Peri-Umbilicated Pseudopustules in Mpox
Nitin Gupta, Shantala GB, Rima Sahay, Kumar Singh, Pothumarthy Venkata Swathikiran, Muralidhar Varma, Tirlangi Praveen Kumar

TL;DR
This paper describes a case of mpox in a man with unique skin lesions, highlighting how the disease can be diagnosed and distinguished from other similar conditions.
Contribution
The paper presents a distinctive clinical case of mpox with peri-umbilicated pseudopustules, emphasizing their diagnostic significance.
Findings
The patient exhibited fever, sore throat, and a genital ulcer followed by distinctive pseudopustular skin lesions.
Mpox was confirmed via PCR testing of throat and skin swabs.
The pseudopustular morphology is a key diagnostic feature distinguishing mpox from other eruptions.
Abstract
Mpox is an emerging zoonotic infection that has shown sustained human-to-human transmission since 2022, often through sexual contact networks. We report a case of mpox in a 43-year-old Indian-origin man residing in the United Arab Emirates who presented with fever, sore throat, and a painful genital ulcer, followed by widespread vesiculo-pseudopustular lesions. Examination revealed firm, well-circumscribed, peri-umbilicated pseudopustules, distinctive lesions lacking purulent content. Laboratory investigations were unremarkable, and a polymerase chain reaction test for the Monkeypox virus, conducted on throat and skin swabs, confirmed the diagnosis. The patient was managed with supportive care and recovered uneventfully. This case highlights the characteristic pseudopustular morphology of mpox, which serves as a key diagnostic clue distinguishing it from other genital and vesicular…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
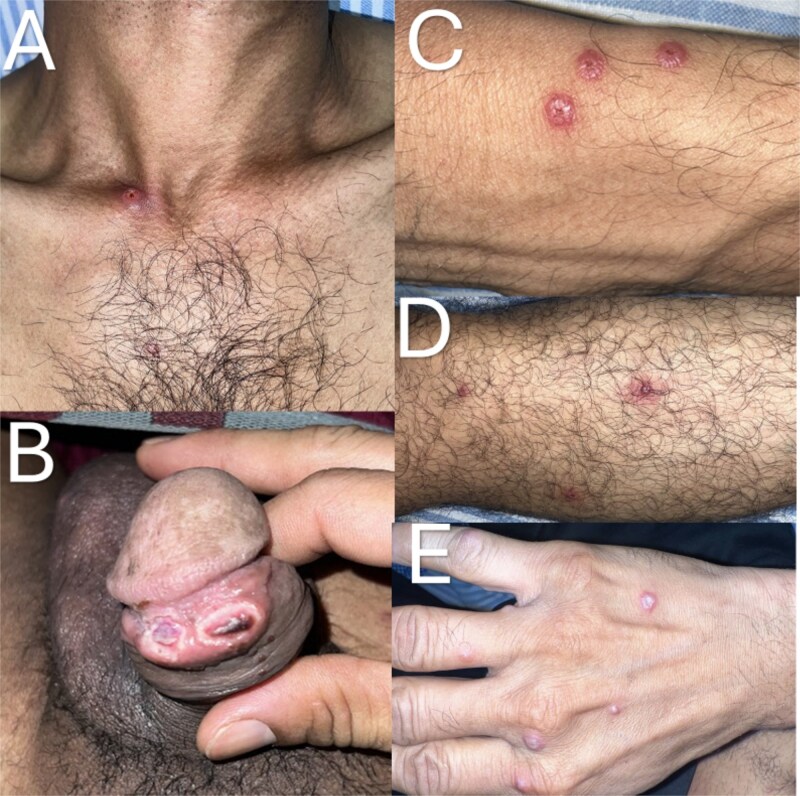 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPoxvirus research and outbreaks · Virology and Viral Diseases · Bacillus and Francisella bacterial research
Introduction
Mpox (formerly known as monkeypox) is an emerging zoonotic infection caused by the Monkeypox virus, an orthopoxvirus closely related to variola and vaccinia viruses [1]. Historically confined to Central and West Africa, mpox has re-emerged since 2022 with sustained human-to-human transmission across multiple continents, particularly affecting sexual networks of men who have sex with men (MSM) [1, 2]. This represents a major epidemiological shift from its earlier sporadic, zoonotically transmitted form [1]. Clinically, mpox is characterized by fever, lymphadenopathy, and a vesiculo-pustular rash that progresses synchronously [3]. However, recent outbreaks have revealed atypical manifestations, including localized genital ulcers, peri-anal lesions, and mucosal involvement that may mimic other sexually transmitted infections [3]. Here, we describe a case of laboratory-confirmed mpox in an Indian-origin male residing in the United Arab Emirates (UAE), highlighting the characteristic morphology of pseudopustular lesions, which serve as a key diagnostic clue distinguishing mpox from other vesicopustular dermatoses.
Case report
A 43-year-old Indian-origin man residing in the UAE presented with a 5-day history of fever, sore throat, and a painful genital ulcer. The patient denied being a man who has sex with men, but reported close contact with another individual who later tested positive for mpox. Over the subsequent days, he developed multiple vesiculo-pseudopustular lesions, initially localized to the genital area and later spreading to the trunk and extremities.
On admission, the patient was febrile (38.5°C) but hemodynamically stable. Physical examination revealed oral and genital ulcers, a maculopapular rash over the trunk, and numerous firm, well-circumscribed, peri-umbilicated pseudopustular lesions on the extremities (Fig. 1). These lesions lacked true purulent material, distinguishing them from typical pustules. Bilateral axillary and inguinal lymphadenopathy were palpable and mildly tender.
Characteristic pseudopustular lesions in mpox. (A) Ulcerated nodule over the upper chest. (B) Umbilicated erosions and ulcers on the glans penis and prepuce. (C–E) well-circumscribed, firm, peri-umbilicated pseudopustules with central crusting on the forearm (C), leg (D), and dorsum of the hand (E).
Laboratory investigations revealed a normal complete blood count and mild elevation of transaminases. Serologic tests for HIV, syphilis, hepatitis B, and hepatitis C were negative. Bacterial cultures from blood and lesion swabs yielded no growth. Given the epidemiological exposure and characteristic lesion morphology, mpox was suspected. Swabs from the throat and skin lesions were sent for PCR testing for the Monkeypox virus, which returned a positive result, confirming the diagnosis.
The patient was managed with supportive therapy, including antipyretics, topical antiseptics, and hydration, along with strict isolation precautions. No antiviral therapy (tecovirimat or brincidofovir) was administered, as the illness was self-limiting. Over the course of two weeks, the lesions crusted and resolved without scarring. The patient remained clinically stable and was discharged upon resolution of symptoms and completion of the isolation period.
Discussion
The re-emergence of mpox in non-endemic regions underscores a paradigm shift in its transmission dynamics, from sporadic zoonotic spillover to sustained human-to-human transmission [1]. The predominant Clade IIb virus circulating globally since 2022 has demonstrated efficient transmission through close physical and sexual contact, particularly within interconnected sexual networks [4, 5]. This shift has led to changes not only in the epidemiology of the disease but also in its clinical spectrum and pattern of presentation.
Traditionally, mpox lesions evolve sequentially from macules to papules, vesicles, pustules, and crusts [3]. However, recent outbreaks have revealed considerable morphological variability. The hallmark finding in this case was the presence of pseudopustules, firm, umbilicated lesions that lack true purulent content, reflecting dermal edema and necrosis rather than suppuration [3]. Recognition of this morphology is critical, as it helps distinguish mpox from other vesiculo-pustular dermatoses [6]. Herpes simplex virus typically presents with grouped, fluid-filled vesicles on an erythematous base that rapidly ulcerate, whereas varicella-zoster virus produces pleomorphic lesions that evolve asynchronously [6]. Molluscum contagiosum, on the other hand, presents as smaller umbilicated papules with central keratin plugs and minimal inflammation [6]. In sexually active individuals, genital ulcers caused by herpes simplex virus, syphilis, or chancroid can further complicate the clinical picture [6]. Therefore, integrating lesion morphology with epidemiological context, such as recent exposure to a confirmed case or travel to an endemic area, remains key for timely clinical suspicion and diagnosis.
While specific antivirals such as tecovirimat showed promise initially, a subsequent randomised controlled trial has shown that it was ineffective in reducing the number of days to lesion resolution [7]. Early recognition, isolation, and appropriate infection control measures are essential to interrupt transmission. This case reinforces the importance of clinician awareness of the atypical and evolving presentations of mpox, especially the distinctive pseudopustular morphology, which can serve as an early diagnostic clue before confirmatory molecular testing is available.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Wu S, Deng J, Du M. et al. Global transmission characteristics of mpox outbreaks: a systematic review and meta-analysis. e Clinical Medicine. 2025;89:103526.41079025 10.1016/j.eclinm.2025.103526 PMC 12508583 · doi ↗ · pubmed ↗
- 2Alshamrani MM, El-Saed A, Al-Fayez S. et al. Routes of transmission of mpox by virus clade and geographic distribution: a systematic review. J Infect Public Health 2025;18:102985. 10.1016/j.jiph.2025.10298541092779 PMC 12596201 · doi ↗ · pubmed ↗
- 3Maronese CA, Avallone G, Aromolo IF. et al. Mpox: an updated review of dermatological manifestations in the current outbreak. Br J Dermatol 2023;189:260–70. 10.1093/bjd/ljad 15137146166 · doi ↗ · pubmed ↗
- 4Callaby H, Belfield A, Otter AD. et al. Mpox: current knowledge and understanding-a scoping review. FEMS Microbiol Rev 2025;49:fuaf 025. 10.1093/femsre/fuaf 02540489313 PMC 12198961 · doi ↗ · pubmed ↗
- 5Srivastava S, Sharma D, Sridhar SB. et al. Comparative analysis of Mpox clades: epidemiology, transmission dynamics, and detection strategies. BMC Infect Dis 2025;25:1290. 10.1186/s 12879-025-11784-841083957 PMC 12516921 · doi ↗ · pubmed ↗
- 6Al-Dabbagh J, Mohammad Deeb E, Younis R. et al. The dermatological manifestations and differential diagnosis of monkeypox: a narrative review. Medicine (Baltimore) 2024;103:e 40359. 10.1097/MD.000000000004035939496026 PMC 11537653 · doi ↗ · pubmed ↗
- 7PALM 007 Writing Group, Ali R, Alonga J. et al. Tecovirimat for clade I MPXV infection in the Democratic Republic of Congo. N Engl J Med 2025;392:1484–96.40239067 10.1056/NEJ Moa 2412439 PMC 12158442 · doi ↗ · pubmed ↗