Suicide risk in people with tuberculosis in Republic of Korea: a nationwide cohort, 2012–2021
Chiwook Chung, Seung Won Lee, Dawoon Jeong, Hongjo Choi, Hojoon Sohn, Young Ae Kang

TL;DR
This study finds that people with tuberculosis in South Korea have a higher risk of suicide, especially early after diagnosis, and identifies factors like mental health and age that contribute to this risk.
Contribution
The study provides the first nationwide analysis of suicide risk in TB patients in South Korea, revealing age- and sex-specific risk factors and timing of suicide incidence.
Findings
Suicide incidence was 0.77 per 1000 person-years among TB patients in South Korea.
Suicide risk was highest immediately after TB diagnosis and decreased over time.
Mental health conditions, age, and comorbidities were key risk factors varying by age group.
Abstract
Many individuals with tuberculosis (TB) experience various psychological problems after TB diagnosis, and they may also have suicidal ideations and suicidal attempts associated with TB-related depression or stigma. Until now, little is known about suicide rates among individuals with TB. We aimed to investigate the trends, characteristics, and contributing factors of suicide deaths among individuals with TB, using a Republic of Korea nationwide cohort. This was a retrospective nationwide cohort study using data of the K-TB-N cohort. We analyzed 310,194 individuals with TB registered in the Korean National Tuberculosis Surveillance System between 2012 and 2021. Suicidal deaths were identified using the International Classification of Diseases 10th revision codes (X60–X84) from the Statistics Korea database. Participants were followed up until death, censoring, or December 2022. We…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
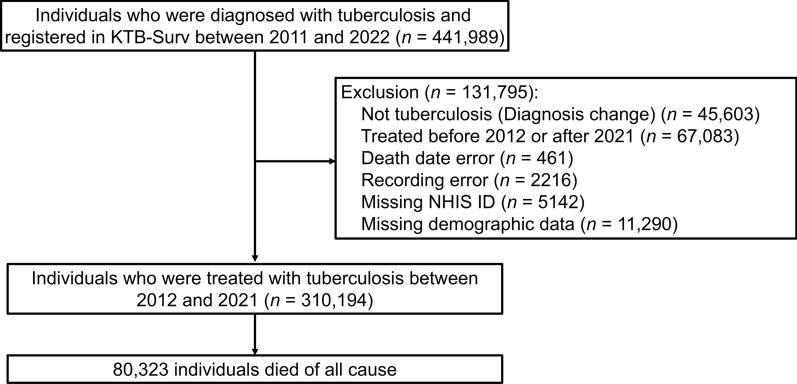 Figure 1
Figure 1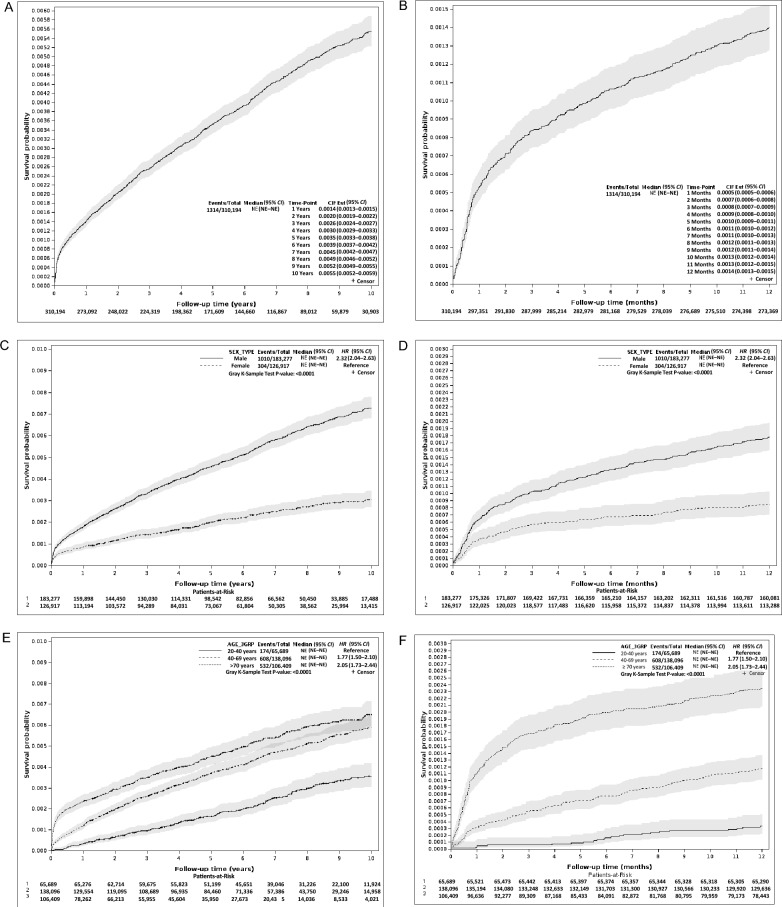 Figure 2
Figure 2 Figure 3
Figure 3- —https://doi.org/10.13039/100018688Korea Disease Control and Prevention Agency
- —Ministry of Education of the Republic of Korea
- —National Research Foundation of Korea
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsTuberculosis Research and Epidemiology · Suicide and Self-Harm Studies · Infectious Diseases and Tuberculosis
Background
Tuberculosis (TB) remains a significant global health concern, particularly in resource-limited high-burden countries [1]. As per the World Health Organization (WHO), there were approximately 10.8 million new TB cases and 1.25 million TB-related deaths in 2023 [1]. Beyond the physical morbidity and mortality associated with TB, there is growing recognition of the mental health and social burdens experienced by individuals diagnosed with TB [2]. These include stigma, social isolation, economic burden accompanying prolonged treatment, and comorbidities such as depression and anxiety [3–5]. More than 30% of patients with TB experienced depression [5]. The presence of these mental health issues not only impairs quality of life and treatment adherence but also increases the risk of suicidal behaviors among affected individuals [6, 7].
Despite substantial progress in national TB control programs, Republic of Korea has the highest TB incidence (39.8/100,000 population in 2022) and mortality (3.8/100,000 population in 2022) among the Organization for Economic Co-operation and Development (OECD) countries [8, 9]. In addition, suicide is a major public health issue in Republic of Korea, with a suicide rate of approximately 27.3/100,000 population in 2023 (the 5th leading cause of death), significantly exceeding the OECD average (approximately 11/100,000 population in 2020) [10, 11]. Mental health challenges in patients with TB may be exacerbated by the chronic nature of the disease, adverse drug effects, socioeconomic vulnerabilities, stigma associated with infectious diseases, and exacerbation of comorbidities [3, 12]. Thus, TB-related neuroendocrinological dysfunction, stigma, depression, social exclusion, and economic hardship may have collectively contributed to increase suicide risk [3, 13–16].
While limited, existing studies from countries such as South Africa and Ethiopia suggest elevated suicide risk among TB patients, particularly during early treatment stages [17, 18]. A recent meta-analysis reported that the pooled prevalence of current suicidal ideations and suicidal attempts within the last year among individuals with TB was 8.5% [95% confidence interval (CI) 5.8–12.3%] and 3.1% (95% CI 2.2–4.5%), respectively [7]. Although this analysis included nine studies and 8770 participants, several methodological limitations were noted. Most of the included studies employed a cross-sectional design and had relatively small sample sizes, and few studies provided data on suicide deaths, highlighting the need for additional epidemiological evidence [7]. Moreover, this analysis also highlighted the lack of large-scale longitudinal studies assessing actual suicide mortality (not just ideation or attempts) among individuals with TB, particularly in the Western Pacific or high-income Asian countries [7].
Understanding the burden and risk factors for suicide among individuals with TB is essential for informing integrated care strategies that incorporate mental health support into TB control programs. The primary objective of this study was to estimate the incidence of suicide and identify clinical and sociodemographic factors associated with suicide risk among individuals with TB, thereby providing evidence to inform integrated TB–mental health care strategies. Therefore, we explored the incidence and risk factors for suicide among individuals with TB using the Republic of Korea national TB cohort (K-TB-N cohort) [19]. To overcome the limitations of previous studies (e.g. a cross-sectional design and small sample sizes), we 1) constructed a nationwide retrospective cohort; 2) identified suicide deaths using national cause-of-death statistics; and 3) explored the incidence, demographics, disease-related factors, and comorbidities associated with suicide risk among patients with TB.
Methods
Data source
The K-TB-N cohort was constructed by linking three databases: 1) the Korean National Tuberculosis Surveillance System (KTB-Surv) established by the Korea Disease Control and Prevention Agency, containing TB notification data for those registered between 2011 and 2022 [20]; 2) the National Health Information Database (NHID), established by the National Health Insurance Service (NHIS) [21]; and 3) the Statistics Korea database on cause-of-death statistics [19]. The KTB-Surv database contains individual patient data including age, sex, nationality, TB notification date, TB lesion (pulmonary or extrapulmonary), sputum acid-fast bacillus (AFB) smear, previous TB history, and drug susceptibility test results. The NHID database contains additional patient data, including 1) socio-demographic data (e.g., age, sex, residential region, household income, and death), 2) disease diagnosis (according to the International Classification of Diseases 10th revision, ICD-10), 3) medications (such as name, quantity, and duration), 4) health services types used (e.g., inpatient procedures, prescriptions, and operations), and 5) healthcare provider information (location, level, and type of healthcare provider). The Statistics Korea database provides information on underlying causes of death. All databases were linked using deterministic matching through unique national identification numbers, ensuring exact one-to-one correspondence between individuals across datasets. As shown in Fig. 1, individuals without valid NHIS identifiers or with missing linkage keys were excluded from the analysis to ensure accurate matching across datasets.Fig. 1. Study flowchart for participants inclusion process. KTB-Surv, Korean Tuberculosis Surveillance System
Study population
This was a nationwide retrospective cohort study of individuals with TB, conducted from May 2023 to April 2025. Figure 1 illustrates the participant inclusion process. The KTB-Surv database identified 441,989 individuals with TB who were registered and treated between 2011 and 2022. Among them, we excluded individuals with 1) change in the diagnosis (not TB, n = 45,603), 2) treatment before 2012 or after 2021 (2011: because of incompleteness of KTB-Surv database, and 2022: owing to ongoing treatment and unconfirmed treatment outcomes, n = 67,083), 3) death date error (n = 461), 4) recording error (n = 2216), 5) missing NHIS ID (n = 5142), and 6) missing demographic data (n = 11,290). Consequently, the remaining 310,194 individuals with TB who were registered and treated between 2012 and 2021 were included in this study. All participants were followed up until December 2022. The follow-up ended at death (including suicide, the study outcome) or censoring. The overall mean follow-up duration was 5.5 ± 3.3 years.
Measurements
The primary outcome of this study was suicide death identified by the cause of death as ICD-10 codes X60–84 (intentional self-harm) [6]. We identified the cause of death from the national mortality statistic of Statistics Korea [22].
Data of demographic, socioeconomic, TB-related, comorbid, and mental disorder factors were collected from the KTB-Surv and the NHID. The demographic variables included age and sex. Socioeconomic variables included residential region, household income, and disability status. The residential regions were classified into provinces and metropolitan areas. Household income levels were categorized into quintiles (Q1 = lowest; Q5 = highest) based on subscribers’ annual national health insurance premiums. Medical aid beneficiaries (lowest 3%) were categorized as Q0. TB-related variables included TB lesions (pulmonary vs. extrapulmonary), drug resistance (either isoniazid or rifampin/multidrug resistance), previous TB history, and sputum AFB smear positivity.
Comorbidities were evaluated using the Charlson comorbidity index (CCI) score [23] and data of cardiovascular disease, cerebrovascular disease, dementia, chronic obstructive pulmonary disease, rheumatic disease, peptic ulcer, chronic liver disease, diabetes, hemiplegia, chronic kidney disease, malignancy (either solid cancer or hematologic malignancy), and living with human immunodeficiency virus (HIV). Mental disorders included depression, anxiety, bipolar disorder, affective disorder, schizophrenia, alcohol use disorder, and substance use disorder. Comorbidities and mental disorders were identified using insurance claims of relevant ICD-10 codes within one year prior to the TB index date (Supplementary Table 1).
Statistical analysis
Continuous variables are presented as mean with standard deviation if normally distributed. Categorical variables are presented as proportion/percentages. Student t-test (for normally distributed variables) or the Mann–Whitney U test was used to compare continuous variables, whereas the chi-squared or Fisher exact tests were used to compare categorical variables. The incidence rate of suicide was calculated as the ratio of the number of suicide deaths to the number of person-years (PY) at risk (per 1000 PY). Poisson regression was used to assess changes in suicide incidence according to time elapsed since TB diagnosis. The Kaplan–Meier survival curve was used to describe the cumulative incidence of suicide. To identify factors associated with suicide, a Cox proportional hazards model with non-suicide death treated as a competing event was used. Covariates included sex, age, residential region, household income, presence of disabilities, type of TB lesions, drug resistance, previous TB history, sputum AFB smears, comorbidities, and mental disorders. Demographic and TB-related variables were included in the multivariate analysis, regardless of the P values in the univariate analysis, while other variables showing statistical significance (P < 0.05) in the univariate analysis were also entered into the multivariate model. Multicollinearity among variables was assessed using the Variance Inflation Factor. As for comorbidities, Model 1 included CCI scores, whereas Model 2 included individual disease categories. Sex and age (< 40, 40–69, and > 70 years) stratified analyses were conducted to identify specific risk factors for suicide. In addition, stratified analyses were conducted according to the TB treatment phase (during vs. after TB treatment) to explore potential differences in risk factors across these periods. All P values were two-tailed, and P values < 0.05 were considered statistically significant. Statistical analyses were performed using the SAS Enterprise Guide 7.1 (SAS Institute Inc., Cary, NC, USA).
Results
General characteristics of participants
Among the 80,323 all-cause deaths, 1314 were identified as suicidal deaths. Table 1 presents the general characteristics of the study population according to vital status and cause of death. The mean age of the population was 57.8 ± 20.0 years, with men comprising 59.1%. Regarding the demographic characteristics, the suicidal death group had the highest proportion of men (76.9%), whereas the mean age in the non-suicidal death group was the highest (74.3 ± 13.0 years). The proportion of those with AFB smear positivity was higher in the suicide group (37.7%) and non-suicide groups (37.3%) than in the survivors (27.0%). Regarding comorbidities, both the CCI score and the proportions of individual comorbid diseases increased in the order of survivors, suicide group, and non-suicide group. Mental disorders were the least frequent in the survivor group and most frequent in the suicidal death group. In the comparison by sex, a higher proportion of older adults was observed in women, whereas there was no notable difference in comorbidities and mental disorders between sexes (Supplementary Table 2). Table 1. General characteristics of individuals with tuberculosis by vital status and cause of deathNTotalSurvivorSuicide deathNon-suicide death310,194 (100%)229,871 (74.11%)1314 (0.42%)79,009 (25.47%)n%n%n%n%Male sex183,27759.08132,27357.54101076.8649,99463.28Age, years57.8 ± 20.052.1 ± 18.961.5 ± 17.974.3 ± 13.0 0–1976862.4876153.31151.14560.07 20–2927,6878.9327,40711.92654.952150.27 30–3930,3169.7729,49112.83947.157310.93 40–4939,36512.6936,12215.7114911.3430943.92 50–5952,53916.9444,74019.4625419.3375459.55 60–6946,19214.8934,98015.2220515.6011,00713.93 70–7956,69518.2832,54314.1630523.2123,84730.18 ≥ 8049,71416.0316,9737.3822717.2832,51441.15Region (Province)176,24756.82126,98755.2478459.6748,47661.36Low income (Q0)25,1118.1013,5105.881319.9711,47014.52Low income (Q1)51,75616.6939,02716.9822116.8212,50815.83Disabilities42,64513.7522,7719.9125219.1819,62224.84Pulmonary TB246,32679.41180,36578.46112185.3164,84082.07Drug resistance13,8894.4810,6164.62644.8732094.06Previous TB history32,85610.5923,08710.0419314.69957612.12Positive AFB smear92,03929.6762,05026.9949537.6729,49437.33CCI score2.2 ± 1.91.7 ± 1.72.5 ± 2.03.4 ± 2.1Cardiovascular disease63,97420.6234,31814.9332024.3529,33637.13Cerebrovascular disease39,60412.7717,9027.7918213.8521,52027.24Dementia28,6809.2590503.94775.8619,55324.75COPD136,52344.0192,22940.1264549.0943,64955.25Rheumatic disease13,3324.3089193.88775.8643365.49Peptic ulcer82,07326.4654,40323.6742132.0427,24934.49Chronic liver disease92,29629.7560,69426.4048636.9931,11639.38Diabetes91,93329.6454,28223.6146035.0137,19147.07Hemiplegia59891.9319760.86272.0539865.04Chronic kidney disease13,4234.3355482.41534.0378229.90Malignancy35,98511.6019,5848.5216812.7916,23320.55Living with HIV5940.194560.2070.531310.17Depression37,07611.9520,2408.8031023.5916,52620.92Anxiety disorder49,94416.1029,84812.9835226.7919,74424.99Bipolar disorder11,6593.7641971.83715.4073919.35Affective disorder20090.6512120.53272.057700.97Schizophrenia71122.2934031.48644.8736454.61Alcohol use disorder57551.8631231.36544.1125783.26Substance use disorder3340.111910.0860.461370.17TB tuberculosis; AFB acid-fast bacilli; CCI Charlson comorbidity index; COPD chronic obstructive pulmonary disease; HIV human immunodeficiency virus
Incidence and characteristics of suicide by sex and age group
Table 2 presents the distribution of suicidal deaths stratified by sex, age, and year of diagnosis. The incidence rate of suicide was 0.77/1000 PY, which was more than twice as high in men compared to that in women (1.03 vs. 0.42/1000 PY, respectively). The incidence rate also increased with age (0–19 years: 0.25/1000 PY vs. ≥ 80 years: 1.59/1000 PY). The incidence rate of suicide within one year after TB diagnosis was 2.04/1000 PY. Although a decreasing trend in the number of suicidal deaths within one year after TB diagnosis was observed longitudinally (2012: 93 cases vs. 2021: 33 cases), the incidence rate remained relatively stable throughout the study period owing to a decreasing trend in the total number of TB cases. Table 2. Distribution of suicide deaths among tuberculosis patients stratified by sex, age group, and year of diagnosisnTotal suicide deathsSuicide within 1 year after TB diagnosisDuration (PY)SuicideIR (per 1000 PY) with 95% CIDuration (PY)SuicideIR (per 1000 PY) with 95% CITotal310,1941,704,159.4213140.77 (0.73–0.81)283,179.535792.04 (1.88–2.22)Male183,277985,358.0610101.03 (0.96–1.09)166,406.754432.66 (2.42–2.92)Female126,917718,801.363040.42 (0.38–0.47)116,772.781361.16 (0.98–1.38)Age, years 0–19768659,622.25150.25 (0.15–0.42)7664.4810.13 (0–0.73) 20–2927,687202,672.33650.32 (0.25–0.41)27,608.59160.58 (0.33–0.94) 30–3930,316215,629.77940.44 (0.36–0.53)30,118.45230.76 (0.48–1.15) 40–4939,365262,825.921490.57 (0.48–0.67)38,554.90511.32 (0.98–1.74) 50–5952,539317,532.072540.80 (0.71–0.90)50,486.38981.94 (1.58–2.37) 60–6946,192242,854.202050.84 (0.74–0.97)43,024.17962.23 (1.81–2.72) 70–7956,695260,258.873051.17 (1.05–1.31)49,370.001523.08 (2.61–3.61) ≥ 8049,714142,764.012271.59 (1.40–1.81)36,352.541423.91 (3.29–4.60)Index Year 201242,611367,354.982690.73 (0.65–0.83)39,970.74932.33 (1.88–2.85) 201338,306300,857.122050.68 (0.59–0.78)35,829.07681.90 (1.47–2.41) 201437,164260,186.722080.80 (0.70–0.92)34,424.65661.92 (1.48–2.44) 201534,075210,945.411410.67 (0.57–0.79)31,339.98632.01 (1.54–2.57) 201632,939176,057.421260.72 (0.60–0.85)30,004.57521.73 (1.29–2.27) 201730,274137,942.871010.73 (0.60–0.89)27,474.00471.71 (1.26–2.27) 201828,450106,094.651010.95 (0.78–1.16)25,552.87582.27 (1.72–2.93) 201925,57075,030.00781.04 (0.83–1.30)22,834.06592.58 (1.97–3.33) 202021,21044,467.47521.17 (0.89–1.53)18,650.02402.14 (1.53–2.92) 202119,59525,222.77331.31 (0.93–1.84)17,099.57331.93 (1.33–2.71)PY person-year; IR incidence rate; CI confidence interval
Temporal distribution of suicide after TB diagnosis
Table 3 shows the distribution of suicidal deaths according to the time elapsed since TB diagnosis. Approximately one-third (31.3%, 411/1314; male: 311, famale: 100) of the suicides occurred during TB treatment. In particular, 12.6% (166/1314) and 19.9% (261/1314) of the cases occurred within 30 and 90 days of TB diagnosis, respectively. Thereafter, the incidence of suicide gradually decreased over time (P < 0.001, Fig. 2, Supplementary Fig. 1). Table 3. Numbers of suicide deaths by time interval since tuberculosis diagnosis stratified by sexTime to suicide, daysTotalIndex year2012201320142015201620172018201920202021Total 0–3016628141813171114241017 31–60558844638662 61–90408223348433 91–120253444422011 121–150205131022123 151–180244504203213 181–2705789811432741 271–360478995632230 ≥ 3618801971531609684736032223Male 0–3011925713101251018613 31–60417413537452 61–90286223215421 91–120221434422011 121–150154110021123 151–180192403202213 181–2704458810121630 271–360386584631230 ≥ 3616841481211168066614823183Female 0–30473753564644 31–60141431101210 61–90122000133012 91–12032010000000 121–15051021001000 151–18052101001000 181–270133101311111 271–36092411001000 ≥ 36119649324416181212940Fig. 2Cumulative incidence of suicide death since tuberculosis diagnosis stratified by sex and age, plotted using the Kaplan–Meier survival curve. A Total study period, B Within one year after tuberculosis diagnosis, C Total study period and stratified by sex, D Within one year after tuberculosis diagnosis and stratified by sex, E Total study period and stratified by age, and F Within one year after tuberculosis diagnosis and stratified by age
Contributing factors to suicide among individuals with TB
Our multivariate analysis models identified several significant factors contributing to suicidal death. Male sex, older age, low income, disability, pulmonary TB, and AFB smear positivity were significant factors contributing to suicide. Among comorbidities, a higher CCI score, rheumatic disease, chronic liver disease, and living with HIV were factors significantly contributing to suicide death. Among mental disorders, depression, anxiety disorder, affective disorder, and schizophrenia were significant contributing factors to suicide death (Table 4). Table 4. Estimated hazard ratios for demographic, tuberculosis-related, and comorbid risk factors contributing to suicide death after tuberculosis diagnosisUnivariate analysisMultivariate analysisModel 1Multivariate analysisModel 2HR95% CIaHR95% CIaHR95% CIMale sex2.3982.1092.7262.6752.3423.0552.6692.3353.050Age, years 0–19RefRefRef 20–291.2610.7202.2111.2500.7132.1931.2360.7052.169 30–391.7070.9902.9431.5650.9062.7021.5360.8892.652 40–492.1991.2933.7381.7051.0002.9051.6580.9732.827 50–593.0531.8145.1382.0861.2353.5262.0331.2023.438 60–693.1451.8625.3132.0661.2163.5112.0361.1973.463 70–794.2762.5467.1812.9191.7224.9512.9311.7274.975 ≥ 805.2783.1278.9073.9382.3076.7244.0512.3716.920Region (Province)1.1841.0601.3221.0770.9641.2041.0780.9641.204Low income (Q0)1.5561.2651.9151.1390.9161.4151.1330.9111.408Low income (Q1)1.0760.9031.2831.2481.0441.4931.2461.0411.490Disabilities1.8681.6282.1431.2371.0701.4311.2641.0911.463Pulmonary TB1.5101.2961.7591.2311.0251.4791.2411.0331.492Drug resistance1.2010.9341.5451.0780.8361.3881.0760.8351.387Previous TB history1.4351.2321.6731.1670.9991.3621.1711.0031.367Positive AFB smear1.4351.2781.6111.3061.1591.4721.3101.1621.476CCI score1.2001.1691.2331.0451.0111.080Cardiovascular disease1.7181.5131.9501.0800.9381.243Cerebrovascular disease1.5771.3481.8450.8460.7111.007Dementia1.1510.9131.451COPD1.3721.2311.5291.0160.9061.139Rheumatic disease1.5341.2191.9321.2791.0121.616Peptic ulcer1.4181.2631.5921.0660.9441.205Chronic liver disease1.5931.4241.7821.1781.0451.328Diabetes1.6331.4571.8291.0310.9101.167Hemiplegia1.7311.1822.5361.0730.7211.598Chronic kidney disease1.4651.1121.9290.9630.7261.279Malignancy1.4641.2441.7211.1350.9611.340Living with HIV2.7031.2865.6812.3921.1345.044Depression2.8542.5123.2431.8591.6002.1591.8851.6232.190Anxiety disorder2.2281.9712.5171.4441.2551.6611.4411.2521.658Bipolar disorder2.5301.9903.2161.0840.8341.4081.1130.8561.447Affective disorder3.5662.4365.2202.0041.3612.9522.0251.3752.984Schizophrenia2.8912.2493.7181.6021.2172.1081.6101.2232.120Alcohol use disorder2.5091.9103.2941.1730.8761.5701.1360.8471.523Substance use disorder4.7972.15110.6982.2961.0245.1462.2340.9975.010HR hazard ratio; aHR adjusted hazard ratio; CI, confidence interval; Ref. reference; TB tuberculosis; AFB acid-fast bacilli; CCI Charlson comorbidity index; COPD chronic obstructive pulmonary disease; HIV human immunodeficiency virus
In the analysis stratified by sex, older age was the most significant contributing factor among men, whereas it had no contribution in women (Supplementary Tables 3 and 4). In the younger age group (< 40 years), depression and schizophrenia were the only mental disorders that were contributing factors to suicide. In contrast, low household income status and AFB smear positivity were significant contributing factors in the 40–69 years age group (economically active population) in addition to mental disorders. In the older age group (> 70 years), disabilities, AFB smear positivity, chronic liver disease, and mental disorders were identified as factors contributing to suicide (Supplementary Table 5, 6, and 7).
In stratified analyses according to the TB treatment phase (during vs. after treatment), male sex, older age, sputum AFB smear positivity, depression, and anxiety disorder consistently showed significant associations with suicide (Supplementary Tables 8 and 9).
Discussion
In this nationwide study spanning a decade, we investigated the incidence, temporal patterns, and contributing factors of suicide in individuals with TB in Republic of Korea. Over a median follow-up period of 5.5 years, 1314 suicidal deaths were identified, accounting for 1.6% of all recorded deaths. Suicides in men accounted for more than three-quarters of suicidal deaths, and the suicide incidence rate was more than twice as high in men than that in women. Older adults aged ≥ 60 years comprised over half of suicide, with a clear age-dependent increase in suicide incidence. Notably, approximately one-third of suicides occurred during TB treatment, with the highest risk being within the first 30 days of TB diagnosis. Multivariate analyses identified male sex, older age, pulmonary TB, sputum AFB smear positivity, comorbidities, and pre-existing mental disorders as significant risk factors for suicide after TB diagnosis. To the best of our knowledge, this is the first study to comprehensively assess the burden and risk factors for suicide among individuals with TB at a national level over an extended period.
TB is an infectious disease that often requires isolation during the initial contagious phase, which may expose individuals to stigma and social exclusion, contributing to psychological distress [3, 14]. Despite the successful national TB control program and significant decline of TB burden in Republic of Korea, severe stigma associated with TB, particularly among socioeconomically disadvantaged patients with TB, remained underreported and neglected [24]. Notably, perceived discriminatory experiences were significantly related to poor self-rated health in Republic of Korea [25]. Among patients with TB, a high level of stigma was linked to depressive symptoms, whereas social support had an inverse association [26]. Depression is prevalent among patients with TB, with a meta-analysis estimating a pooled prevalence of 45.19% (95% CI 38.04–52.55%) [15]. Pathophysiological changes associated with chronic inflammation, such as neuroendocrinological and immunological dysfunction, caused by TB are also thought to contribute to depression and suicide [13]. In addition to the psychological burden, patients with TB frequently experience substantial economic hardship owing to treatment-related direct and indirect medical costs and unemployment during the treatment period [4, 16], with 43% of individuals facing catastrophic costs according to pooled estimates [4]. These combined psychological and economic stressors likely contribute to elevated rates of suicidal ideation and behavior in this population [7].
We found that 411 of 310,194 individuals with TB (0.13%) died of suicide during TB treatment, a rate comparable to those observed in patients with cancer (0.15%) [27], and stroke (0.12%) [28]. These findings support existing evidence that a diagnosis of severe physical illness is a major risk factor for suicide [29]. Importantly, the incidence rate of suicide within one year after TB diagnosis was 2.04/1000 person-years, which was markedly higher than the national average and highlights the vulnerability of patients with TB in the immediate post-diagnosis period [8, 10, 30].
The demographic patterns observed in our study align with national suicide statistics: suicide rates in Republic of Korea are more than twice as high among men compared to that in women and increase with age, particularly among those aged ≥ 70 years [30]. The higher rate of completed suicide among men has been partly attributed to the use of more lethal methods such as fire, jumping from heights, or firearms [31, 32]. In older adults, suicide is often associated with physical decline, loss of independence, and co-existing chronic illnesses [33]. Our stratified analysis revealed that older age was a significant suicide risk factor among men but not women, suggesting that sex-specific biologic or socio-behavioral mechanism may underlie age-related suicide risk in patients with TB. Further studies are required to clarify this association in women.
Notably, suicides were highly concentrated within the first month following TB diagnosis, and the elevated risk persisted throughout the initial 90-day period, suggesting a critical window for early psychological intervention. This pattern has also been reported in patients newly diagnosed with other serious medical conditions [29]. The acute psychosocial impact of a TB diagnosis, particularly when combined with the stigma of infectiousness, as reflected by the higher risk in those with pulmonary TB and smear positivity, may trigger suicidal ideation and behavior. Early psychological support may be critical during this vulnerable period. Unfortunately, no official social support is currently available to patients with TB dealing with isolation or social disconnection, particularly in the early stages following TB diagnosis. In this context, vulnerability assessment at the time of TB diagnosis and enhanced community-based care may be helpful for suicide prevention [34]. The following intervention programs should be considered for suicide prevention: early psychological screening at diagnosis, integration of suicide risk assessment in TB treatment protocols, community-based mental health linkage models, and peer support programs during the first months of treatment.
Despite the strengths of our study, including its large national sample size and robust link between TB and mortality data, several limitations must be acknowledged. First, suicide deaths were identified using national death certificate data, which may underreport suicides, particularly among older adults [35]. Given that the suicides of older adults are more likely to be underreported than those of people of other ages [36], the real suicide rate among men and older adults can be higher than that in our findings. Second, because this was an observational study, the association between several individual characteristics and suicide may not be causal. Third, time-dependent variables such as change in comorbid condition were not modeled dynamically and all covariates used in multivariable models were treated as fixed over time. Furthermore, several potential confounding factors, such as medication side effects, social support, and concurrent psychiatric treatment could not be accounted for. Finally, although our findings are relevant to high-income countries with well-established TB control programs, they may not be generalizable to low-resource settings.
Nevertheless, our findings highlighted the urgent need for integrated mental health support in TB care, particularly during the early treatment phase. Although Republic of Korea has implemented national suicide prevention policies since 2004 [37], the suicide rate remains high, and the stable incidence observed within one year of TB diagnosis suggests that these efforts may not sufficiently reach this vulnerable population. Individuals with TB, particularly newly diagnosed individuals, should be considered a high-risk group for suicide prevention strategies.
Our findings provide evidence for age- and context-specific interventions. Among younger adults (age < 40 years), preexisting mental health conditions are major risk factors, suggesting the need for appropriate psychiatric interventions. In economically active middle-aged adults (age 40–69 years), low income and infectiousness are predominant risk factors, underscoring the importance of socioeconomic support for mitigating stigmatization and providing economic assistance during treatment. For older adults (age > 70 years), comorbidities and disability are key drivers of suicide, indicating the need for multidisciplinary care to address existing chronic health conditions. In addition, considering protective factors against suicide, including perceived control, self-regulation and satisfaction, purpose-in-life, social support and connectedness, sense of belonging, and positive relationship, individualized intervention programs tailored to the contexts of TB should be developed [38].
Conclusions
Suicide is a significant but underrecognized outcome among individuals with TB. Suicides in men and older adults accounted for more than half of the suicidal deaths, with the highest risk being shortly after diagnosis. A combination of demographic, clinical, socioeconomic, and psychological factors contribute to suicide risk. The incidence of suicide within the first year following a TB diagnosis remained largely unchanged over time, highlighting the urgent need for earlier identification and timely intervention among high-risk individuals. Integrating mental health screening and support into the TB care continuum—through multi-sectoral collaborations across health, social welfare, and mental health systems—is essential to improve patient outcomes and prevent avoidable deaths. It would be valuable for future research to evaluate psychosocial interventions within TB programs and to examine temporal changes in mental health trajectories after TB diagnosis.
Supplementary Information
Additional file 1
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1World Health Organization. Global tuberculosis report 2024. https://www.who.int/teams/global-programme-on-tuberculosis-and-lung-health/tb-reports/global-tuberculosis-report-2024. Accessed June 17 2025.
- 2Statistics Korea. Causes of Death Statistics in 2023. 2024. https://kostat.go.kr/board.es?mid=a 20108010000&bid=11773&act=view&list_no=433679&tag=&n Page=3&ref_bid=11742,11743,11744,11745,11746,11747,11748,11749,11773,11774,11750&key Field=&key Word=. Accessed June 17 2025.
- 3Society at a Glance 2024: OECD Social Indicators. https://www.oecd.org/en/publications/society-at-a-glance-2024_918d 8db 3-en/full-report/suicides_357d 50c 7.html. Accessed November 22 2025.
- 4Statistics Korea. Suicide Rate. 2025. https://www.index.go.kr/unify/idx-info.do?idx Cd=8040. Accessed April 5 2025.