Atypical lung carcinoid with prominent mucinous stroma: unusual pathologic finding in pulmonary carcinoid
Ghaida S AlSugair, Wajd A Althakfi

TL;DR
A rare lung tumor case with mucin-rich features is described, highlighting the importance of recognizing this variant to avoid misdiagnosis.
Contribution
The paper presents a unique case of atypical lung carcinoid with prominent mucinous stroma, emphasizing its diagnostic challenges.
Findings
A 34-year-old female was diagnosed with an atypical carcinoid featuring a prominent mucinous stroma.
The tumor exhibited organoid, trabecular, and pseudopapillary histologic patterns with positive immunohistochemical markers.
The case underscores the need for careful evaluation to distinguish this variant from other mucin-producing lung tumors.
Abstract
Background: Atypical carcinoids (ACs) are uncommon neuroendocrine tumors of the lung, and the presence of a prominent mucinous stroma is an exceptionally rare feature that may complicate diagnosis. Highlighting such variants is important for avoiding misclassification with mucin-producing pulmonary tumors. Case Presentation: A 34-year-old nonsmoking female presented with mild chest pain, minimal cough, and night sweats. Imaging revealed a well-circumscribed right middle-lobe lesion measuring 4.1 cm, and bronchoscopy showed a white-tan, fleshy mass filling the bronchial lumen. Pathology Findings: Histologic examination demonstrated a well-defined neoplasm with organoid, trabecular, follicular, pseudopapillary, and solid patterns and striking mucinous stromal change. Immunohistochemical staining was positive for CK AE1/AE3, synaptophysin (diffuse), chromogranin (diffuse), and TTF1, and…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
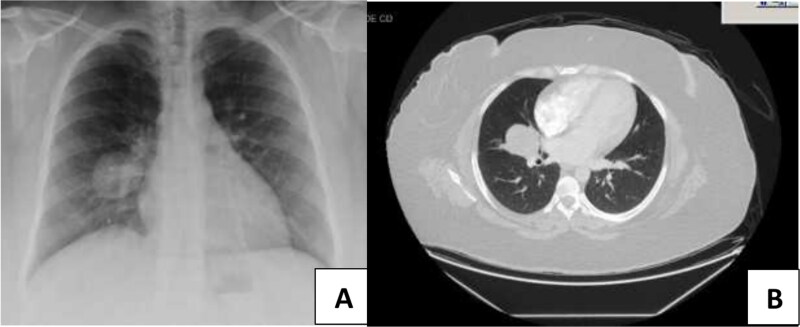 Figure 1
Figure 1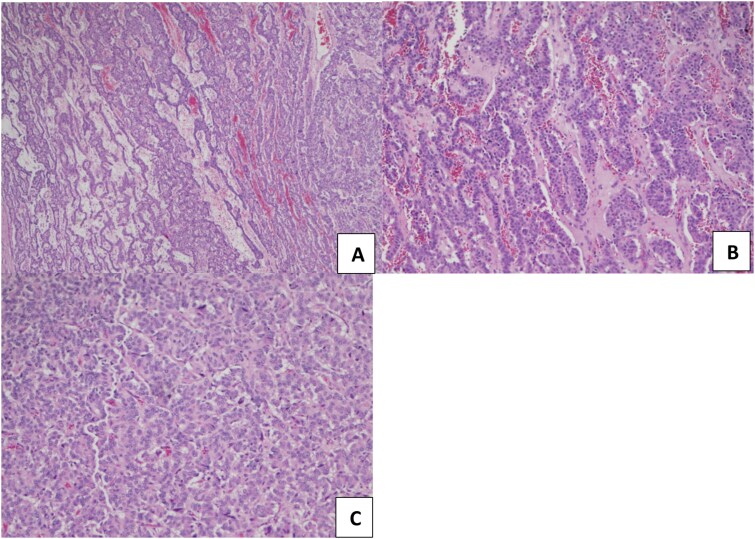 Figure 2
Figure 2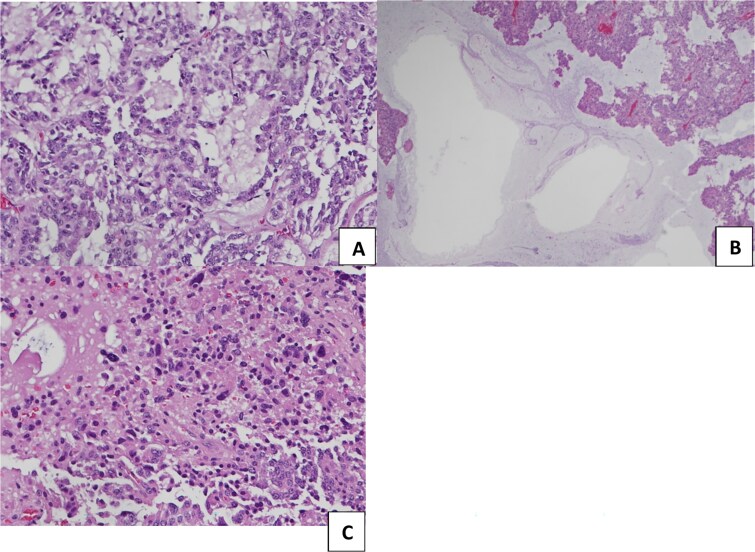 Figure 3
Figure 3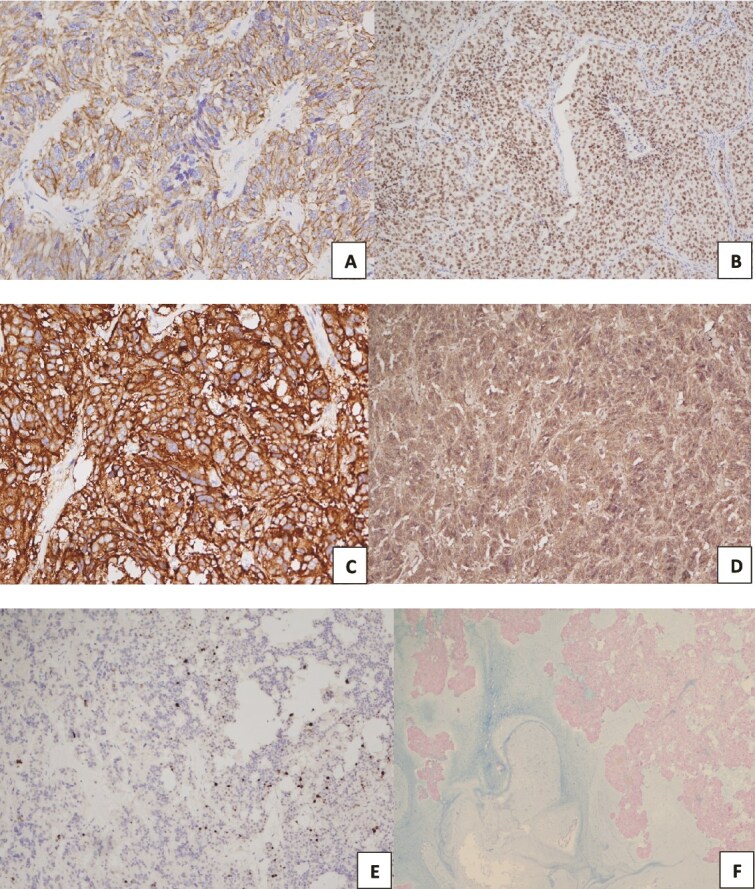 Figure 4
Figure 4| Marker | Result | Notes |
|---|---|---|
| CK AE1/AE3 | Positive | — |
| Synaptophysin | Positive | Diffuse |
| Chromogranin | Positive | Diffuse |
| TTF-1 | Positive | — |
| CK7 | Negative | — |
| CK20 | Negative | — |
| CDX2 | Negative | — |
| Ki-67 | ~10% | Proliferation index |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsNeuroendocrine Tumor Research Advances · Medical Imaging and Pathology Studies · Thyroid Cancer Diagnosis and Treatment
Introduction
Carcinoid tumors of the lung account for about 2% of all lung cancers (ratio of typical to atypical is 10:1), arising from the enterochromaffin cells lining the aerodigestive tract [1]. They are divided into two types: typical carcinoid tumors and atypical carcinoid tumors, which are low- and intermediate-grade neuroendocrine tumors, respectively. Approximately 80% of pulmonary carcinoids arise centrally, while 20% arise peripherally. According to the Thoracic WHO classification 5th edition [1], pulmonary carcinoids are classified as typical or atypical based on the number of mitotic figures per 2 mm^2^ and the presence of necrosis. 1 Typical carcinoids have fewer than 2/2 mm^2^ mitoses and are without necrosis, while ACs have 2-10/2 mm^2^ mitoses and/or necrosis and have focal, punctate, or comedo-like morphology [1].
However, both carcinoid subtypes can have a broad array of histological patterns, including organoid, trabecular, palisading, papillary, pseudo-glandular, rosette-like, spindle, and follicular growth. Classically, the stroma of carcinoids is richly vascularized and can exhibit hyalinization, bone formation, or cartilage formation. In the literature, cases of stromal amyloid and a prominent mucinous stroma have been reported [2].
Having such a heterogeneous morphology, carcinoid tumors can be muddled with other primary and metastatic tumors and require careful morphological and immunohistochemical analysis for differential diagnosis [1].
Here, we present a rarely reported case of AC with a protuberant mucinous stroma. We also performed a detailed histopathologic and immunohistochemical examination to rule out other primary and metastatic mucin-rich tumors.
Case report
A 34-year-old nonsmoker female with a nonremarkable previous medical history presented with mild chest pain, minimal cough, and night sweats. There was no history of lung or gastrointestinal cancer in her family. The patient was referred to the thoracic surgery clinic due to an incidental finding of a right lung middle lobe mass revealed by a computed tomographic (CT) scan of the chest, which was done as pre-operative imaging before hernial repair surgery. On standard chest X-ray and CT scan, a defined nodule was visible in the middle right lobe of the lung (4.1 cm in diameter) (Fig. 1).
Radiological examination of the chest of the patient. (A) Chest X-ray revealed a demarcated nodule located in the middle right lobe. (B) Chest CT scan displayed a 4.1 cm nodule with no mediastinal lymph node enlargement.
The patient underwent a right middle lung lobectomy. On gross examination, a round to oval white-tan well-demarcated mass filled the bronchial lumen, measuring 4.2 × 3.3 × 3.0 cm, which was 2 mm away from the uninvolved bronchial margin. Grossly, the lesion had a tan, fleshy cut surface. On histopathological examination, the tumor exhibits various growth patterns: organoid, trabecular, follicular, pseudopapillary, and solid patterns (Fig. 2). The cells show neuroendocrine differentiation with salt-and-pepper chromatin and mild eosinophilic cytoplasm. The classic stroma of high vascularization was seen, but the striking diffuse finding was the abundant mucinous stroma. Multiple small foci of necrosis were present, and the mitotic rate was five mitoses per 2 mm^2^ in the hotspot (Fig. 3).
Histopathological analysis of atypical lung carcinoid with different proliferation patterns observed under a light microscope and after H&E stain. (A, B) trabecular proliferation pattern with vascular stoma, original magnification x20 (C). Solid and organoid proliferation patterns, original magnification x40.
(A, B) abundant mucinous stroma, original magnification x40. (C) Area of necrosis, original magnification x100.
On immunohistochemistry, the tumor showed diffuse positivity for pan-cytokeratin (CK AE1/AE3) and the neuroendocrine markers synaptophysin and chromogranin, with additional positivity for thyroid transcription factor 1 (TTF1). In contrast, CK7, CK20, and caudal-type homeobox 2 (CDX2) were negative. The Ki-67 proliferation index was approximately 10% (Fig. 4). The detailed immunohistochemical findings are summarized in Table 1. These findings, in combination with the histologic features, support the diagnosis of atypical carcinoid with prominent mucinous stroma.
Tumor cells are positive for pan-CK, TTF-1, Synaptophysin, and chromogranin (A-D, respectively). The staining index for Ki67 was between 5 and 20% (E). Alcian blue stain demonstrates extracellular mucinous secretions. (original magnification x40 (F).
Discussion
Pulmonary carcinoid tumors are malignant neuroendocrine neoplasms that generally follow an indolent course, yet they can display a wide range of histologic patterns. Carcinoids with abundant mucinous stroma are exceedingly rare, with only two well-documented pulmonary atypical carcinoid cases reported in the literature [3, 4]. Extrapulmonary counterparts—particularly in the thymus have been reported more frequently, with at least six published cases demonstrating similar mucin-rich stromal features [5, 6]. Many of these thymic cases exhibited destructive growth, early metastasis, or poor outcomes, suggesting that mucinous stromal production may correlate with more aggressive biological behavior.
Beyond case reports, mucinous stromal change has been described in a subset of extrapulmonary neuroendocrine neoplasms, including pancreatic and gastrointestinal NETs, where mucin deposition has been associated with altered tumor–stroma signaling and more infiltrative growth patterns [7, 8]. Although these findings cannot be directly extrapolated to pulmonary carcinoids, they support the concept that stromal mucin in NETs may reflect underlying biological alterations rather than a purely degenerative process.
The biological significance of mucinous stroma in neuroendocrine tumors remains uncertain. Proposed mechanisms include stromal metaplasia, mucin-secreting transdifferentiation, or tumor–stroma signaling pathways that promote extracellular mucin deposition. Recent molecular studies have emphasized the importance of extracellular matrix remodeling in NET progression, including mucin-associated pathways such as MUC1/MUC2 dysregulation and TGF-β–mediated stromal activation [9, 10]. Given the limited number of reported cases, firm conclusions regarding the biological impact of mucinous stroma in atypical carcinoids cannot yet be drawn.
From a diagnostic perspective, mucin-rich atypical carcinoids require careful distinction from primary mucinous lung tumors, including mucinous adenocarcinoma, mucin-rich salivary-type tumors, and mucinous cystadenoma, as well as metastatic mucin-producing neoplasms [11]. In addition, rare mucin-producing salivary gland-type pulmonary tumors such as mucoepidermoid carcinoma and adenocarcinoma NOS should be considered [12]. Correlation of clinical, radiologic, histologic, and immunophenotypic features remains essential for accurate classification.
Management of pulmonary carcinoids continues to rely on complete surgical resection. For atypical carcinoids, lobectomy with systematic lymph node sampling is preferred. Given the aggressive behavior described in mucin-rich thymic carcinoids, careful assessment of lymph nodes and margins may be warranted in similarly unusual pulmonary variants. Adjuvant therapy remains controversial; ENETS recommends postoperative therapy for node-positive ACs, while NCCN suggests it for stage III disease [13]. More recently, ESMO guidelines have emphasized individualized risk stratification incorporating mitotic index, Ki-67, margin status, and nodal disease when considering adjuvant treatment in pulmonary NETs [14].
Prognostic uncertainty remains significant due to the rarity of mucin-rich ACs. Lung cases have shown variable behavior, whereas thymic cases demonstrate poorer outcomes. Although stromal mucin has been proposed as a possible marker of biologic aggressiveness, current evidence is insufficient and inconsistent across organ systems [7–10]. As such, the prognostic impact of mucinous stroma cannot be reliably established and warrants documentation and long-term follow-up.
We have described an unusual and rarely reported variant of atypical carcinoid with prominent mucinous stroma in the lung. The tumor’s behavior is not well characterized, and the subsequent optimal treatment options remain uncertain. Similar cases in the thymus exhibit aggressive behavior and outcomes. We also emphasize the importance of clinicopathologic and radiologic evaluation to ensure accurate diagnosis and appropriate management.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1WHO Classification of Tumours Editorial Board . Thoracic tumours, 5th edn. International Agency for Research on Cancer: Lyon, 2021.
- 2Metovic J, Barella M, Pelosi G. Neuroendocrine neoplasms of the lung: a pathology update. Memo 2021;14:381–5. 10.1007/s 12254-021-00681-w · doi ↗
- 3Sweeney EC, Cooney T. Mucin-producing atypical bronchial carcinoid. J Clin Pathol 1978;31:1218–25. 10.1136/jcp.31.12.1218219040 PMC 1145534 · doi ↗ · pubmed ↗
- 4Nannini N, Bertolini F, Cavazza A. et al. Atypical carcinoid with prominent mucinous stroma: a hitherto unreported variant of pulmonary neuroendocrine tumor. Endocr Pathol 2010;21:120–4. 10.1007/s 12022-010-9115-x 20195926 · doi ↗ · pubmed ↗
- 5Gao Z, Kahn L, Bhuiya T. Thymic carcinoid with mucinous stroma: a rare variant of carcinoid with an aggressive clinical course. Ann Diagn Pathol 2006;10:114–6. 10.1016/j.anndiagpath.2005.07.01716546049 · doi ↗ · pubmed ↗
- 6Suster S, Moran CA. Thymic carcinoid with prominent mucinous stroma. Am J Surg Pathol 1995;19:1277–85. 10.1097/00000478-199511000-000087573690 · doi ↗ · pubmed ↗
- 7Perren A, Couvelard A, Scoazec JY. et al. Stromal changes in neuroendocrine tumors: biological and prognostic implications. Endocr Relat Cancer. 2020;27:R 369–R 380. 10.1530/ERC-20-0253 · doi ↗
- 8Klöppel G, Rindi G. Neuroendocrine neoplasms of the pancreas and gastrointestinal tract: morphology and stroma interaction. Virchows Arch. 2021;480:247–257. 10.1007/s 00428-021-03211-5 · doi ↗