Lung ultrasound guided management in chronic heart failure: an updated systematic review and meta-analysis of randomized controlled trials
Ravi Chotalia, Kevin Mohee, Robert Ambrogetti, Minesh Chotalia, Latif Raiyan Rahman, Hasan Mohiaddin

TL;DR
A review of recent studies finds that lung ultrasound-guided management reduces urgent heart failure visits but not hospitalizations, with no impact on mortality or kidney function.
Contribution
An updated synthesis of randomized trials shows LUS-guided care reduces urgent heart failure visits compared to standard care.
Findings
LUS-guided management significantly reduced heart failure urgent visits by 69%.
No significant difference was found in heart failure hospitalization rates.
Mortality, hypokalaemia, and worsening renal function were unaffected by LUS-guided management.
Abstract
Existing systematic reviews support the prognostic and therapeutic value of lung ultrasound (LUS) in heart failure (HF), but recent randomized controlled trials (RCTs) in chronic HF justify an up-to-date synthesis. A systematic search of OVID via Medline, SCOPUS, COCHRANE, and CINAHL was conducted from inception until 25 February 2025. The study was registered with PROSPERO (ID: CRD420251003434). RCTs of LUS interventions in patients with chronic HF were included. The primary outcomes were HF urgent visits and HF hospitalizations. Secondary outcomes included mortality, hypokalaemia, and worsening renal function. Five RCTs, involving a total of 694 patients, were included in meta-analyses, with variability in LUS-based definitions of pulmonary congestion across studies. LUS-guided management was associated with a significant reduction in HF urgent visits [RR 0.31 (95% CI 0.17, 0.55), I2…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
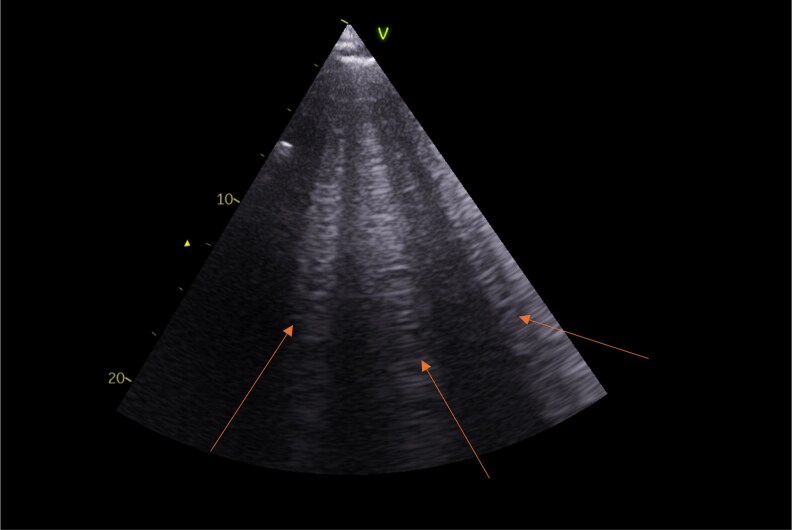 Figure 1
Figure 1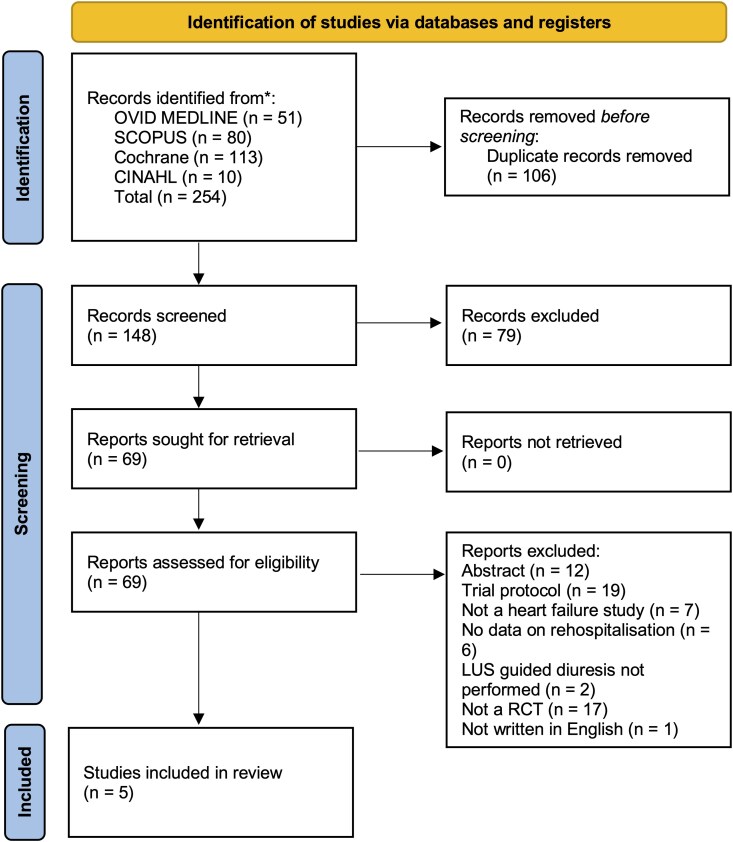 Figure 2
Figure 2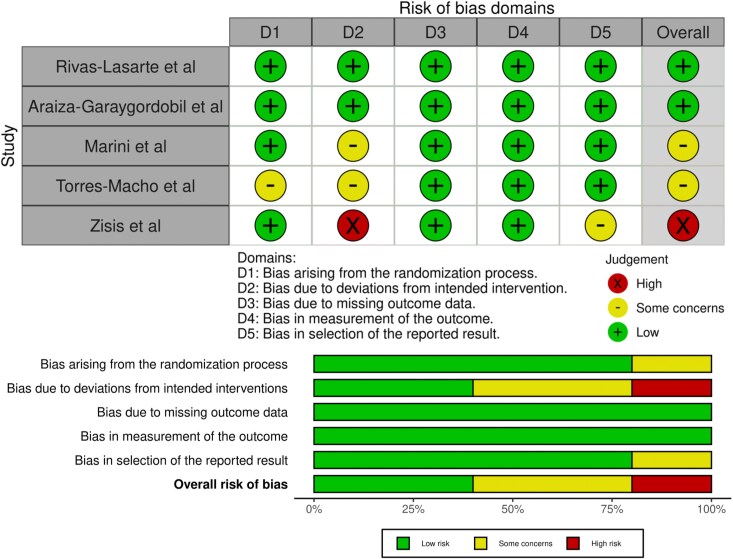 Figure 3
Figure 3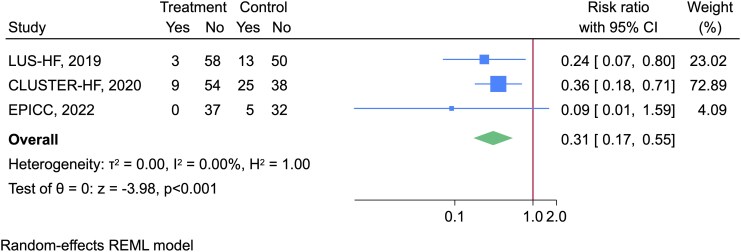 Figure 4
Figure 4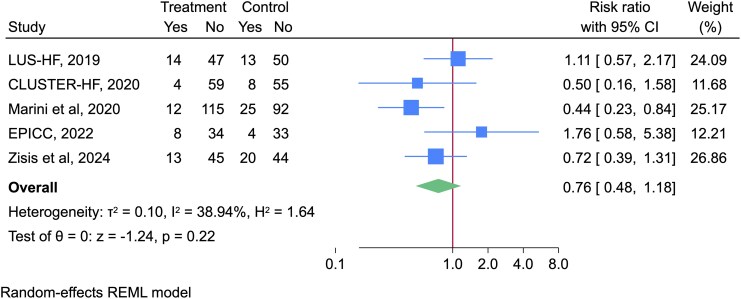 Figure 5
Figure 5| Study | LUS-HF | CLUSTER-HF | Marini | EPICC | Zisis |
|---|---|---|---|---|---|
| Year of publication | 2019 | 2020 | 2020 | 2022 | 2024 |
| Country | Spain | Mexico | Italy | Spain | Australia |
| HF population | Patients hospitalized with HF | Patients hospitalized with HF | Chronic HF on OMT | Patients hospitalized with HF | Patients hospitalized with HF |
| Follow-up (months) | 6 | 6 | 3 | 6 | 3 |
| Definition of congestion | Total number of B-lines across 8 chest zones ≥3 | Total number of B-lines across 8 chest zones ≥3 | Lung comet score definition | Bilateral presence of B-lines in one pulmonary region and/or significant pleural effusion (>1 cm) | Total number of B-lines across 8 chest zones ≥10 |
| LUS group treatment regimen | Follow-up at 14 days, 1 month, 3 months and 6 months. | Follow-up at day 14, 6 weeks and 3 and 6 months. | Follow-up not specified | Follow up at week 1–2, and 1,3 and 6 months. | Follow up at week 1–2, week 3 and 1 month |
| Control group | Follow-up at 14 days, 1 month, 3 months and 6 months | Follow-up at day 14, 6 weeks and 3 and 6 months | Follow-up not specified | Follow-up at week 1–2, and 1,3 and 6 months | Follow-up at week 4 with phone-call assessment |
| Primary outcome | Composite of urgent HF visits, HF hospitalization or all-cause death | Composite of urgent HF visits, HF hospitalization or all-cause death | HF hospitalization | Composite of urgent HF visit, HF hospitalization, CV death | Composite of HF hospitalization or all-cause death |
| Primary outcome result | Significant reduction in LUS group | Significant reduction in LUS group | Significant reduction in LUS group | No significant difference between groups | No significant difference between groups |
| Secondary outcome | Significant reduction in urgent HF visits in LUS group. No significant difference in HF hospitalizations or death. No difference in rates of hypokalaemia or worsening renal function. Significant improvement in 6MWD and QoL scores in LUS group | Significant difference in urgent HF visits in LUS group. No significant difference in HF hospitalizations or death. No difference in rates of hypokalaemia or worsening renal function or QoL scores | No significant difference in mortality. Significant difference in NT-proBNP value and QoL scores in LUS group | No significant difference in HF hospitalization, ED visits, all-cause mortality, worsening renal function, or QoL scores | No significant difference in HF hospitalization or death. |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsUltrasound in Clinical Applications · Ultrasound and Hyperthermia Applications · Heart Failure Treatment and Management
Introduction
Heart failure (HF) is a common and progressive condition that affects approximately 64 million people worldwide.^1^ The number of patients with HF is increasing due to several factors, including improvements in diagnosis, an ageing population and improved survival after diagnosis.^2^
Decompensated HF, resulting in HF hospitalizations or urgent HF visits, is the rapid onset or change in symptoms or signs of HF. HF hospitalizations continue to rise in incidence and have become the leading cause of hospitalization in patients over 65 years of age.^3^ Associated with significant morbidity and mortality, it also carries a huge financial burden, with over 80% of the cost of HF originating from hospitalizations or urgent HF visits.^4^ As a result, strategies to reduce HF hospitalizations and urgent HF visits are of considerable research interest.
Pulmonary congestion is a characteristic feature of HF decompensation. However, traditional physical examination, such as auscultation for crackles or assessment of jugular venous pressure, has a limited sensitivity in identifying signs of decompensated HF.^5^ Point of care lung ultrasound (LUS) is a diagnostic tool that can be used to identify pulmonary congestion in HF. LUS detects B-lines (Figure 1), which are vertical reverberation artefacts that correlate with extravascular lung water, and has shown a high sensitivity in detecting pulmonary congestion.^6^ Moreover, multiple randomized controlled trials (RCTs) have identified that the use of LUS can improve outcomes in acute^7^ and chronic HF.^7,8^ This has led to the recognition of the benefits of LUS by the European Society of Cardiovascular Imaging in a 2023 consensus statement.^9^ However, the most up-to-date European Society of Cardiology HF guidelines^10,11^ do not provide a recommendation for its use in chronic HF, but note it may be considered in the setting of acute HF presentations. LUS may also be incorporated within a multiorgan ultrasound assessment of congestion, recognizing that pulmonary congestion represents only one component of the systemic congestive phenotype in HF, as demonstrated by Pugiliese et al.^12^
Lung ultrasound depicting B-lines (indicated by red arrows). A total of three B-lines are visible. Appropriate written consent was obtained from the patient for acquisition and use of this image.
A prior meta-analysis assessed the use of LUS in chronic HF^8^ and found a nonsignificant trend toward reduced HF hospitalizations and a significant reduction in urgent HF visits. Since that publication, further RCTs^13,14^ have been published. Therefore, we conducted an updated meta-analysis of LUS-guided management in patients with chronic HF, providing an up-to-date synthesis of its impact on HF related clinical outcomes.
Methods
This systematic review was conducted by adhering to the criteria defined in the Cochrane Handbook for Systematic Reviews of Interventions^15^ and reported using the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) 2020 statement.^16^ The protocol was registered with PROSPERO under the ID: CRD420251003434.
Search strategy
A systematic search was conducted from inception to 25 February 2025 using the following databases: OVID via Medline, SCOPUS, COCHRANE, and CINAHL. The full details of the search strategy and MeSH terms are included as Supplementary Material S1. Reference lists of other systematic reviews and RCTs were also screened.
Eligibility
We only included RCTs that compared the efficacy of LUS-guided outpatient management and usual care in adults ≥18 years old with HF. Only trials that reported the primary and/or secondary outcomes of interest were included in the review.
Duplicate records were automatically identified by Rayyan, followed by manual review and removal by the reviewers. Titles and abstracts were independently screened by two reviewers (R.A. and H.M.), with any conflicts resolved by discussion. All nonrandomized studies and articles not written in English were excluded.
Data extraction
Data were extracted from selected studies by two independent reviewers (H.M. and R.C.). Data, including study characteristics (author, year, and country), patient characteristics (sample size, demographic data, HF aetiology), type of LUS intervention (length of intervention, length of follow up, definition of congestion), and reported outcome measures (HF urgent visit rates, HF hospitalization rates, mortality rates and other secondary outcomes) were collected.
Primary outcome
The primary outcomes were HF-related urgent visits (defined as a same day or ambulatory urgent appointment that did not meet the threshold for hospital admission) and HF-related hospitalization. These outcomes were analysed and reported separately. Risk ratios were calculated with 95% confidence intervals (CIs), comparing the LUS-guided management with usual care.
Secondary outcomes
Secondary outcomes included mortality, hypokalaemia, and worsening renal function. These outcomes were compared between the LUS- guided cohort and usual care cohort and expressed as risk ratios with 95% CIs. Studies that did not report data on the secondary outcome of interest were excluded from the corresponding analysis.
Bias assessment
The risk of bias assessment was conducted independently by two reviewers (R.C. and M.C.), using the Cochrane risk of bias 2 tool.^17^ Any conflicts were resolved by discussion with a third reviewer who was not involved in the initial assessment. The risk of bias plots was generated using the robvis tool.^18^
Statistical analysis
Meta-analyses were performed for each outcome of interest using the random-effects model. Statistical heterogeneity was assessed using the I^2^ statistic, with an I^2^ of 0–25% considered low, 26–50% moderate, and >50% considered high heterogeneity. Meta-regression could not be performed due to the small number of studies within the meta-analysis. All analyses were performed using Stata18 (StataCorp, College Station, TX).
Results
After removing duplicate articles (n = 106) and following title and abstract screening, a total of 69 records were identified for full-text review (Figure 2). Of these records, 64 were excluded for the reasons listed in Figure 2. The remaining 5 studies^13,14,19–21^ were included in the systematic review and meta-analysis, involving 694 HF patients.
Prisma flow diagram of study selection. Flow diagram showing the identification, screening, eligibility, and inclusion of studies for the systematic review.
- shows a detailed description of the five included studies published between 2019 and 24. The median age of patients ranged from 62 to 80 years, and the prevalence of male participants ranged from 45% to 81% (Table 1). Two of the included studies originated in Spain^14,19^ and one study was from Italy,^20^ Mexico,^21^ and Australia.^13^
All studies examined the use of LUS vs. usual care in the outpatient management of HF patients. All of the studies except Marini et al.^20^ examined LUS in all HF patients recently hospitalized for decompensated HF. In contrast, Marini et al. studied chronic patients without recent hospitalization, but who only had HF with reduced ejection fraction. Usual care varied across studies: in three studies, patients had equivalent follow-up to the LUS group^14,19,21^ and had LUS performed, but the results were not available to clinicians. The usual care group in Zisis et al.^13^ had a reduced follow-up intensity compared to the LUS group (only at week 4 with a telephone assessment). Marini et al.^20^ did not report the frequency or nature of follow up appointments in either LUS-guided or usual care groups. Length of follow up varied, with three studies following up to 6 months^14,19,21^ and two studies following up to 3 months.^13,20^ The definition of congestion varied across studies (see Table 1).
Regarding outcome measures, the primary outcome of three studies was a composite of urgent HF visits, HF hospitalizations, or all-cause death.^14,19,21^ The primary outcome in Zisis et al. was a composite of HF hospitalizations or CV death,^13^ whereas the primary outcome in Marini et al. was HF hospitalizations.^20^ All studies reported HF hospitalizations and mortality. Three studies reported urgent HF visits separately.^14,19,21^ Difference in quality of life was reported in four studies;^14,19–21^ however, these results could not be synthesized as different quality of life tools were used.
Quality assessment
Two studies were deemed to be low risk of bias,^19,21^ two were judged to have some concerns,^14,20^ and one was deemed to be high risk.^13^ Frequent sources of bias originated from domain 2 (bias originating from deviations from intended interventions), due to patients being unblinded, and extra follow-up for the LUS cohort compared to usual care, which could have influenced results. Figure 3 illustrates a detailed risk of bias assessment.
Risk of bias assessment of the included studies using ROB 2.0 tool. Risk of bias plots were generated using the robvis tool.
Primary outcomes
A meta-analysis of three studies^14,19,21^ showed a significant reduction in proportion of patients with urgent HF visits [RR 0.31 (95% CI 0.17, 0.55), I^2^ = 0%] (Figure 4).
Forest plot illustrating the effect of LUS interventions compared to usual care on HF urgent visits during follow-up period.
A meta-analysis of five studies showed that whilst there was a trend towards reduced HF hospitalizations with LUS-guided management, this was not significant [RR 0.76 (95% CI 0.48, 1.18), I^2^ = 38.9%] (Figure 5).
Forest plot illustrating the effect of LUS interventions compared to usual care on HF hospitalizations during follow-up period.
Secondary outcomes
There was no significant difference in rates of mortality with LUS use [RR 1.25 (95% CI 0.73, 2.14), I^2^ = 0%] (see Supplementary data online, Figure S1). The number of patients with hypokalaemia was reported in two studies.^19,21^ A meta-analysis of these two studies showed no significant difference in rates of hypokalaemia with LUS use [RR 0.72 (95% CI 0.21, 2.42), I^2^ = 39.4%] (see Supplementary data online, Figure S2). The number of patients with worsening renal function was reported in three studies.^14,19,21^ A meta-analysis of these three studies showed no significant difference in rates of worsening renal function with LUS use [RR 1.21 (95% CI 0.69, 2.15), I^2^ = 0%] (see Supplementary data online, Figure S3).
Discussion
In this meta-analysis, we examined the impact of LUS-guided management in patients with chronic HF. Our findings indicate that the use of LUS is associated with a significant reduction in urgent HF visits compared with usual care, alongside a nonsignificant reduction in HF hospitalizations. This effect is most likely due to the ability of LUS to detect subclinical pulmonary congestion not apparent on clinical examination, allowing clinicians to more appropriately titrate diuretic therapy. LUS-guided therapy in HF appears safe, with no significant difference between groups in secondary outcomes, including mortality, hypokalaemia, or worsening renal function.
The previous meta-analysis by Mhanna et al.^8^ included three RCTs and found LUS-guided management significantly reduced urgent HF visits [RR 0.32 (95% CI 0.18–0.59), P = 0.0002] and, although there was a trend to reduction in HF hospitalizations, this was not significant [RR 0.65 (95% CI 0.34–1.22), P = 0.18]. Our analysis extends these findings by incorporating additional data from Torres-Macho et al.^14^ and Zisis et al.^13^
The effects of LUS-guided management on HF hospitalizations and urgent visits varied across studies, with some trials demonstrating statistically significant reductions and others showing nonsignificant trends. Several factors may account for this variability. First, studies varied in how pulmonary congestion was defined on LUS. Zisis et al.^13^ used threshold of >10 B-lines across eight lung zones to define congestion, whereas Torres-Macho et al.^14^ required bilateral positive lung zones, with each zone having ≥3 B-lines. LUS-HF and CLUSTER-HF^19,21^ used a threshold of ≥3 B-lines in total across all lung zones, and Marini et al. applied the lung comet score.^20^ Differences in these thresholds likely affected which patients were identified for intervention and may have influenced the magnitude of observed benefit. Standardizing B-line thresholds in future studies may improve comparability.
Second, patient characteristics varied. Studies such as Torres-Macho et al. and Zisis et al. included older patients (81 and 76 years, respectively) and higher proportion of patients with CKD (48% and 57%, respectively) compared with prior studies (average age 62.5–71.5 years; CKD 27–36%). These factors can reduce responsiveness to diuretics^22^ and may blunt the impact of LUS-guided therapy.
Third, trial size and recruitment challenges, including those caused by the COVID-19 pandemic, may have limited statistical power. For example, Torres-Macho^14^ enrolled 79 of 152 planned patients, and Zisis et al.^13^ enrolled 122 of the 404 planned patients, which may have increased the risk of type 2 error and contribute to nonsignificant findings in some outcomes.
Strengths and limitations
There are multiple strengths of our study. Our search was conducted across multiple major databases. Moreover, the study protocol was prespecified and registered, reducing risk of bias in study selection and analysis. Only RCTs were included, which represent the highest level of clinical evidence. Most outcomes demonstrated low heterogeneity, e.g. I^2^ = 0% for urgent HF visits, mortality, and worsening renal function. In contrast, moderate heterogeneity was observed for HF hospitalizations, I^2^ = 38.9%, indicating some between study variability. While low heterogeneity suggests consistency of effect estimates due to broadly similar study designs and outcome definitions across studies, the absence of detectable heterogeneity is uncommon in clinical meta-analyses and should be interpreted cautiously, as it could reflect a limited statistical power to detect heterogeneity due to the small number of included studies. Further limitations include the inclusion of two trials that were underpowered, and one study was judged to be at high risk of bias, which may limit the precision and robustness of our results.
Clinical implications
Our results suggest that the use of LUS can be effective in reducing HF urgent visits and possibly hospitalizations. Most included studies recruited HF patients after an acute decompensation; however, Marini et al. also assessed the use of LUS in chronic HF outpatients with a reduced ejection fraction. From a health system perspective, LUS- guided care is rapid, relatively inexpensive, and a simple technique that can be taught to nonspecialists to perform with good accuracy following brief, structured training.^23,24^ This evidence supports LUS as a safe, scalable adjunct in outpatient HF care.
Future research
Further studies are required to assess which patient populations derive the greatest benefit from the use of LUS. The results from these trials suggest the use of LUS is equally beneficial across different HF ejection fractions and in chronic outpatients vs. postdischarge populations. However, its benefit may be reduced in older patients and in those with CKD, highlighting the value of dedicated trials in older, comorbid populations. It is also important to note that pulmonary congestion is defined inconsistently across LUS trials. Establishing a standardized definition, and identifying which most accurately reflects congestion, is essential. It is also increasingly recognized that pulmonary congestion may only be one aspect of a multiorgan process of decompensation in HF.^12,25^ Indeed, ultrasound assessment of systemic venous congestion, such as inferior vena cava size and renal venous flow patterns, have been shown to carry independent and incremental prognostic information in HF, in addition to LUS assessment.^12,25^ It is possible that integrating ultrasound assessment of pulmonary congestion and systemic venous congestion into a combined assessment may help to better identify patients at risk of decompensation and guide therapy, although this requires further study.
Conclusion
In conclusion, our meta-analysis demonstrated that outpatient LUS-guided management is associated with a significant reduction in urgent HF visits and a nonsignificant reduction in HF hospitalizations. Importantly, LUS-guided management appears safe, with no observed increases in mortality, hypokalaemia, or worsening renal function. Future studies should focus on establishing an optimal, standardized LUS-based definition of pulmonary congestion in chronic HF to improve comparability and clinical application.
Supplementary Material
qyag049_Supplementary_Data
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Groenewegen A, Rutten FH, Mosterd A, Hoes AW. Epidemiology of heart failure. Eur J Heart Fail 2020;22:1342.32483830 10.1002/ejhf.1858 PMC 7540043 · doi ↗ · pubmed ↗
- 2Dunlay SM, Roger VL. Understanding the epidemic of heart failure: past, present, and future. Curr Heart Fail Rep 2014;11:404–15.25182014 10.1007/s 11897-014-0220-x PMC 4224604 · doi ↗ · pubmed ↗
- 3Ziaeian B, Fonarow GC. The prevention of hospital readmissions in heart failure. Prog Cardiovasc Dis 2016;58:379–85.26432556 10.1016/j.pcad.2015.09.004PMC 4783289 · doi ↗ · pubmed ↗
- 4Heidenreich PA, Albert NM, Allen LA, Bluemke DA, Butler J, Fonarow GC et al Forecasting the impact of heart failure in the United States: a policy statement from the American Heart Association. Circ Heart Fail 2013;6:606–19.23616602 10.1161/HHF.0b 013e 318291329 a PMC 3908895 · doi ↗ · pubmed ↗
- 5Kelder JC, Cramer MJ, van Wijngaarden J, van Tooren R, Mosterd A, Moons KGM et al The diagnostic value of physical examination and additional testing in primary care patients with suspected heart failure. Circulation 2011;124:2865–73.22104551 10.1161/CIRCULATIONAHA.111.019216 · doi ↗ · pubmed ↗
- 6Platz E, Merz AA, Jhund PS, Vazir A, Campbell R, Mc Murray JJ. Dynamic changes and prognostic value of pulmonary congestion by lung ultrasound in acute and chronic heart failure: a systematic review. Eur J Heart Fail 2017;19:1154–63.28557302 10.1002/ejhf.839PMC 5731779 · doi ↗ · pubmed ↗
- 7Li Y, Ai H, Ma N, Li P, Ren J. Lung ultrasound-guided treatment for heart failure: an updated meta-analysis and trial sequential analysis. Front Cardiovasc Med 2022;9:943633.36072884 10.3389/fcvm.2022.943633 PMC 9441745 · doi ↗ · pubmed ↗
- 8Mhanna M, Beran A, Nazir S, Sajdeya O, Srour O, Ayesh H et al Lung ultrasound–guided management to reduce hospitalization in chronic heart failure: a systematic review and meta-analysis. Heart Fail Rev 2022;27:821–6.33835332 10.1007/s 10741-021-10085-x · doi ↗ · pubmed ↗