen LE, Franken LC, de Boer MT, Buttner S, van Dieren S, Koerkamp BG et al Value of routine intraoperative frozen sections of proximal bile duct margins in perihilar cholangiocarcinoma, a retrospective multicenter and matched case-control study. Eur J Surg Oncol 2022;48:2424–243135729016 10.1016/j.ejso.2022.06.011 · doi ↗ · pubmed ↗
- 8Endo I, House MG, Klimstra DS, Gönen M, D’Angelica M, De Matteo RP et al Clinical significance of intraoperative bile duct margin assessment for hilar cholangiocarcinoma. Ann Surg Oncol 2008;15:2104–211218543039 10.1245/s 10434-008-0003-2 · doi ↗ · pubmed ↗