Umbrella-like systolic billowing of redundant mitral leaflets on left ventriculography in barlow mitral valve disease
Takeshi Nishi, Jagadeesh K Kalavakunta, Ashok Akula, Frank Saltiel

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
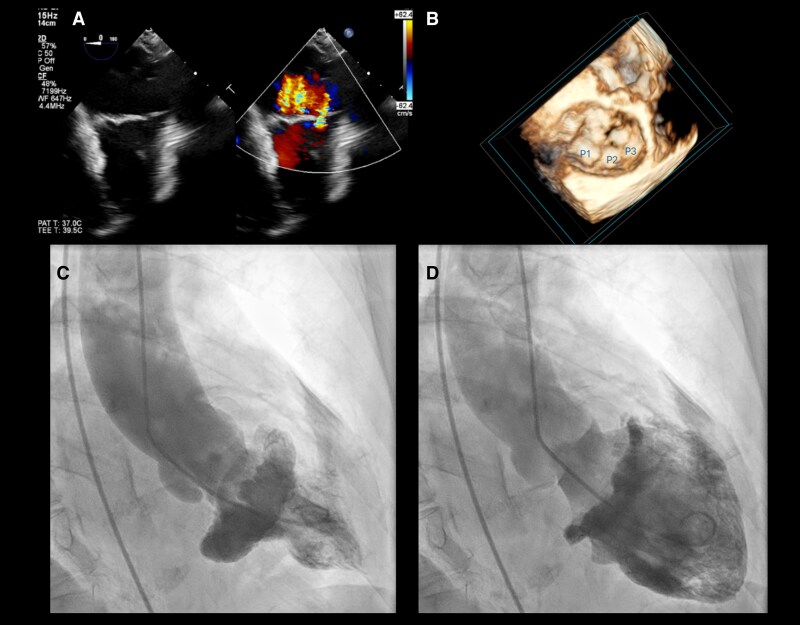 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCardiac Valve Diseases and Treatments · Cardiovascular Function and Risk Factors · Cardiac Structural Anomalies and Repair
An 81-year-old woman with a history of coronary artery disease, atrial fibrillation, and long-standing mitral valve prolapse presented with progressive exertional dyspnoea and palpitations. Cardiac examination revealed a late systolic murmur, prompting comprehensive imaging to assess mitral regurgitation (MR).
Transoesophageal echocardiography demonstrated bileaflet myxomatous prolapse with marked leaflet redundancy and thickening exceeding 3 mm. The mitral annulus was dilated with an average diameter >40 mm. Colour Doppler revealed three holosystolic MR jets (Panel A and Supplementary data online, Video S1), and quantitative assessment of the dominant jet showed an effective regurgitant orifice area of 0.45 cm^2^, consistent with severe MR. Multiplane imaging confirmed absence of mitral annular disjunction. Three-dimensional transoesophageal echocardiography further demonstrated complex multisegment systolic billowing, supporting a Barlow-type degenerative phenotype (Panel B and Supplementary data online, Video S2).
Left ventriculography, performed in the right anterior oblique 30° projection during invasive coronary assessment, provided an uncommon but striking depiction of global leaflet motion (see Supplementary data online, Video S3). In systole, markedly redundant mitral leaflets ballooned into the left atrium, forming a dome-shaped, umbrella-like multilobulated configuration (Panel C). In early diastole, the leaflet tissue returned toward the ventricle with restoration of coaptation (Panel D). No aortic regurgitation was identified on echocardiography. Although left ventriculography is no longer routinely used for evaluation of MR, this case illustrates its ability to visualize the integrated motion of excessive leaflet tissue in a manner complementary to echocardiography.
This image highlights a rarely documented ventriculographic appearance of advanced Barlow mitral valve disease and provides an intuitive visualization of leaflet excess that underlies severe degenerative MR.
Supplementary Material
qyag046_Supplementary_Data