Bradycardic Tamponade: The Myxedema Pitfall
Mazen Ahmed, Ali Mohamedshata, Mohamed O Elhussain, Mohammed Elmojtaba Ahmed, Ali Ghandour

TL;DR
A case report shows that severe hypothyroidism can cause cardiac tamponade with a slow heart rate, highlighting the importance of echocardiography for diagnosis and treatment.
Contribution
Highlights a rare clinical scenario where bradycardia coexists with cardiac tamponade due to severe hypothyroidism.
Findings
A patient with severe hypothyroidism presented with tamponade physiology and bradycardia.
Echocardiography confirmed tamponade, and pericardiocentesis led to rapid hemodynamic recovery.
Thyroid hormone replacement and drainage prevented recurrence after excluding other causes.
Abstract
Severe, untreated hypothyroidism can produce large, slowly accumulating pericardial effusions; progression to cardiac tamponade is uncommon and may present without tachycardia because of blunted sympathetic tone. We report a middle-aged woman with long-standing hypothyroidism who presented with dyspnea and hypotension but a low resting heart rate. Transthoracic echocardiography demonstrated a large circumferential effusion with right ventricular diastolic collapse and marked respiratory variation in tricuspid inflow, confirming tamponade physiology. She underwent urgent, echo-guided pericardiocentesis with the removal of a large volume of straw-colored fluid, followed by short-term catheter drainage and the initiation of thyroid hormone replacement. Cultures and cytology were negative, and the clinical course, with rapid hemodynamic recovery and resolution of the effusion, supported…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
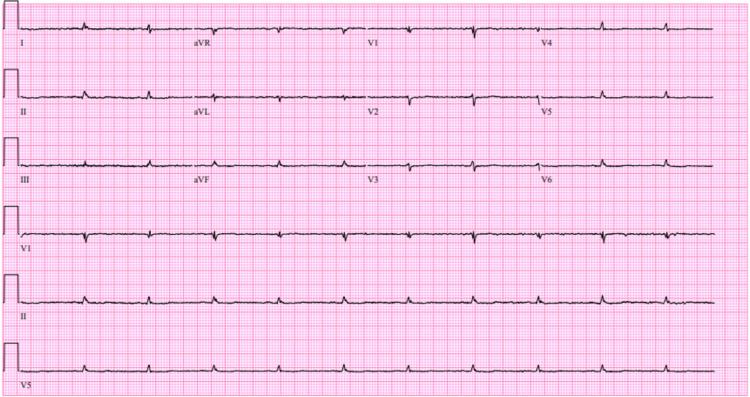 Figure 1
Figure 1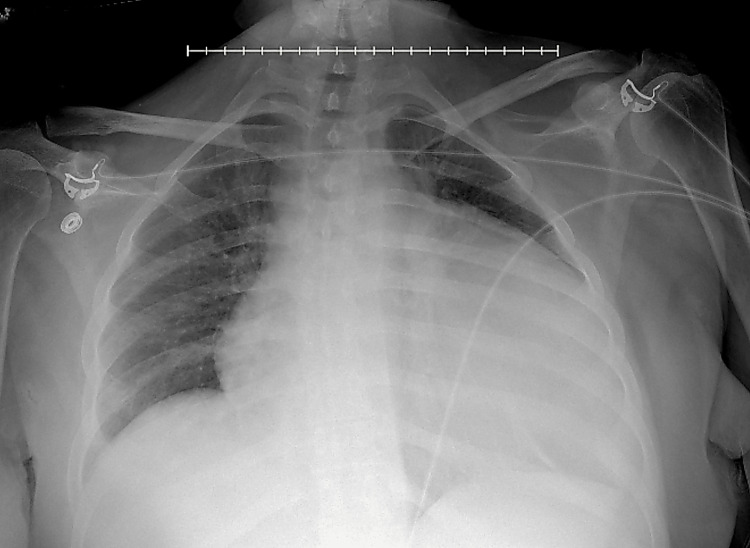 Figure 2
Figure 2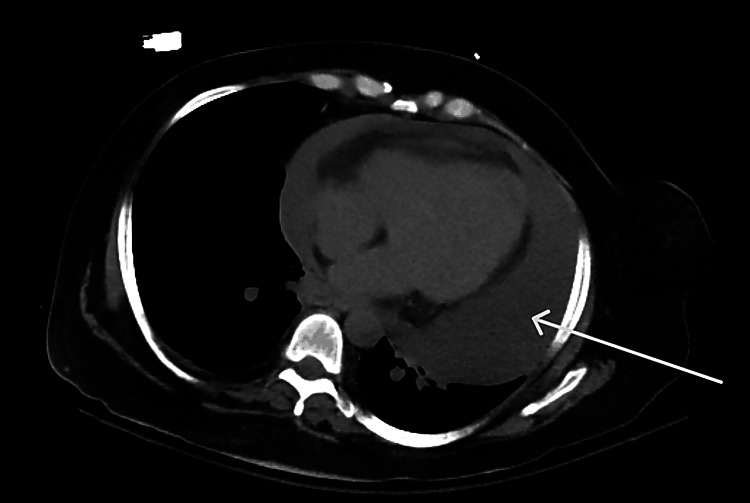 Figure 3
Figure 3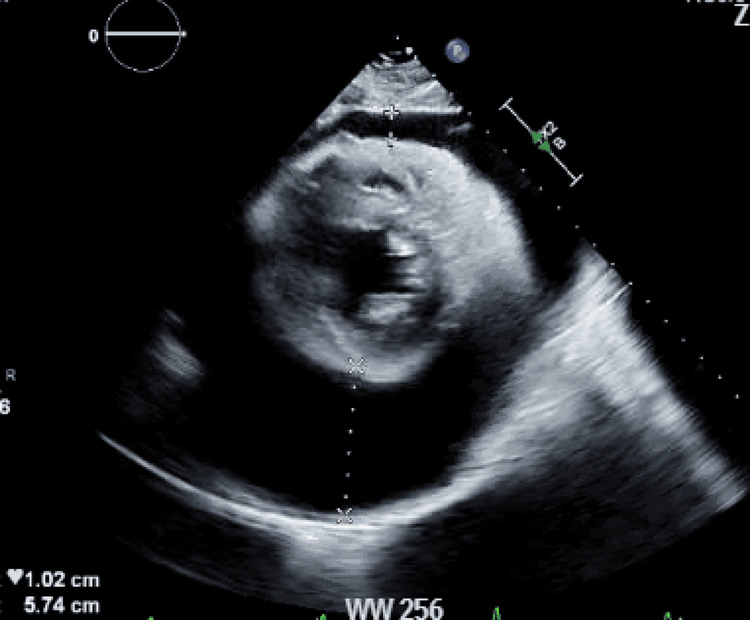 Figure 4
Figure 4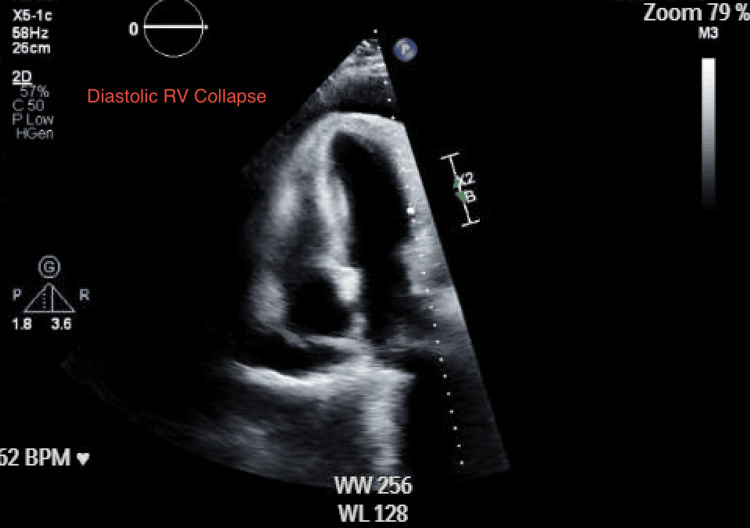 Figure 5
Figure 5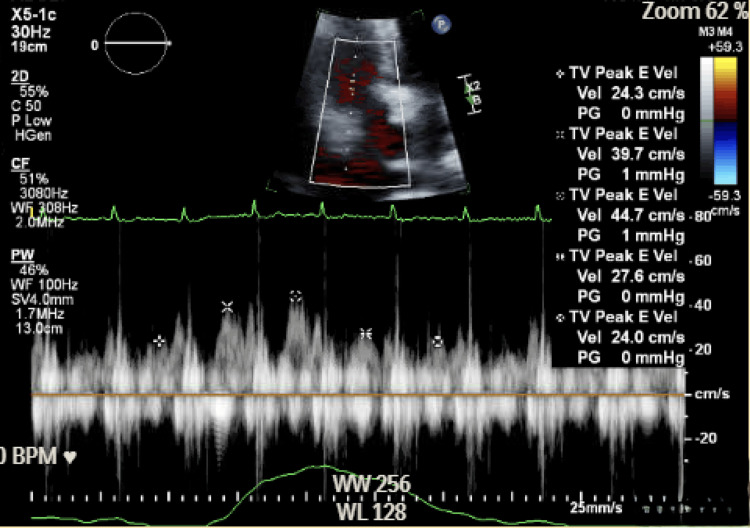 Figure 6
Figure 6| Test | Result | Units | Reference range |
| TSH | 65.04 | μIU/mL | 0.40-4.50 |
| Free T4 | <0.4 | ng/dL | 0.7-1.5 |
| Morning cortisol | 18.8 | mcg/dL | 10-20 |
| Pericardial fluid protein | 5.4 | g/dL | No universal normal |
| Pericardial fluid LDH | 84 | U/L | No universal normal |
| Pericardial fluid glucose | 75 | mg/dL | No universal normal |
| ANA | Negative | Negative | |
| Anti-Smith antibody | Negative | Negative | |
| Hepatitis B antibody | Negative | Negative | |
| Hepatitis C antibody | Negative | Negative |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPericarditis and Cardiac Tamponade · Myasthenia Gravis and Thymoma · Thyroid Disorders and Treatments
Introduction
Hypothyroidism has diverse cardiovascular manifestations, including sinus bradycardia, impaired diastolic function, and pericardial effusion [1]. Pericardial effusion is a recognized consequence of long-standing disease and often accumulates slowly enough to remain clinically silent until pericardial reserve is exceeded [1,2]. The pathophysiology involves increased capillary permeability, interstitial glycosaminoglycan deposition, and reduced lymphatic drainage, which favor gradual fluid accumulation [1]. Although large effusions are not uncommon in this setting, progression to hemodynamic compromise is relatively rare; when tamponade occurs, compensatory tachycardia may be attenuated because sympathetic tone and β-adrenergic responsiveness are blunted, a "myxedema heart" phenomenon that can obscure recognition at the bedside [2]. Classically, tamponade presents with hypotension, elevated venous pressures, and reflex tachycardia (often with pulsus paradoxus), reflecting impaired diastolic filling; however, these bedside cues may be muted in severe hypothyroidism, making imaging pivotal [3].
Diagnosis relies on echocardiography demonstrating tamponade physiology [3,4], and management centers on urgent pericardial drainage with subsequent thyroid hormone replacement to address the underlying disorder and reduce the risk of recurrence [5-7]. This framework emphasizes that heart rate alone is an unreliable discriminator in myxedema-associated tamponade and that timely imaging-guided intervention with coordinated endocrine care is essential [8].
Case presentation
A 50-year-old woman with a long-standing history of hypothyroidism, who had not been taking her thyroid medication for years, presented with progressive dyspnea and fatigue. On arrival, blood pressure was 82/60 mmHg and heart rate 60 beats/min; examination was notable only for mild lower extremity edema. Pulsus paradoxus was not formally assessed. Laboratory testing confirmed severe hypothyroidism: thyroid-stimulating hormone (TSH) 65.04 μIU/mL (0.40-4.50) and free T4 <0.4 ng/dL (0.7-1.5). Triiodothyronine and thyroid peroxidase antibodies were not obtained. Electrocardiography showed a normal sinus rhythm with low-voltage QRS complexes (Figure 1). Chest radiography demonstrated an enlarged cardiac silhouette (Figure 2), and abdominal/pelvic CT incidentally identified a large pericardial effusion (Figure 3).
Twelve-lead electrocardiogram demonstrating normal sinus rhythm with low-voltage QRS complexes.
Portable AP chest radiograph demonstrating an enlarged cardiac silhouette.AP: anteroposterior
Axial CT scan (lower thoracic cut) showing a circumferential low attenuation surrounding the heart (arrow), compatible with a large pericardial effusion.
Urgent transthoracic echocardiography revealed a large circumferential effusion with a swinging heart (Figure 4), right ventricular diastolic collapse (Figure 5), and marked respiratory variation of tricuspid inflow (Figure 6; approximately 46% respiratory variation in tricuspid E-wave peak velocity, 44.7 to 24 cm/s), with a plethoric inferior vena cava without respiratory variation, consistent with tamponade physiology. Endocrinology, cardiology, and thoracic surgery were consulted. The patient received intravenous fluids and stress-dose hydrocortisone 100 mg for empiric adrenal coverage during the initiation of intravenous levothyroxine, as thyroid hormone replacement can increase cortisol clearance and unmask occult adrenal insufficiency; glucocorticoids were discontinued after a reassuring morning cortisol (18.8 mcg/dL). She then underwent echo-guided emergent pericardiocentesis with the removal of three liters of straw-colored fluid; a pericardial catheter was left to gravity drainage and removed on hospital day 5 after declining output and imaging improvement.
Transthoracic echocardiography showing circumferential anechoic space consistent with pericardial effusion.
Transthoracic echocardiography showing early diastolic RV free-wall collapse consistent with tamponade physiology.RV: right ventricular
Doppler echocardiography showing marked tricuspid inflow respiratory variation supporting tamponade physiology.
Pericardial fluid analysis showed protein 5.4 g/dL, lactate dehydrogenase (LDH) 84 U/L, and glucose 75 mg/dL; cultures and cytology were negative, supporting a noninfectious, nonmalignant profile. Although Light's criteria are widely used for pleural effusions, they are not validated for pericardial fluid and may misclassify pericardial effusions; interpretation should rely on clinical context with cultures and cytology. Concurrent serum protein and LDH were not obtained; therefore, serum-to-fluid ratios could not be calculated. Screening serologies were limited but negative (antinuclear antibody and anti-Smith), as were hepatitis B and C antibodies; liver, renal, and adrenal function were normal, together favoring hypothyroidism as the etiology by exclusion. Key laboratory values and reference ranges are summarized in Table 1. Thyroid replacement was initiated with intravenous levothyroxine 200 μg daily for three doses, followed by oral levothyroxine 125 μg daily; intravenous therapy was used short-term to ensure reliable replacement in critical illness with hemodynamic instability, and the patient had no altered mental status or myxedema coma. Hemodynamics normalized, symptoms improved, and follow-up echocardiography showed only a minimal residual effusion without tamponade physiology.
Discussion
Pericardial effusion is a known manifestation of long-standing hypothyroidism, typically accumulating slowly and permitting very large volumes before pericardial reserve is exceeded [1,2]. While large effusions may develop in myxedema due to gradual accumulation, the three-liter volume drained in our patient is exceptional and highlights how prolonged untreated hypothyroidism can allow extreme pericardial fluid accumulation before clinical decompensation.
Severe hypothyroidism blunts sympathetic tone and β-adrenergic responsiveness, so the compensatory tachycardia seen in other tamponade etiologies may be attenuated, yielding bradycardic tamponade and a potential diagnostic pitfall [1,2,8]. Echocardiography remains central to diagnosis: large effusion with respiratory variation of atrioventricular (AV) valve inflow (≈≥25% mitral; ≥40% tricuspid) or right-sided chamber collapse with a plethoric inferior vena cava supports tamponade physiology [3,4]. In our patient, the combination of a large circumferential effusion and marked inflow variation prompted definitive drainage. Rapid evacuation of large pericardial effusions carries a recognized risk of pericardial decompression syndrome (PDS), a rare but potentially serious complication characterized by acute ventricular dysfunction and pulmonary edema following drainage, particularly in cases of massive, chronic effusions [5].
Assigning etiology requires a structured exclusion: infection and malignancy are addressed via cultures/cytology; biochemical panels (protein, LDH, glucose) help characterize the fluid while recognizing that conventional transudate/exudate cutoffs (Light's criteria) do not reliably apply to pericardial effusions [3]. Screening for autoimmune or viral causes should be tailored; our limited serologies (antinuclear antibody, anti-Smith, hepatitis B and C antibodies) were negative, and there were no clinical stigmata of connective tissue disease, making myxedema-related effusion most likely in the context of profound hypothyroidism [3]. Therapeutically, urgent pericardiocentesis with short-term catheter drainage is indicated when tamponade physiology is present, accompanied by careful endocrine management with adrenal coverage when appropriate and levothyroxine replacement (intravenous loading in critical illness followed by oral maintenance) [6-8]. These steps typically lead to rapid hemodynamic recovery and prevent recurrence as euthyroidism is restored.
Conclusions
Severe, untreated hypothyroidism can cause massive pericardial effusion and, rarely, tamponade. In this setting, the expected reflex tachycardia of tamponade may be absent due to blunted sympathetic tone ("myxedema heart"), making reliance on bedside heart rate potentially misleading. Echocardiography is therefore pivotal to confirm tamponade physiology and guide urgent pericardial drainage, followed by thyroid hormone replacement to treat the underlying cause and reduce recurrence risk.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Thyroid disease and the heart Circulation Klein I Danzi S 1725173511620071792358310.1161/CIRCULATIONAHA.106.678326 · doi ↗ · pubmed ↗
- 2Hypothyroidism-related cardiac tamponade Cureus Kaur H Chakwop Ngassa H Elmenawi KA Anil V Gosal H Mohammed L 013202110.7759/cureus.18611 PMC 858010934786222 · doi ↗ · pubmed ↗
- 32015 ESC guidelines for the diagnosis and management of pericardial diseases: the task force for the diagnosis and management of pericardial diseases of the European Society of Cardiology (ESC) endorsed by: the European Association for Cardio-Thoracic Surgery (EACTS)Eur Heart J Adler Y Charron P Imazio M 292129643620152632011210.1093/eurheartj/ehv 318PMC 7539677 · doi ↗ · pubmed ↗
- 42015 ESC guidelines for pericardial disease ACC.org American College of Cardiology. 2015 https://www.acc.org/latest-in-cardiology/ten-points-to-remember/2015/10/30/12/01/2015-esc-guidelines-for-the-diagnosis-and-management-of-pericardial-diseases
- 5Pericardial decompression syndrome in a patient with hypothyroidism presenting as massive pericardial effusion: a case report and review of related literature BMJ Case Rep Lim AS Paz-Pacheco E Reyes M Punzalan F 02011201110.1136/bcr.04.2011.4117 PMC 318964622679149 · doi ↗ · pubmed ↗
- 6Guidelines for the treatment of hypothyroidism: prepared by the American Thyroid Association task force on thyroid hormone replacement Thyroid Jonklaas J Bianco AC Bauer AJ 167017512420142526624710.1089/thy.2014.0028 PMC 4267409 · doi ↗ · pubmed ↗
- 7Echo-guided pericardiocentesis: when and how should it be performed?Curr Cardiol Rep Flint N Siegel RJ 712220203257259410.1007/s 11886-020-01320-2 · doi ↗ · pubmed ↗
- 8Echo-guided pericardiocentesis: let the bubbles show the way Circulation Ainsworth CD Salehian O 01123201110.1161/CIRCULATIONAHA.110.00551221282518 · doi ↗ · pubmed ↗