Sex differences in clinical and imaging characteristics of axial juvenile spondyloarthritis
Adam S Mayer, Rui Xiao, Timothy G Brandon, Pamela F Weiss, Amita Aggarwal, Amita Aggarwal, Ruben Burgos-Vargas, Robert A Colbert, Gerd Horneff, Ronald M Laxer, Kirsten Minden, Angelo Ravelli, Nicolino Ruperto, Judith A Smith, Matthew L Stoll, Shirley M Tse, Filip Van den Bosch

TL;DR
This study finds that males with axial juvenile spondyloarthritis show more inflammatory signs and MRI features compared to females at diagnosis.
Contribution
The study identifies sex-based differences in clinical and MRI features at diagnosis in axial juvenile spondyloarthritis.
Findings
Males had higher odds of inflammatory MRI lesions, bone marrow oedema, and pelvic enthesitis compared to females.
Males showed greater HLA-B27 positivity and elevated inflammatory markers.
No sex differences were observed in peripheral arthritis, enthesitis, or patient-reported outcomes.
Abstract
The impact of biologic sex in axial juvenile spondyloarthritis (axJSpA) is unknown. We assessed whether biologic sex is associated with disease manifestations, patient-reported outcomes, or characteristic sacroiliac joint (SIJ) MRI lesions in a large cohort of youths with classified axJSpA. This international multicentre cross-sectional study included youths aged <18 years with physician-diagnosed juvenile spondyloarthritis and fulfilling the classification criteria for axJSpA. Clinical and SIJ MRI data were available from the time axial disease was first diagnosed and were compared between males and females using Pearson’s chi-squared and Wilcoxon rank-sum tests, as appropriate. Multivariable logistic regression evaluated the association of sex with inflammatory and structural MRI lesions typical of axial disease. Among the 143 patients included, 67.1% were male. Males had…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
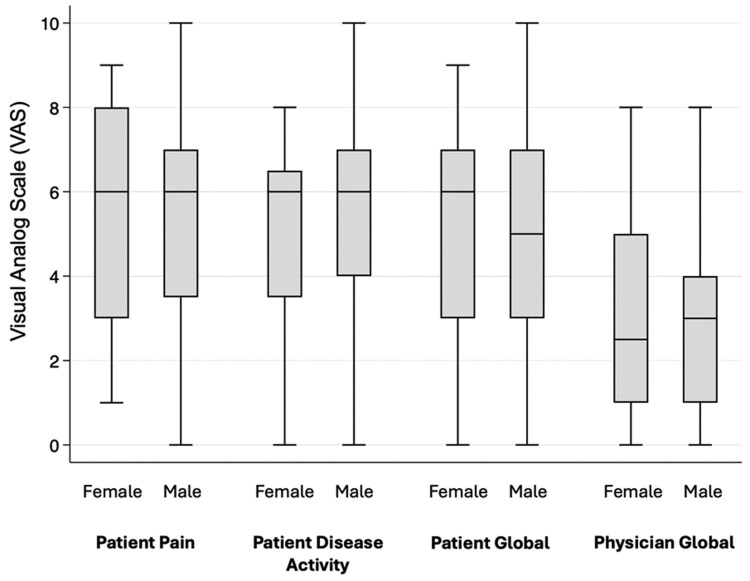 Figure 1
Figure 1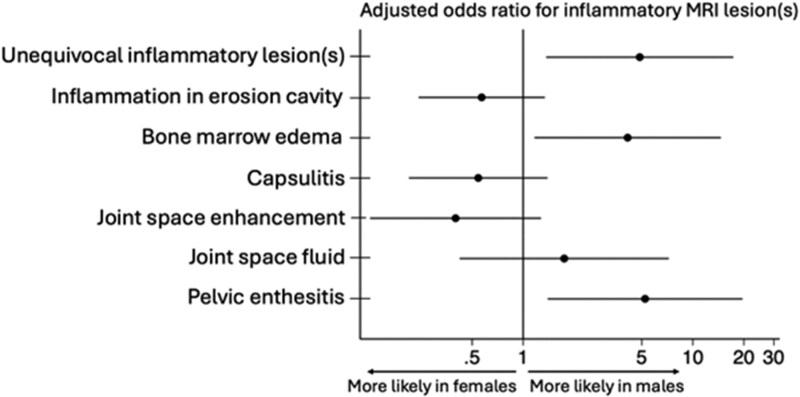 Figure 2
Figure 2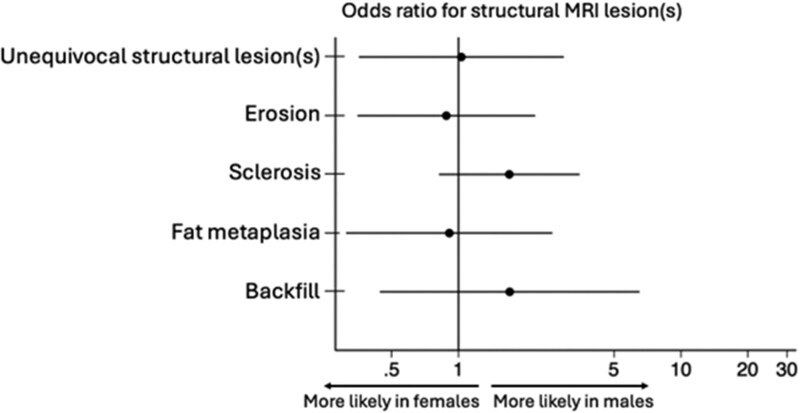 Figure 3
Figure 3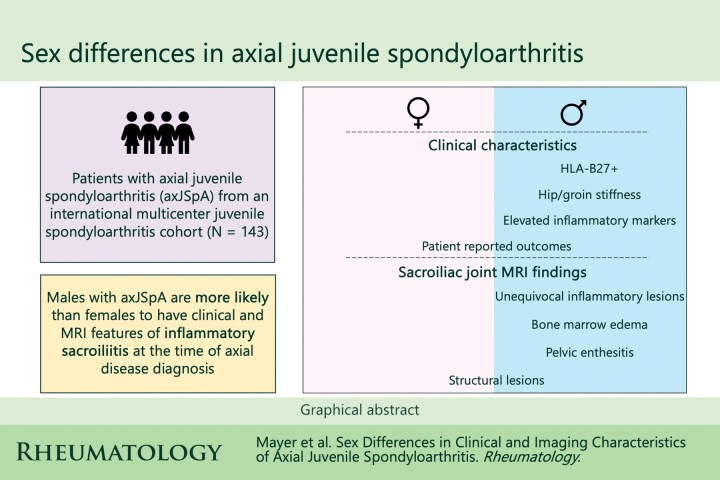 Figure 4
Figure 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsSpondyloarthritis Studies and Treatments · Autoimmune and Inflammatory Disorders Research · Scoliosis diagnosis and treatment
Introduction
Biologic sex is increasingly appreciated as having important implications in the manifestations and treatment of adult axial spondyloarthritis (axSpA). The pathophysiology underlying these sex differences remains poorly understood, with hypothesized roles for sex-dependent immunologic, genetic, and hormonal pathways(1–3). For example, the administration of estrogen to ovariectomized SKG mice has been found to suppress inflammatory arthritis and decrease expression of cytokines important in spondylarthritis pathogenesis, such as those on the interleukin-17 axis(1). Over the past decade, key differences in clinical characteristics, radiologic findings, and patient-reported outcomes have been identified between adult male and female patients with axSpA(4–12). Male sex is a known risk factor for both inflammatory sacroiliitis and radiographic progression in the sacroiliac joint (SIJ)(4,5,13,14) while females tend to have worse patient-reported outcomes and functional status(4,8–10,12,15–17). However, the existence of such sex differences in pediatric cohorts has never been explored and may plausibly differ from those in adults, especially given differences in the classification of axial disease in the two populations(18,19).
While an evaluation of sex differences in clinical characteristics and patient-reported outcomes is needed, differences in inflammatory and structural lesions in the SIJ on magnetic resonance imaging (MRI) are particularly important as these imaging findings are considered necessary for both the clinical diagnosis and classification of axial disease in juvenile spondyloarthritis (JSpA)(18,20). Additionally, inflammatory SIJ lesions are anatomically associated with the occurrence of local structural damage over time(21) and thus is a critical factor to assess in a young population who will live for decades with this chronic immune-mediated disease. Ultimately, an assessment of the association between biologic sex and clinical and imaging characteristics in patients with axial juvenile spondyloarthritis (axJSpA) is both clinically important and will lead to a better understanding of how to handle biologic sex as a covariate in trials of axJSpA.
The objective of this study was to determine whether biologic sex is associated with disease manifestations, patient-reported outcomes, or the presence of inflammatory and/or structural MRI lesions in the SIJ at the time axial disease was initially diagnosed in a large international multicenter cohort of youth with classified axJSpA.
Methods
This study was reviewed by the Children’s Hospital of Philadelphia (CHOP) Institutional Review Board (IRB), and the IRB determined the procedures met the exemption criteria per 45 Code of Federal Regulations 46.104(d) 4(iii) (IRB19–016078).
Study Design and Patient Selection
This study is a secondary analysis of data from an international multicenter cross-sectional study of a cohort of patients who met axJSpA criteria that have previously been published(18). Details on methodology and data collection have been previously described(18). The axJSpA classification score ranges from 0–100 with a classification threshold of ≥55 and is comprised of 6 domains: unequivocal evidence of inflammatory or structural lesions on MRI of the SIJs, pain chronicity, pain pattern, pain location, morning stiffness, and genetics (HLA-B27 positivity in patient or first-degree relative). This study included the youth from that cohort age <18 years with a physician diagnosis of JSpA who fulfilled classification criteria for axJSpA.
Cross-sectional data on clinical characteristics, including demographics, symptoms, exam findings, laboratory values, MRI, and patient/physician-reported outcomes were obtained from the clinical visit at which axial disease was diagnosed. Current use of medications known to treat axial disease were also available, including nonsteroidal anti-inflammatory drugs (NSAIDs), tumor necrosis factor alpha inhibitors (TNFi), interleukin-17 inhibitors (IL-17i) and Janus kinase inhibitors (JAKi). At least three members of a central imaging team with expertise in musculoskeletal imaging completed the MRI assessment for each patient. Imaging experts reviewed MRI studies independently and were blinded to clinical details other than age and sex.
Exposure and Outcomes
The primary exposure of interest was biologic sex. The co-primary outcomes were the presence on MRI of 1) Unequivocal SIJ inflammatory lesion(s), defined as bone marrow edema in ≥3 quadrants across all SIJ slices(22) and 2) Unequivocal SIJ structural lesion(s), defined as erosion in ≥3 quadrants or sclerosis or fat lesion in ≥2 SIJ quadrants or backfill or ankylosis in ≥2 joint halves across all SIJ slices and structural MRI lesions(22). Secondary outcomes included component inflammatory and structural MRI lesions as defined by the ASAS classification criteria for active sacroiliitis on MRI(23,24) and the preliminary Juvenile Idiopathic Arthritis Magnetic Resonance Imaging Score - Sacroiliac Joint (JAMRIS-SIJ) from the Outcome Measures in Rheumatology (OMERACT) working group(25) (Supplementary Table S1).
Covariates
Several covariates of interest were included given their clinical relevance and known association with biologic sex in adult cohorts of recent-onset axial spondyloarthritis(4), including age, HLA-B27 status, first-degree relative with spondyloarthritis, past or current peripheral arthritis, and inflammatory marker elevation (C-reactive protein (CRP) or erythrocyte sedimentation rate (ESR) normal versus abnormal).
Statistical Analysis
Clinical and imaging characteristics and patient/physician-reported outcomes were compared between male and female patients using Pearson’s chi-squared or Fisher’s exact test as appropriate for categorical variables and Wilcoxon rank-sum test for continuous variables. Separate multivariable logistic regression models were used to assess the association between inflammatory and structural MRI findings typical of axJSpA and sex. Candidate covariates with p<0.2 in univariate logistic regression models were sequentially selected for the multivariable model using a stepwise model selection approach. Given the association of HLA-B27 positivity with both inflammatory and structural sacroiliac joint lesions in adult axSpA(26), the interaction between sex and HLA-B27 status was also tested in the primary analysis. Covariate selection and goodness of fit testing (Akaike and Bayesian information criteria) were conducted separately for the inflammatory and structural lesion models. Missingness was <16% across all covariates and addressed using multiple imputation by chained equations with 10 imputations. All statistical analyses were performed using Stata 17.0 (StataCorp LLC, College Station, TX).
Results
Patient Cohort
143 patients met inclusion criteria of which 96 (67.1%) were male, 64.0% were HLA-B27 positive, and 18.1% had a family history of spondyloarthritis in a first degree relative.
Clinical Characteristics
Table 1 displays clinical characteristics of male and female patients. In comparison to females, male patients had significantly greater prevalence of HLA-B27 positivity (p<0.01), hip/groin stiffness (p=0.01), and elevated inflammatory markers (p=0.03). The discrepancy in inflammatory marker elevation was driven by CRP (elevated in 63.9% of males vs. 36.8% females) rather than ESR (elevated in 58.8% of males vs. 52.5% females). There were no significant differences between males and females in prevalence of comorbid psoriasis or inflammatory bowel disease, enthesitis, peripheral arthritis, total body pain, or use of NSAIDs or TNFi at the time axial disease was initially suspected. A majority of both male and female patients had symptom duration ≥12 weeks prior to axial disease evaluation and symptom duration did not significantly differ between groups (p=0.24). Patient- and physician-reported measures also did not significantly differ between male and female patients (Figure 1).
Inflammatory MRI Lesions
Differences in imaging characteristics between sexes are shown in Table 2. In univariate analyses, male patients with axJSpA had a significantly greater prevalence of pelvic enthesitis (p<0.01), subchondral bone marrow edema (p<0.01), and unequivocal sacroiliac joint inflammation on MRI (p<0.01) compared to females. After adjusting for age and inflammatory marker elevation, the odds of unequivocal inflammatory lesions typical of axial disease remained significantly higher in male patients (OR 4.86, 95% CI 1.37–17.32). In models assessing component inflammatory lesions, the adjusted odds of pelvic enthesitis outside the sacroiliac joint (OR 5.23, 95% CI 1.39–19.61) and subchondral bone marrow edema (OR 4.13, 95% CI 1.17–14.62) remained significantly higher in males than females (Figure 2). The results were similar when using the multiply-imputed datasets, and interaction between sex and HLA-B27 status was not significant in any of the models.
Structural MRI lesions
Univariate analyses did not reveal any significant differences between male and female patients with respect to unequivocal or component structural MRI lesions (Figure 3). Multiple imputation did not change the results, and interaction between sex and HLA-B27 was again not significant.
Discussion
There has been significant interest over the past decade in exploring sex differences in manifestations and outcomes of adult axSpA. This study leveraged a large international, multicenter cohort of youth with classified axJSpA to evaluate key clinical and imaging differences between male and female patients. At the time axial disease was first diagnosed, male youth with axJSpA were significantly more likely than females to have hip symptoms, HLA-B27 positive status, elevated inflammatory markers and active inflammatory sacroiliitis lesions. Patient-reported outcomes did not differ between sexes. These sex differences have important implications in the design of trials in axJSpA and offer an early window into the differences observed between male and female patients in adult axSpA cohorts.
Similar to known sex differences in adult axSpA(4,13), male youth with axJSpA were found to have a greater burden of inflammatory sacroiliac joint lesions on MRI, CRP elevation, and HLA-B27 positivity. Interestingly, despite the known association of HLA-B27 positivity with inflammatory and structural sacroiliac joint lesions in axSpA(26,27) and radiographic progression in adult males(28,29), HLA-B27 did not reach significance for inclusion in the inflammatory or structural sacroiliitis models or as an interaction term. Male patients with axJSpA also reported hip stiffness significantly more than their female counterparts. A Chinese retrospective cohort study of adult ankylosing spondylitis patients reported a greater degree of hip involvement at a younger age in men (median symptom onset 18 vs. 23 years) with a similarly earlier age of total hip arthroplasty, albeit in a cohort with <10% female patients(30). Despite the significantly higher prevalence of patient-reported hip stiffness in males in our cohort, there were no sex differences in physician-confirmed hip arthritis on exam, suggesting that the increased hip symptoms reported by male patients may be referred pain and/or stiffness from active inflammatory sacroiliitis in this group.
While several distinctions between male and female patients in this juvenile cohort are consistent with sex differences reported in the adult axSpA literature, there are also notable differences. First, despite structural sacroiliitis being more common in adult males(5,13,14), these differences were not observed in this study. This is possibly due to the study cohort consisting of youth with newly diagnosed axial disease and thus with less time to accrue significant structural lesions. A recent longitudinal study showed that anatomic regions of the SIJ affected by inflammatory sacroiliitis lead to local structural sacroiliitis over time(21). Thus, it is possible that the higher degree of active inflammatory sacroiliitis in male axJSpA patients may offer an early window into the higher burden of structural sacroiliitis and radiographic progression observed in adult males(5–7,13,14). Second, adult females with axSpA are additionally more likely to have worse pain scores and functional outcomes with a higher degree of tender joints and entheses(4,7–12,15–17,31). In contrast, the patient-reported pain and disease activity scores did not significantly differ between sexes in this juvenile cohort. There were also no differences in total body pain, peripheral arthritis, or clinically-defined enthesitis. It is possible that differences in VAS scores and joint/enthesis tenderness in adult cohorts may be biased by comorbid fibromyalgia that predominates in female patients(9,32), particularly in cohorts of non-radiographic axSpA. Female pediatric patients more broadly with juvenile idiopathic arthritis and enthesitis-related arthritis tend to have worse pain scores(33), but this may be driven by peripheral symptoms and thus sex differences may not manifest in an axial disease cohort. Third, the prevalence of comorbid IBD and psoriasis did not differ between male and female youth despite the greater prevalence of these comorbidities in adult females with axSpA(34,35). This may be due to the younger median age of our cohort with less time for comorbidity development, particularly IBD which has an initial peak incidence at age 15–30 years(36,37).
There are several strengths to this study. The study population was drawn from a large international multicenter cohort of patients who fulfilled classification criteria for axJSpA. Our findings therefore are likely generalizable to the broader axJSpA population but should not be extrapolated to patients with JSpA without axial disease. The involvement of expert radiologists in the interpretation of sacroiliac joint MRI and use of data-driven definitions of inflammatory and structural sacroiliac joint lesions enhance the validity of the outcomes explored in this study. There are also several limitations. There is a possibility of variation across centers in clinical practice around the diagnosis of JSpA and in the specific MRI protocol employed. However, these variations further enhance the generalizability of our findings to the real world where clinical practice and imaging protocols often differ between sites. This study is cross-sectional and includes patients with axJSpA at the time axial disease was initially suspected. Further study is therefore needed to determine how these sex differences may change longitudinally or in those with longer-established disease. As with any observational study there was missing data. However, this was minimal and there were no significant changes to results after multiple imputation, thus adding confidence to our findings. Active use of medications such as NSAIDs and TNFi that treat axial disease did not significantly differ between sexes and thus are unlikely to confound the observed sex differences in this cohort.
In summary, male youth with axJSpA were significantly more likely than females to have clinical and MRI features of active inflammatory sacroiliitis at the time axial disease was first diagnosed. While some differences observed between male and female youth with axJSpA mirror known differences in adult axSpA, several key distinctions from adult axSpA were found, reaffirming axJSpA as a distinct disease entity. Considering these findings, trials in axJSpA should consider stratification by sex in their study design.
Supplementary Material
1
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Jeong H, Bae EK, Kim H, Eun YH, Kim IY, Kim H, Estrogen attenuates the spondyloarthritis manifestations of the SKG arthritis model. Arthritis Res Ther. 2017 Sep 7;19(1):198.28882159 10.1186/s 13075-017-1407-9PMC 5590166 · doi ↗ · pubmed ↗
- 2Tsui HW, Inman RD, Paterson AD, Reveille JD, Tsui FWL. ANKH variants associated with ankylosing spondylitis: gender differences. Arthritis Res Ther. 2005;7(3):R 513–525.15899038 10.1186/ar 1701 PMC 1174945 · doi ↗ · pubmed ↗
- 3Sexual Dimorphism in the Th 17 Signature of Ankylosing Spondylitis. [cited 2025 Feb 26]; Available from: https://acrjournals.onlinelibrary.wiley.com/doi/10.1002/art.3946410.1002/art.3946426473967 · doi ↗ · pubmed ↗
- 4Tournadre A, Pereira B, Lhoste A, Dubost JJ, Ristori JM, Claudepierre P, Differences Between Women and Men With Recent-Onset Axial Spondyloarthritis: Results From a Prospective Multicenter French Cohort. Arthritis Care Res. 2013;65(9):1482–9.10.1002/acr.2200123463610 · doi ↗ · pubmed ↗
- 5Webers C, Essers I, Ramiro S, Stolwijk C, LandewéR, van der Heijde D, Gender-attributable differences in outcome of ankylosing spondylitis: long-term results from the Outcome in Ankylosing Spondylitis International Study. Rheumatol Oxf Engl. 2016 Mar;55(3):419–28.10.1093/rheumatology/kev 34026385369 · doi ↗ · pubmed ↗
- 6Baraliakos X, Listing J, von der Recke A, Braun J. The natural course of radiographic progression in ankylosing spondylitis: differences between genders and appearance of characteristic radiographic features. Curr Rheumatol Rep. 2011 Oct;13(5):383–7.21706179 10.1007/s 11926-011-0192-8 · doi ↗ · pubmed ↗
- 7van der Slik B, Spoorenberg A, Wink F, Bos R, Bootsma H, Maas F, Although female patients with ankylosing spondylitis score worse on disease activity than male patients and improvement in disease activity is comparable, male patients show more radiographic progression during treatment with TNF-α inhibitors. Semin Arthritis Rheum. 2019 Apr;48(5):828–33.30253878 10.1016/j.semarthrit.2018.07.015 · doi ↗ · pubmed ↗
- 8Lee W, Reveille JD, Davis JC, Learch TJ, Ward MM, Weisman MH. Are there gender differences in severity of ankylosing spondylitis? Results from the PSOAS cohort. Ann Rheum Dis. 2007 May 1;66(5):633–8.17127685 10.1136/ard.2006.060293 PMC 1954622 · doi ↗ · pubmed ↗