Solid Biomass Fuel Use and Respiratory Health Among Women and Children in South Asian Countries: A Systematic Review and Meta-Analysis
Kulumina Dash, Sasmita Nayak, Kripalini Patel, Milinda Mishra, Pratap K Jena, Krushna Chandra Sahoo

TL;DR
Using solid biomass fuels for cooking increases respiratory infections in women and young children in South Asia, according to a review and meta-analysis.
Contribution
This study provides the first systematic review and meta-analysis on biofuel use and respiratory health in South Asian populations.
Findings
Women using unimproved fuels had 23.3% prevalence of respiratory infections, compared to 8% with improved fuels.
Children in households using unimproved fuels had 26.4% higher acute respiratory infections than those with improved fuels.
Switching to improved cooking fuels significantly reduces the risk of chronic and acute respiratory infections.
Abstract
The use of biofuels for cooking in households has been associated with an increased risk of respiratory infections, particularly among women and children. However, there remains a dearth of systematic evidence regarding the respiratory health impacts of biofuel use in South Asian countries. This review aimed to compare the prevalence of respiratory infections among women and children under five years old in households using unimproved cooking fuels versus those using improved alternatives. Articles were systematically retrieved from the PubMed, Embase, and Web of Science databases. Pooled prevalence estimates were calculated through meta-analysis utilizing the random-effects model. From a pool of 4,190 identified articles, 86 full-text articles were scrutinized, leading to the inclusion of 36 studies. Analysis revealed a notably higher prevalence of respiratory infections among…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
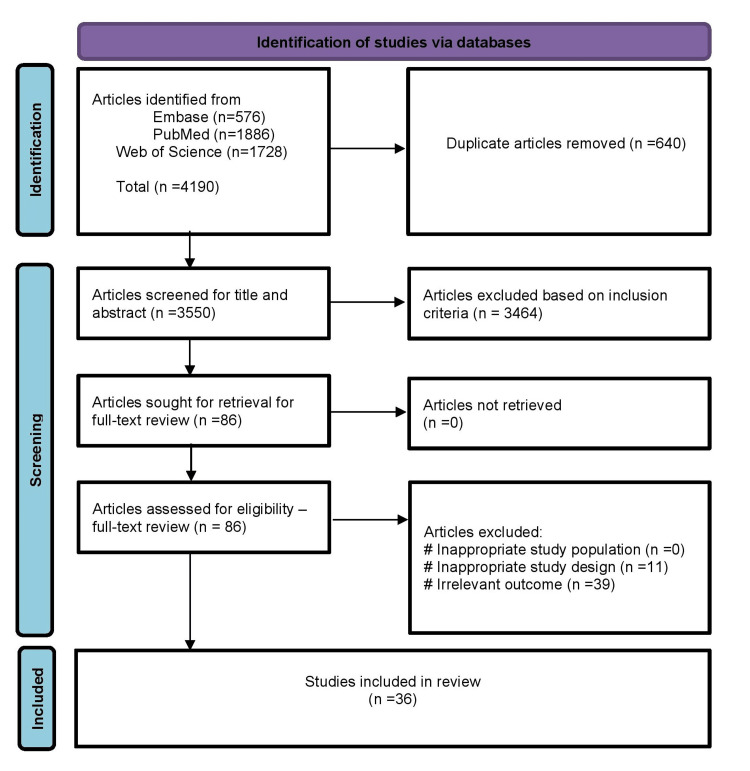 Figure 1
Figure 1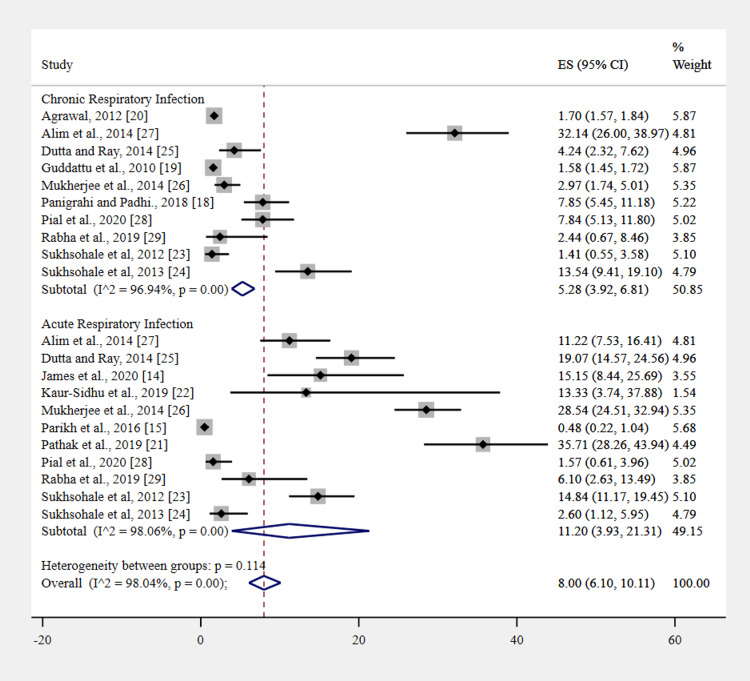 Figure 2
Figure 2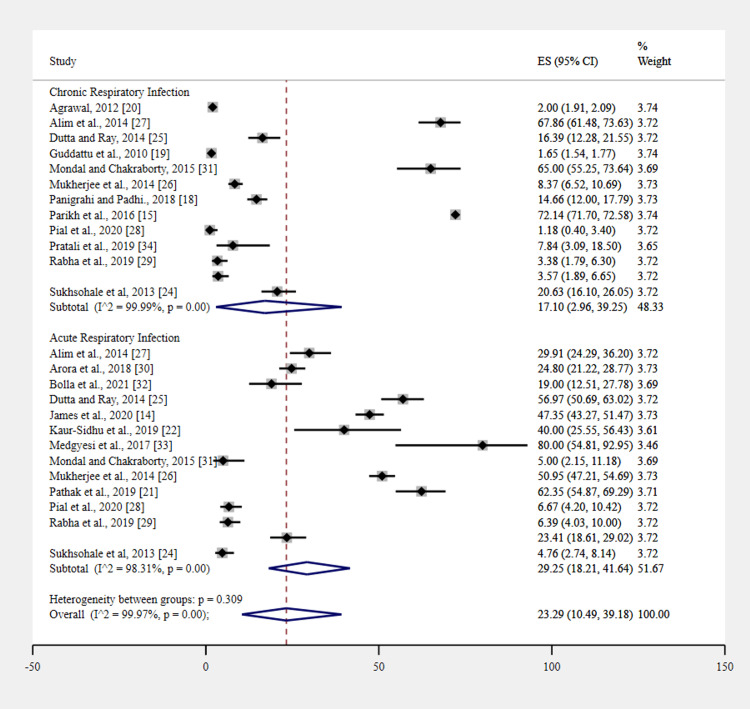 Figure 3
Figure 3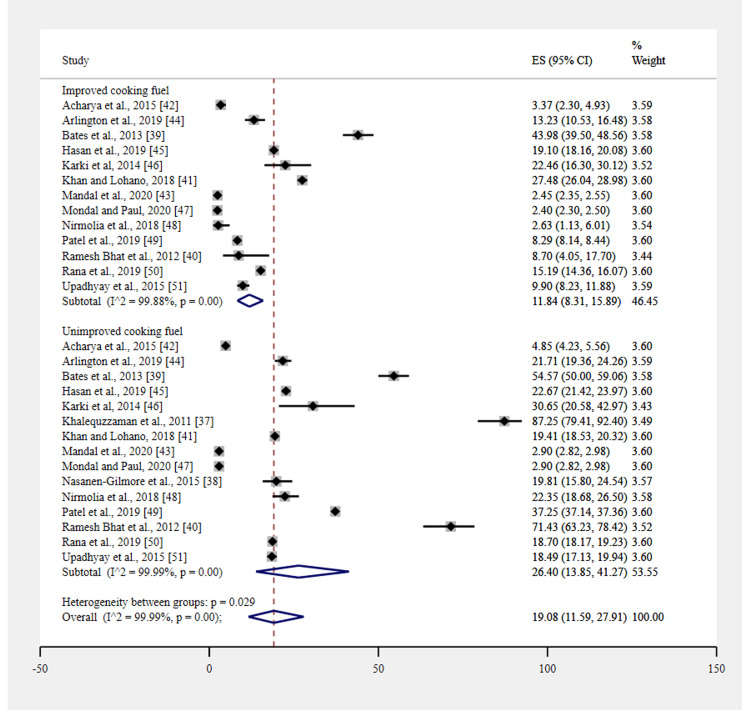 Figure 4
Figure 4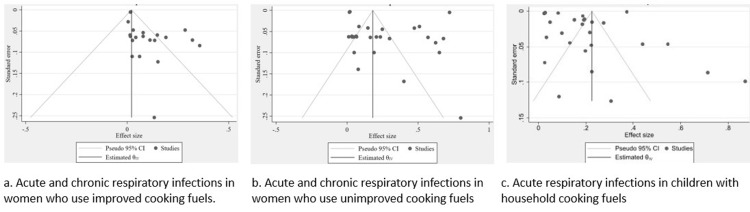 Figure 5
Figure 5| Author, year | State | Country | Study design | Settings | Age in years | Total women | Women with improved fuel | Women with unimproved fuel | Chronic respiratory infection among improved fuel users | Chronic respiratory infection among unimproved fuel users | Acute respiratory infection among improved fuel users | Acute respiratory infection in unimproved fuel users |
|
James et al., 2020 [ | Manipal | India | Community-based cross-sectional | Rural | 18+ | 632 | 66 | 566 | Not available | Not available | 10 | 268 |
|
Parikh et al., 2016 [ | Rajasthan | India | Large survey | Rural | 15+ | 41,965 | 1,259 | 40,706 | 12,589 | 29,366 | 6 | Not available |
|
Panigrahi and Padhi, 2018 [ | Odisha | India | Community-based cross-sectional | Rural | 18-49 | 917 | 344 | 573 | 27 | 84 | Not available | Not available |
|
Guddattu et al., 2010 [ | Not available | India | Large survey | Rural | 15-49 | 85,699 | 34,870 | 50,829 | 551 | 839 | Not available | Not available |
|
Agrawal, 2012 [ | Not available | India | Large survey | Both | 20-49 | 124,385 | 37,067 | 87,318 | 630 | 1,746 | Not available | Not available |
|
Pathak et al., 2019 [ | Uttar Pradesh | India | Community-based cross-sectional | Rural | 18–40 | 310 | 140 | 170 | Not available | Not available | 50 | 106 |
|
Kaur-Sidhu et al., 2019 [ | Punjab | India | Community-based cross-sectional | Rural | 30-60 | 50 | 15 | 35 | Not available | Not available | 2 | 14 |
|
Sukhsohale et al., 2012 [ | Nagpur | India | Community-based cross-sectional | Rural | 15+ | 535 | 283 | 252 | 4 | 9 | 42 | 59 |
|
Sukhsohale et al., 2013 [ | Nagpur | India | Community-based cross-sectional | Rural | 15+ | 444 | 192 | 252 | 26 | 52 | 5 | 12 |
|
Dutta and Ray, 2014 [ | West Bengal | India | Community-based cross-sectional | Rural | 22-41 | 480 | 236 | 244 | 10 | 40 | 45 | 139 |
|
Mukherjee et al., 2014 [ | West Bengal | India | Community-based cross-sectional | Rural | 23–43 | 1,119 | 438 | 681 | 13 | 57 | 125 | 347 |
|
Alim et al., 2014 [ | Bogra | Bangladesh | Community-based cross-sectional | Rural | 15-58 | 224 | Not available | 224 | Not available | 152 | Not available | 67 |
| Urban | 15-58 | 196 | 196 | Not available | 63 | Not available | 22 | Not available | ||||
|
Pial et al., 2020 [ | Sylhet | Bangladesh | Community-based cross-sectional | Rural | 18+ | 510 | Not available | 255 | Not available | 3 | Not available | 17 |
| Urban | 18+ | 510 | 255 | Not available | 20 | Not available | 4 | Not available | ||||
|
Rabha et al., 2019 [ | Assam | India | Community-based cross-sectional | Rural | 18–55 | 266 | Not available | 266 | Not available | 9 | Not available | 17 |
| Urban | 18–55 | 82 | 82 | Not available | 2 | Not available | 5 | Not available | ||||
|
Arora et al., 2018 [ | Delhi | India | Community-based cross-sectional | Urban | 15-59 | 500 | Not available | 500 | Not available | Not available | Not available | 124 |
|
Mondal and Chakraborty, 2015 [ | West Bengal | India | Community-based cross-sectional | Rural | 26-39 | 100 | Not available | 100 | Not available | 65 | Not available | 5 |
|
Bolla et al., 2021 [ | Tamilnadu | India | Community-based cross-sectional | Rural | 18+ | 100 | Not available | 100 | Not available | Not available | Not available | 19 |
|
Medgyesi et al., 2017 [ | Dhaka | Bangladesh | Community-based cross-sectional | Rural | 18-65 | 15 | Not available | 15 | Not available | Not available | Not available | 12 |
|
Pratali et al., 2019 [ | Khumbu | Nepal | Case-control | Rural | 16-75 | 51 | Not available | 51 | Not available | 4 | Not available | Not available |
|
Adhikari et al., 2020 [ | Western Nepal | Nepal | Community-based cross-sectional | Urban | 40+ | 661 | 424 | 237 | Not available | 228 | Not available | Not available |
|
Johnson et al., 2011 [ | Tamilnadu | India | Community-based cross-sectional | Rural | 30+ | 900 | 147 | 753 | Not available | Not available | Not available | Not available |
| Authors, year | Country | Study design | Settings | Total children | Age in years | Children with improved cooking fuel | Improved acute respiratory infection | Children with unimproved cooking fuel | Unimproved acute respiratory infection |
| Khalequzzaman et al., 2011 [ | Bangladesh | Cross-sectional | Both | 102 | 0-5 | Not available | Not available | 102 | 89 |
| Nasanen-Gilmore et al., 2015 [ | Bangladesh | Cross-sectional | Rural | 321 | 0-5 | Not available | Not available | 318 | 63 |
| Bates et al., 2013 [ | Nepal | Case-control | Urban | 917 | 2-3 | 457 | 201 | 460 | 251 |
| Ramesh Bhat et al., 2012 [ | India | Case-control | Rural | 202 | 0-5 | 69 | 6 | 133 | 95 |
| Khan and Lohano, 2018 [ | Pakistan | Cross-sectional | Both | 11,040 | 0-5 | 3,533 | 971 | 7,507 | 1,457 |
| Acharya et al., 2015 [ | Nepal | Cross-sectional | Both | 4,802 | 0-5 | 741 | 25 | 4,061 | 197 |
| Mandal et al., 2020 [ | India | Cross-sectional | Both | 247,743 | 0-5 | 88,667 | 2,172 | 159,075 | 4,613 |
| Arlington et al., 2019 [ | India | Prospective | Rural | 1,586 | 0-0.5 | 499 | 66 | 1,087 | 236 |
| Hasan et al., 2019 [ | Bangladesh | Cross-sectional | Urban | 10,575 | 0-5 | 6,402 | 1,223 | 4,173 | 938 |
| Karki et al., 2014 [ | Nepal | Case-control | Both | 200 | 0-5 | 138 | 31 | 62 | 19 |
| Mondal and Paul, 2020 [ | India | Cross-sectional | Both | 247,743 | 0-5 | 86,225 | 2,069 | 161,528 | 4,684 |
| Nirmolia et al., 2018 [ | India | Cross-sectional | Urban | 624 | 1-5 | 190 | 5 | 434 | 97 |
| Patel et al., 2019 [ | India | Cross-sectional | Both | 932,341 | 0-5 | 125,231 | 10,379 | 807,110 | 300,645 |
| Rana et al., 2019 [ | Afghanistan | Cross-sectional | Both | 27,565 | 0-5 | 6,799 | 1,033 | 20,766 | 3,883 |
| Upadhyay et al., 2015 [ | India | Cohort | Both | 3,961 | 0-5 | 1,030 | 102 | 2,931 | 542 |
| Author, year | Inclusion in the sample clearly defined | Study subjects and the setting described in detail | Exposure measured in a valid and reliable way | Objective, standard criteria used for measurement of the condition | Confounding factors identified | Strategies to deal with confounding factors | Outcomes measured in a valid and reliable way | Appropriate statistical analysis |
| James et al., 2020 [ | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Parikh et al., 2016 [ | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Panigrahi and Padhi, 2018 [ | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Guddattu et al., 2010 [ | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Agrawal, 2012 [ | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Pathak et al., 2019 [ | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Kaur-Sidhu et al., 2019 [ | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Sukhsohale et al., 2012 [ | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Sukhsohale et al., 2013 [ | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Dutta and Ray, 2014 [ | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Mukherjee et al., 2014 [ | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Alim et al., 2014 [ | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Pial et al., 2020 [ | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Rabha et al., 2019 [ | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Arora et al., 2018 [ | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Mondal and Chakraborty, 2015 [ | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Bolla et al., 2021 [ | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Medgyesi et al., 2017 [ | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Pratali et al., 2019 [ | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Adhikari et al., 2020 [ | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Johnson et al., 2011 [ | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Khalequzzaman et al., 2011 [ | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Nasanen-Gilmore et al., 2015 [ | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Bates et al., 2013 [ | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Ramesh Bhat et al., 2012 [ | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Khan and Lohano, 2018 [ | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Acharya et al., 2015 [ | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Mandal et al., 2020 [ | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Arlington et al., 2019 [ | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Hasan et al., 2019 [ | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Karki et al., 2014 [ | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Mondal and Paul, 2020 [ | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Nirmolia et al., 2018 [ | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Patel et al., 2019 [ | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Rana et al., 2019 [ | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Upadhyay et al., 2015 [ | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsEnergy and Environment Impacts · Air Quality and Health Impacts · Indoor Air Quality and Microbial Exposure
Introduction and background
Biomass fuel serves as the primary domestic energy source for nearly one-third of the global population, underscoring its widespread significance [1]. However, its utilization for household cooking is accompanied by a substantial contribution to indoor air pollution (IAP), affecting over four million people annually worldwide [2]. Approximately 2.4 billion individuals inhabit households reliant on solid biomass fuels for cooking and heating, with an additional 0.6 billion depending on coal [3]. Within these households, levels of PM10 and PM2.5 often surpass recommended guidelines for mean 24-hour concentration, with cooking activities exacerbating these hazardous levels [4].
Beyond statistical figures, the ramifications of biomass fuel dependence are profound. IAP emerges as a significant environmental risk factor, accounting for 5% of all women's deaths annually in developing countries due to respiratory infections [5]. Projections from the International Energy Agency (IEA) forecast that by 2030, one billion individuals will still lack access to electricity, while 2.6 billion will continue to lack access to clean cooking fuel [6]. Presently, approximately 2.5 billion people worldwide rely on biomass fuels for cooking, heating, and lighting, including materials like manure, wood, agricultural residues, and coal [7]. This reliance is particularly pronounced in Africa, where over 500 million people (78% of the population) employ biomass fuel for cooking and heating [8,9]. Similarly, South Asia, encompassing countries such as India, Bangladesh, Pakistan, Nepal, Sri Lanka, and Bhutan, witnesses extensive use of biomass fuels like wood, crop residues, and dung, particularly in rural settings [10-13].
Moreover, mounting evidence establishes a troubling association between biomass fuel exposure and respiratory ailments such as tuberculosis, chronic obstructive pulmonary disease (COPD), and lung cancer, significantly contributing to the global disease burden [13]. Women and children under five emerge as particularly vulnerable to IAP from these fuels, given their prolonged exposure near cooking fires [13]. In South Asia, where women traditionally assume household chores and cooking duties, they endure disproportionate exposure to IAP's detrimental effects due to extended proximity to smoke. Furthermore, commonly used biomass fuels emit various organic compounds such as benzene, formaldehyde, 1,3-butadiene, and polyaromatic hydrocarbons, further exacerbating health risks [14,15]. Notably, studies in India have linked IAP to a spectrum of health conditions, including 20% of ischemic heart disease (IHD), 23% of strokes, 45% of COPD cases, 21% of lung cancer cases, and 22% of acute respiratory tract infections (ARI) [15].
In South Asia, the confluence of household air pollution and biomass fuel utilization poses intricate and substantial health risks to women [16]. Given their primary role in cooking, women are predisposed to heightened exposure to household air contaminants. Furthermore, households reliant on biofuels are at an increased risk of respiratory infections. The predominant role of women in South Asia, revolving around cooking responsibilities, exacerbates this issue due to their prolonged proximity to pollution sources. Despite these realities, a systematic understanding of the health impacts of biofuel use on women and children in South Asian countries remains lacking. Hence, this comprehensive systematic review and meta-analysis aim to elucidate the health effects of solid biomass fuels on women and children under five in South Asian countries, seeking to inform policy changes and address this urgent concern.
Review
Methods
This systematic review was conducted according to the Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) guideline and registered in PROSPERO (http://www.crd.york.ac.uk/PROSPERO/) (CRD42021260063).
Databases and Search Strategies
We conducted independent searches on three online databases: PubMed, Embase, and Web of Science. To create a comprehensive search strategy, we used relevant keywords and MeSH terminology related to “Household Air Pollution” and “Respiratory Health Outcomes.” This strategy encompassed three major domains: “Household Air Pollution,” “Respiratory Health Outcomes,” and “South Asia.” We combined these domains and terms using the Boolean operator "AND” to create custom search queries tailored to each database's requirements and specifications.
Inclusion Criteria
The review centered on examining acute and chronic respiratory infections in women and children under the age of five within households that relied on unimproved (solid biomass) cooking fuels in South Asian countries, comparing them to households that used improved cooking fuels. We considered studies published in English between January 2010 and June 2021 for inclusion. The selected study types encompassed cross-sectional, case-control, cohort, longitudinal, case-cross-over, and intervention studies conducted in the South Asian region. Excluded from the review were editorial reports, review articles, and case reports.
Screening and Identification of Studies
Upon identifying all articles through searches, we imported them into reference management software (EndNote X8, Clarivate, London, UK) to remove duplicate entries. Following this, the records were transitioned to Rayyan (Rayyan Systems Inc., Cambridge, MA, US), where the initial screening involved reviewing titles and abstracts. The primary screening was carried out by three independent researchers. Subsequently, potentially pertinent studies underwent a comprehensive eligibility assessment during a full-text screening phase. Any discrepancies or disagreements among the authors were addressed through open discussion and mutual consensus.
Quality Assessment, Data Extraction, and Synthesis
This study employed the Joanna Briggs Institute (JBI) critical appraisal checklist [17], tailored for analytical cross-sectional studies, to evaluate the methodological rigor of the studies incorporated in this analysis. For the systematic data extraction of pertinent study details and outcomes, we employed a pre-designed and standardized data extraction form. Two authors autonomously collected relevant information using a Microsoft Excel spreadsheet (Microsoft Corporation, Redmond, WA, US), ensuring consistency and accuracy. Subsequently, the extracted data were cross-validated by another author to enhance reliability. The extraction parameters included information about the authors, the study design, the study location, the sample size, the publication year, the study period, the number of households that used improved and unimproved cooking fuels, and the number of acute respiratory and chronic infections among women and children under the age of five.
The meta-analysis was performed using a random-effects model to determine pooled prevalence among different subgroups. The models estimated the overall effect size and assessed study heterogeneity. Subgroup analysis and meta-regression were used to investigate sources of heterogeneity and evaluate how different study characteristics may influence the results. The results are presented in forest plots to help interpret the results by visualizing individual study effect sizes and the combined effect size. The funnel plots are used to determine whether or not there is publication bias.
Results
The initial search retrieved a total of 4,190 articles, which were subsequently reduced to 3,550 after eliminating duplicates. Following a meticulous review of titles and abstracts, 3,464 articles were excluded, primarily due to the study area being outside of South Asia or not aligning with the expected outcome. This left us with 86 articles that underwent a comprehensive full-text review. Ultimately, 36 studies were identified as meeting the inclusion criteria. For a visual representation of this process, please refer to Figure 1 in the detailed PRISMA flow diagram.
PRISMA flow diagram.PRISMA: Preferred Reporting Items for Systematic reviews and Meta-Analyses
The systematic review encompassed a total of 36 articles, with 21 focusing on women and 15 on children. Tables 1, 2, respectively, present detailed characteristics of the women participants and households with children under the age of five.
Regarding the women's studies [14,15,18-36], the majority consisted of community-based cross-sectional studies, while three were large-scale investigations, and one adopted a case-control study design. Predominantly, these studies were conducted in India, with an additional five from Bangladesh and two from Nepal. Most of the research was concentrated in rural areas, although four studies extended to both rural and urban settings, while only one study was exclusively conducted in urban areas.
Table 3 shows that all listed studies meet the JBI critical appraisal checklist for analytical cross-sectional studies, demonstrating comprehensive methodological quality across all evaluated domains. The study's inclusion, description of subjects, exposure measurement, objective criteria, identification of confounding factors, strategies to address them, outcome measurement validity, and appropriate statistical analysis are marked "yes." If further nuance is needed, per-study specifics or qualitative synthesis can be provided.
In the children's studies [37-51], the majority were cross-sectional, complemented by three case-control studies, one prospective study, and one cohort study. India featured prominently as the research location, with three studies in Nepal, three in Bangladesh, one in Pakistan, and one in Afghanistan. A significant portion of these studies encompassed both rural and urban areas, with three studies focusing exclusively on each of these settings.
Out of the 21 women's studies [14,15,18-36], five focused on the prevalence of respiratory infections among women who solely used unimproved cooking fuels, while 16 examined those who used both improved and unimproved fuels. Among women using improved fuels, three studies addressed chronic respiratory infections, four focused on acute respiratory infections, and seven explored both acute and chronic respiratory infections. Similarly, among women using unimproved fuels, five studies investigated chronic respiratory infections, six studied acute respiratory infections, and eight examined both acute and chronic respiratory infections. Among the 15 children's studies, only two examined the prevalence of acute respiratory infections in households using unimproved cooking fuel. The remaining 13 studies focused on acute respiratory infections in households that used both improved and unimproved cooking fuels.
The pooled prevalence of respiratory infections among women exposed to improved cooking fuel was 8% (95% CI 6.10-10.11; I² = 98.04%, P < 0.001). A subgroup analysis, classified by the type of respiratory infection, revealed a notable difference. Acute respiratory infections were higher at 11.20% (95% CI 3.93-21.31; I² = 98.06%, P < 0.001) compared to chronic respiratory infections, which stood at 5.28% (95% CI 3.92-6.81; I² = 96.94%, P < 0.001). Figure 2 depicts the forest plot describing acute and chronic respiratory infections in women who use improved cooking fuels.
Acute and chronic respiratory infections in women who use improved cooking fuels.
The pooled prevalence of respiratory infections among women exposed to unimproved cooking fuel was 23.29% (95% CI 10.49-39.18; I² = 99.97%, P < 0.001). Subgroup analysis, categorized by the type of respiratory infection, revealed that the prevalence of acute respiratory infection was higher at 29.25% (95% CI 18.21-41.67; I² = 98.31%, P < 0.001) than chronic respiratory infection at 17.10% (95% CI 2.96-39.25; I² = 99.99%, P < 0.001). Figure 3 depicts the forest plot describing acute and chronic respiratory infections in women who use unimproved cooking fuels.
Acute and chronic respiratory infections in women who use unimproved cooking fuels.
Figure 4 compares the prevalence of acute respiratory infections among children [37-51] living in households with and without improved cooking fuel practices. The overall prevalence was 19.08% (95% CI 11.59-27.91). The subgroup analysis revealed that the pooled prevalence was higher among children whose households used unimproved cooking fuel (26.40%, 95% CI 13.85-41.27) than among those whose households used improved cooking fuel (11.84%, 95% CI 8.31-15.54).
Acute respiratory infections in children with household cooking fuels (improved versus unimproved) using practices.
The publication bias of the results is presented in a funnel plot (Figure 5). Figure 5a shows acute and chronic respiratory infections in women who use improved cooking fuels, where the spread is moderate, indicating reasonable heterogeneity but not extreme. Figure 5b shows acute and chronic respiratory infections in women who use unimproved cooking fuels, where a wider dispersion of study estimates suggests greater heterogeneity. Figure 5c shows acute respiratory infections in children with household cooking fuels, where the distribution shows some asymmetry with more studies on one side, which may hint at potential small-study effects or contextual differences specific to child populations. There is notable between-study heterogeneity across all groups, with greater dispersion in Figures 5b, 5c.
(a-c) Funnel plot showing publication bias.
Discussion
The study identified a higher prevalence of respiratory infections among women and children in South Asia residing in households reliant on unimproved cooking fuel. Women exposed to unimproved fuel exhibited an increased likelihood of developing acute respiratory infections (29.2%) and chronic infections (17.1%). Similarly, a significant disparity in acute respiratory infections was observed among children. These findings underscore the imperative for strategic policy frameworks aimed at fostering the widespread adoption of clean cooking fuels, necessitating incentives, subsidies, and public awareness campaigns.
South Asia, grappling with the pervasive challenge of household air pollution stemming from cooking fuel usage and its associated respiratory infections, has witnessed concerted efforts through various initiatives. Notable among these is the Pradhan Mantri Ujjwala Yojana (PMUY), launched by the Indian government in May 2016. This scheme incentivizes the adoption of clean cooking fuels in rural India by subsidizing liquid petroleum gas (LPG) connections for rural households, which include a complimentary gas cylinder, regulator, and pipe [16]. In addition to the PMUY, similar programs have been implemented across other South Asian nations to advocate for cleaner cooking practices. The current implementation status of the PMUY in India demonstrates continued progress in expanding LPG access to rural and economically vulnerable households, with millions of new gas connections completed and a continued emphasis on beneficiary verification and policy refinements to prevent duplication and leakages. However, issues continue in guaranteeing a consistent fuel supply in remote areas, maintaining affordability in the face of growing LPG prices, and meeting ongoing demands for safe household energy practices and petrol cylinder safety. While administrative outreach and grievance redress mechanisms have improved, critical gaps in target accuracy, refill uptake consistency, and equitable benefits across states remain, highlighting the need for improved monitoring, strong supply chains, and complementary clean cooking energy initiatives to achieve universal clean cooking access.
In Bangladesh, the "Practical Action" program focuses on improving cookstoves and fosters community education about the benefits of cleaner cooking practices [52]. Meanwhile, Nepal's "National Improved Cook Stove Program" strives to replace traditional stoves with cleaner alternatives, emphasizing technological innovation and dissemination. Another noteworthy initiative in Nepal, the Urban Health Initiative (UHI), strives to mitigate household air pollution. In Sri Lanka, the "Sustainable Energy for All" (SE4ALL) initiative targets the reduction of household air pollution attributable to biomass fuel or unimproved fuels [53]. This initiative includes a component promoting clean cooking solutions, such as improved cookstoves and biogas systems, to diminish IAP and bolster health outcomes [54,55].
Nevertheless, challenges, including accessibility, affordability, behavioral change, and monitoring, impede the impact of PMUY and analogous programs in Bangladesh, Nepal, and Sri Lanka. Overcoming these hurdles is pivotal for the success of initiatives promoting clean cooking in South Asia. Addressing these challenges and fostering collaboration among governments, non-governmental organizations, and communities are essential for making substantial progress in reducing household air pollution and improving respiratory health. Investment in research and development holds promise for yielding efficient and affordable alternatives, thereby warranting further exploration of the impact of cleaner cooking fuels on health, the environment, and society.
Concurrently, there should be a prioritized focus on improving the accessibility of advanced cooking technologies, particularly in remote and marginalized areas. The effective implementation of policies necessitates robust monitoring and evaluation mechanisms [32-42]. A thorough, long-term assessment of intervention impacts on respiratory health outcomes and indoor air quality is crucial for informed decision-making and course adjustments. Collaborative efforts across various sectors, including health, energy, environment, and gender, are indispensable for the comprehensive implementation of policies. Coordinated actions between sectors can amplify the effectiveness of interventions and ensure a holistic approach to addressing the issue [44-47]. To effectively mitigate the grave threat of household air pollution in South Asia, comprehensive and effective policies are imperative, necessitating coordinated actions and investments among countries and extending policymakers' focus into additional sectors such as small manufacturing, agriculture, residential cooking, and waste management.
The study has inherent limitations that warrant consideration when interpreting results. Variability in study design, population, and outcome measures among the included studies may limit result generalizability. Unaccounted factors may influence respiratory infection risk in South Asian women and children. Nevertheless, the study's strengths lie in its comprehensive systematic review and meta-analysis, offering a robust summary of evidence on the link between solid biomass fuel use and respiratory health outcomes in South Asian countries. The findings provide valuable insights into the potential impact of interventions promoting improved cooking fuels and technologies on respiratory health outcomes.
Conclusions
The findings underscore the urgent need to advocate for improved cooking fuels and technologies to mitigate the heightened risk of respiratory infections among women and children in South Asian nations. It implies that prioritizing interventions aimed at promoting cleaner cooking fuels and technologies is imperative for enhancing respiratory health outcomes in these communities. Public health authorities in South Asian countries must prioritize such interventions to effectively reduce the prevalence of respiratory infections and safeguard the health of women and children.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1A review of diseases associated with household air pollution due to the use of biomass fuels J Hazard Mater Kim KH Jahan SA Kabir E 4254311922011 https://doi.org/10.1016/j.jhazmat.2011.05.0872170514010.1016/j.jhazmat.2011.05.087 · doi ↗ · pubmed ↗
- 2The Global Impact of Respiratory Disease Forum of International Respiratory Societies Sheffield European Respiratory Society 2017 https://static.physoc.org/app/uploads/2019/04/22192917/The_Global_Impact_of_Respiratory_Disease.pdf
- 3Respiratory disease associated with solid biomass fuel exposure in rural women and children: systematic review and meta-analysis Thorax Po JY Fitz Gerald JM Carlsten C 2322396620112124832210.1136/thx.2010.147884 · doi ↗ · pubmed ↗
- 4Indoor air pollution in developing countries: a major environmental and public health challenge Bull World Health Organ Bruce N Perez-Padilla R Albalak R 10781092782000 https://iris.who.int/handle/10665/26821811019457 PMC 2560841 · pubmed ↗
- 5Solid fuel use for household cooking: country and regional estimates for 1980-2010 Environ Health Perspect Bonjour S Adair-Rohani H Wolf J 78479012120132367450210.1289/ehp.1205987 PMC 3701999 · doi ↗ · pubmed ↗
- 6World Energy Outlook Birol F 329Paris International Energy Agency 232008 https://iea.blob.core.windows.net/assets/89d 1f 68c-f 4bf-4597-805f-901cfa 6ce 889/weo 2008.pdf
- 7Clean cooking and the SD Gs: integrated analytical approaches to guide energy interventions for health and environment goals Energy Sustain Dev Rosenthal J Quinn A Grieshop AP Pillarisetti A Glass RI 1521594220182986157510.1016/j.esd.2017.11.003PMC 5975963 · doi ↗ · pubmed ↗
- 8Household Energy Access for Cooking and Heating: Lessons Learned and the Way Forward World Bank Publications Ekouevi K Tuntivate V Washington, D.C.World Bank 232012 https://openknowledge.worldbank.org/entities/publication/30a 88758-091c-5c 99-9489-d 2fd 6b 3bf 889