Whispers of decay: necrotic mediastinal lymphadenopathy due to melioidosis in a diabetic patient
Rathan Kamath, Nitin Gupta, Anirudh Venkatesh, Muralidhar Varma, Praveen Kumar Tirlangi

TL;DR
A diabetic man with poorly controlled diabetes developed a rare case of melioidosis that mimicked tuberculosis, highlighting the need for early diagnosis in similar cases.
Contribution
This paper presents a rare clinical case of melioidosis manifesting as necrotic mediastinal lymphadenopathy in a diabetic patient.
Findings
Melioidosis can present as necrotic mediastinal lymphadenopathy, mimicking tuberculosis.
Diabetes and poor glycemic control may increase susceptibility to such presentations of melioidosis.
Dual microbiological confirmation via sputum culture and EBUS-guided aspiration is effective for diagnosis.
Abstract
We report a case of melioidosis presenting as isolated necrotic mediastinal lymphadenopathy in a 60-year-old man from coastal Karnataka with poorly controlled diabetes (HbA1c 9.9%). Such a presentation, closely mimicking tuberculosis, is rarely described in the literature. Dual microbiological confirmation through sputum culture and endobronchial ultrasound (EBUS) guided lymph node aspiration established the diagnosis of Burkholderia pseudomallei. This case underscores the importance of considering melioidosis in the differential diagnosis of necrotic mediastinal lymphadenopathy, particularly in endemic regions and in diabetic patients. Early recognition and appropriate therapy remain crucial to prevent complications and improve outcomes in this potentially fatal but treatable infection.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
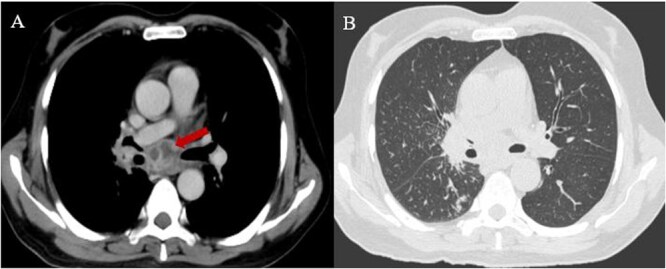 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsBurkholderia infections and melioidosis · Research on Leishmaniasis Studies · Galectins and Cancer Biology
Case
A 60-year-old resident of coastal Karnataka, with poorly controlled diabetes (Glycosylated haemoglobin-9.9%), presented with a 25-day history of fever, chills, and a cough with minimal expectoration. He denied haemoptysis, chest pain, or shortness of breath. Initial investigations revealed mild anaemia (haemoglobin 11.9 g/dl), neutrophilic leucocytosis (total leukocyte count 19 400 cells/mm^3^ with 81% neutrophils), and elevated C-reactive protein (142.7 mg/dl). Liver and renal function tests were routine. Blood cultures were sterile, and no vegetation was detected on two-dimensional echocardiography. A contrast-enhanced chest computed tomography (CT) revealed multiple large necrotic mediastinal lymph nodes and centrilobular nodules in the superior segment of the right lower lobe (Fig. 1). With a suspicion of tuberculosis, sputum samples were sent for acid-fast staining, GeneXpert Ultra, and mycobacterial culture, all of which were negative. A sputum sample was sent for bacterial culture, which grew Burkholderia pseudomallei. Subsequent endobronchial ultrasound (EBUS)-guided aspiration of mediastinal lymph nodes was also positive for the same organism. The patient was started on intravenous meropenem (1 gram three times a day), with subsequent resolution of his fever within 8 days. Meropenem was continued for 14 days and then switched to oral co-trimoxazole (800/160, two tablets twice a day, for 4 months) for the continuation phase of treatment.
Multiple large necrotic mediastinal lymph nodes (A), along with centrilobular nodules in the superior segment of the right lower lobe (B).
Discussion
Melioidosis, a potentially fatal infection caused by B. pseudomallei, is primarily endemic in tropical regions of Southeast Asia, Northern Australia, and India [1, 2]. Clinical presentations vary widely, ranging from fulminant septic shock to a more indolent, chronic disease characterised by abscesses in multiple organs [3]. This broad spectrum often leads to diagnostic delays, particularly when the disease presents with atypical features such as isolated necrotic mediastinal lymphadenopathy.
Importantly, melioidosis can closely mimic tuberculosis both clinically and radiologically, contributing to frequent misdiagnosis in endemic regions. B. pseudomallei can induce granulomatous inflammation and, in some instances, caseous necrosis, reproducing the hallmark histopathological features of tuberculous lymphadenitis [4, 5]. Clinically, both diseases may present with prolonged fever, weight loss, cough, mediastinal lymphadenopathy, and pulmonary nodularity. Radiologically, features such as necrotic lymph nodes, tree-in-bud nodules, and patchy infiltrates can be indistinguishable between the two conditions [6, 7]. Additionally, diabetes one of the strongest risk factors for melioidosis is also a known risk factor for tuberculosis, further increasing diagnostic complexity in regions where both pathogens are endemic.
Another important consideration is that tuberculosis and melioidosis rarely can co-infect the same patient, particularly in individuals with impaired immunity such as those with diabetes [8–10]. Co-infection may also influence the clinical course, complicate radiological interpretation, and impact therapeutic decisions. Therefore, establishing a clear microbiological diagnosis becomes crucial in avoiding inappropriate monotherapy, which could worsen outcomes if the second pathogen is not recognised.
In our case, the diagnosis of melioidosis was supported by dual microbiological confirmation from two independent sites sputum culture and EBUS-guided lymph node aspiration [11]. Confirming the organism from both a respiratory sample and the involved lymph nodes provided robust evidence against tuberculosis and ruled out the possibility of a coincidental colonisation or contamination. This multi-site confirmation is particularly important in TB-endemic regions, where reliance on imaging alone can be misleading and where co-infection remains a real possibility. Obtaining microbiological evidence from more than one site therefore strengthens diagnostic certainty and ensures timely initiation of appropriate therapy.
Though lymphadenitis can occasionally be observed in melioidosis, necrotic mediastinal lymphadenopathy as the predominant or sole presenting feature remains exceptionally rare in the literature [12–14]. In tuberculosis-endemic settings, this often leads clinicians to prioritise TB, potentially delaying targeted therapy for melioidosis. This case highlights the need for systematic microbiological evaluation including cultures and tissue sampling rather than assuming tuberculosis based on radiological pattern alone.
Treatment typically involves two to eight weeks of intravenous antibiotics (e.g. meropenem or ceftazidime), followed by an extended eradication phase of at least 3–4 months with oral co-trimoxazole [15]. Adherence to this prolonged regimen is essential to prevent relapse, a known complication when therapy is incomplete.
In conclusion, melioidosis though uncommon should be strongly considered in individuals from endemic regions who present with unexplained fever and necrotic mediastinal lymphadenopathy, particularly in those with diabetes. Its clinical and radiological resemblance to tuberculosis, along with the possibility of co-infection, underscores the need for definitive microbiological confirmation. Early recognition and appropriate therapy remain crucial to improving outcomes in this potentially fatal but treatable infection.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Currie BJ, Dance DAB, Cheng AC. The global distribution of Burkholderia pseudomallei and melioidosis: an update. Trans R Soc Trop Med Hyg 2008;102 Suppl 1:S 1–4. 10.1016/S 0035-9203(08)70002-619121666 · doi ↗ · pubmed ↗
- 2Dance DA . Melioidosis as an emerging global problem. Acta Trop 2000;74:115–9. 10.1016/S 0001-706X(99)00059-510674638 · doi ↗ · pubmed ↗
- 3Nisarg S, Tirlangi PK, Ravindra P. et al. Predictors of 28-day mortality in melioidosis patients presenting to an emergency department: a retrospective cohort study from South India. Trans R Soc Trop Med Hyg 2024;118:652–8. 10.1093/trstmh/trae 01738554065 · doi ↗ · pubmed ↗
- 4Sriwijitalai W, Wiwanitkit V. Concurrent melioidosis and tuberculosis: an expected incidence in endemic tropical country. Int J Mycobacteriology 2019;8:412.10.4103/ijmy.ijmy_148_1931793517 · doi ↗ · pubmed ↗
- 5Jamani NA, Mohd Nor FH, Yatim Y. It is tuberculosis or melioidosis? A clinical diagnostic dilemma. Med J Malaysia 2021;76:734–6.34508384 · pubmed ↗
- 6Kottarathil M, Reju S, Barani R. et al. Are we dealing with melioidosis under the mask of tuberculosis? - a case series. Indian J Tuberc 2024;71:99–104. 10.1016/j.ijtb.2023.06.01438296398 · doi ↗ · pubmed ↗
- 7Lam NH, Huyen DT, Hoa L. et al. Cavitary lung disease in hospitalized patients: differences between melioidosis and tuberculosis. Trop Dr 2022;52:427–30. 10.1177/0049475522109571135440256 · doi ↗ · pubmed ↗
- 8Jain M, Ratna HVK, Mohanty S. et al. Coinfection of melioidosis and tuberculosis causing infective lumbar spondylodiscitis: a rare case report. JBJS Case Connect 2023;13:e 00770. 10.2106/JBJS.CC.22.0077037172118 · doi ↗ · pubmed ↗