ECG challenge: unexpected shift in QRS morphology
Pietro Redigolo, Paolo Zappulla, Davide Capodanno

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
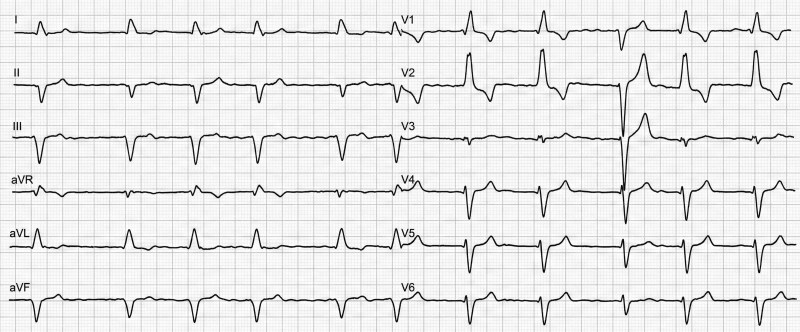 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCardiac electrophysiology and arrhythmias · ECG Monitoring and Analysis · Cardiac Arrhythmias and Treatments
An 84-year-old male with a history of hypertension, type 2 diabetes mellitus, dyslipidaemia, atrial fibrillation and chronic kidney disease, first experienced the onset of exertional dyspnoea accompanied by palpitations in February 2025. Due to the persistence of these symptoms, a comprehensive diagnostic workup was performed in June 2025, revealing heart failure with reduced ejection fraction (HFrEF) of non-ischemic origin, as confirmed by the absence of obstructive coronary artery disease on invasive coronary angiography. Following the diagnosis, the patient was started on guideline-directed medical therapy (GDMT).
Despite 3 months of such management, a follow-up echocardiogram showed persistent systolic impairment with a left ventricular ejection fraction (LVEF) of 35%. Given the lack of substantial recovery and the risk of sudden cardiac death, the patient met the criteria for primary prevention. Consequently, he was admitted in January 2026 for elective implantation of an implantable cardioverter-defibrillator (ICD).
A pre-procedural ECG showed atrial fibrillation with a complete right bundle branch block (RBBB) pattern. During the routine post-procedural clinical monitoring in the inpatient ward, a 12-lead ECG was performed, capturing a spontaneous transition between RBBB and left bundle branch block (LBBB) morphologies within the same recording (Figure 1).
Question 1: What is the most likely diagnosis for the rhythm transition seen in Figure 1?
Rate-dependent Ashman phenomenon.Alternating Bundle Branch Block (ABBB).Intermittent ventricular pacing.Intermittent pre-excitation.
Correct Answer: B
Discussion and explanation
The transition seen in Figure 1 is diagnostic of ABBB, defined as spontaneous alternation between RBBB and LBBB morphologies in the same patient. Unlike rate-dependent aberrancy (Ashman phenomenon), the alternation occurs without a consistent long-short RR sequence. Moreover, no pacing artefacts or pacing-related QRS morphology are evident, excluding intermittent ventricular pacing.
ABBB reflects advanced conduction system disease involving both bundle branches, indicating severe and unstable infra-Hisian conduction. This pattern is widely recognized as a marker of impending complete atrioventricular (AV) block rather than a functional or benign conduction abnormality.^1^
Question 2: What is the primary clinical implication of this ECG finding?
It represents a benign variant of intraventricular conduction delay.It suggests lead dislodgement or micro-dislodgement after ICD implantation.It indicates an imminent risk of progression to complete (third-degree) atrioventricular block.It is a pathognomonic sign of acute myocardial ischaemia in the septal area.
Correct Answer: C
Discussion and explanation
From a clinical standpoint, recognition of ABBB is crucial, as it is associated with a high and unpredictable risk of progression to complete AV block and ventricular standstill, even in asymptomatic patients. Both European and American guidelines consider ABBB a Class I indication for permanent pacing, owing to the advanced infra-Hisian nature of the conduction disease.^2,3^
In this specific case, the recently implanted ICD already provides the necessary backup pacing; although no immediate device upgrade is required, the presence of ABBB underscores the need for careful follow-up, as it may precede future pacing dependency or the development of conduction patterns relevant to resynchronization strategies.^2,3^
Question 3: What is the most likely anatomical site of the conduction delay in a patient exhibiting alternating bundle branch block?
Proximal AV node.Intranodal AV node.Infra-Hisian conduction system.Left posterior fascicle with compensatory right-sided delay.
Correct Answer: C
Discussion and explanation
Alternating bundle branch block is a hallmark of advanced infra-Hisian conduction system disease, typically involving bilateral bundle branch pathology. Unlike AV nodal disease, which often manifests as Mobitz I AV block, ABBB reflects severe conduction instability distal to the His bundle, with unpredictable propagation through the His–Purkinje system. Electrophysiological studies in such patients frequently demonstrate markedly prolonged HV intervals and confirm a high likelihood of progression to complete AV block or ventricular standstill.^1^
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Surawicz B, Childers R, Deal BJ, Gettes LS. AHA/ACCF/HRS recommendations for the standardization and interpretation of the electrocardiogram: part III: intraventricular conduction disturbances: a scientific statement from the American Heart Association electrocardiography and arrhythmias committee, council on clinical cardiology; the American College of Cardiology foundation; and the heart rhythm society. Endorsed by the international society for computerized electrocardiology. J Am Coll Car · doi ↗ · pubmed ↗
- 2Glikson M, Nielsen JC, Kronborg MB, Michowitz Y, Auricchio A, Barbash IM, et al 2021 ESC guidelines on cardiac pacing and cardiac resynchronization therapy. Eur Heart J 2021;42:3427–3520.34455430 10.1093/eurheartj/ehab 364 · doi ↗ · pubmed ↗
- 3Kusumoto FM, Schoenfeld MH, Barrett C, Edgerton JR, Ellenbogen KA, Gold MR, et al 2018 ACC/AHA/HRS guideline on the evaluation and management of patients with bradycardia and cardiac conduction delay: a report of the American College of Cardiology/American Heart Association task force on clinical practice guidelines and the heart rhythm society. Circulation 2019;140:e 382–e 482.30586772 10.1161/CIR.0000000000000628 · doi ↗ · pubmed ↗